Page 2 of 29
EN4.12 | Acoustic Neuroma — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The diagnosis of acoustic neuroma is established by the combination of clinical features (unilateral SNHL + tinnitus ± vestibular symptoms), audiological evidence of retrocochlear pattern (rollover on speech audiometry, absent stapedial reflex, prolonged ABR wave V), and confirmed by contrast-enhanced MRI showing an enhancing mass in the IAC/CPA. Histological confirmation is obtained only when surgery is performed; the MRI appearance is sufficiently characteristic that diagnosis without surgery is standard practice in the absence of atypical features.
The diagnostic approach is pattern recognition: the combination of a slowly progressive unilateral SNHL, unilateral tinnitus, and audiological evidence of retrocochlear dysfunction in a patient aged 30–60 is acoustic neuroma until MRI proves otherwise. The key clinical habit is not to dismiss these symptoms as 'normal ageing' or 'stress-related' — asymmetric SNHL demands imaging regardless of the patient's age or apparent cause.
Differential diagnosis of CPA tumours:
The CPA contains several important structures and can be the site of multiple different tumour types. The differential diagnosis is most efficiently structured by MRI appearance, comparing the epicentre, enhancement pattern, relationship to the IAC, and associated clinical features of each entity:
| Tumour | Frequency | Key MRI/Clinical features |
|---|---|---|
| Acoustic neuroma (vestibular schwannoma) | ~80% of CPA tumours | Enhancing mass centred on IAC, ice-cream cone sign; SNHL + tinnitus |
| Meningioma | ~10–15% | Broad-based dural attachment, calcification common, no IAC widening; may not cause SNHL early |
| Epidermoid cyst | ~5% | 'Cauliflower' shape, restricted diffusion on DWI, no enhancement; may cause trigeminal neuralgia |
| Facial nerve schwannoma | Rare | Identical appearance to acoustic neuroma but centred on facial nerve canal; facial palsy prominent early |
| Arachnoid cyst | Rare | CSF signal, no enhancement, no mass effect |
Key distinguishing features of acoustic neuroma from meningioma (the most important differential):
- Acoustic neuroma: epicentre at porous acusticus, IAC widening (bony erosion of IAC), acute angle with petrous bone, SNHL prominent
- Meningioma: broad dural base ('en plaque'), calcification, obtuse angle with petrous bone, may have hyperostosis, hearing loss less prominent
Non-tumour differentials for unilateral SNHL:
Before diagnosing acoustic neuroma, consider:
- Meniere's disease: episodic vertigo + low-frequency fluctuating SNHL + tinnitus + aural fullness — the hearing loss fluctuates rather than progressing unidirectionally, and MRI is normal
- Sudden sensorineural hearing loss (SSNHL): acute onset over hours; most cases are idiopathic; some are caused by acoustic neuroma (6–15% of SSNHL cases have an acoustic neuroma on MRI — hence MRI is recommended in all SSNHL)
- Presbyacusis: bilateral, symmetric, gradual — does not explain unilateral asymmetric loss
- Noise-induced hearing loss: bilateral, notch at 4 kHz, history of noise exposure
SELF-CHECK
On MRI with gadolinium, an enhancing mass is found centred on the left internal auditory canal with extension into the CPA, creating an 'ice-cream cone' appearance. There is erosion of the porous acusticus. The adjacent dura is flat and normal. The most likely diagnosis is:
A. Meningioma of the posterior fossa
B. Acoustic neuroma (vestibular schwannoma)
C. Epidermoid cyst
D. Facial nerve schwannoma
Reveal Answer
Answer: B. Acoustic neuroma (vestibular schwannoma)
The 'ice-cream cone' appearance (intracanalicular cone + CPA ball) with an enhancing mass centred on the IAC and bony erosion of the porous acusticus is the classic MRI signature of acoustic neuroma. Meningioma has a broad dural base, calcification, and does NOT widen the IAC. Epidermoid cysts show restricted diffusion on DWI and do not enhance with gadolinium. Facial nerve schwannoma is identical in appearance but rare and would have an epicentre on the facial nerve canal (geniculate ganglion/horizontal canal), not the vestibular nerve.
Principles of Management
Three treatment strategies are available for acoustic neuroma: observation (wait-and-scan), stereotactic radiosurgery, and microsurgical excision. The choice depends on tumour size, rate of growth, degree of hearing loss, patient age and fitness, and patient preference. No single option is universally best — the decision is individualised.
1. Observation (Watch-and-Wait / Wait-and-Scan)
Indications: small tumour (<1.5 cm), elderly or medically unfit patient, preserved hearing, or slow/absent growth on serial MRI. Approximately 40–50% of acoustic neuromas show no growth over 5 years; these patients may be managed indefinitely with observation. The protocol involves MRI every 6 months for 2 years, then annually if stable. Observation is abandoned if the tumour shows growth, symptoms worsen, or the patient requests treatment. The main disadvantage is the risk of tumour growth that may ultimately make hearing-preservation surgery impossible.
2. Stereotactic Radiosurgery (Gamma Knife / CyberKnife / LINAC)
Indications: small-to-medium tumours (generally ≤3 cm, no significant brainstem compression), older patients, or those refusing microsurgery. The principle is focused ionising radiation to the tumour volume in a single session (Gamma Knife) or fractionated sessions, causing tumour growth arrest through DNA damage and vascular occlusion — not tumour removal. Long-term tumour control rates are ~90–95% over 10 years. Hearing may be preserved in 50–60% of patients with useful pre-treatment hearing. Risks include delayed cranial nerve effects (V, VII palsy in 1–5% of cases) and very rare radiation-induced malignancy. Radiosurgery does NOT provide a tissue diagnosis and is less effective for large tumours.
3. Microsurgical Excision
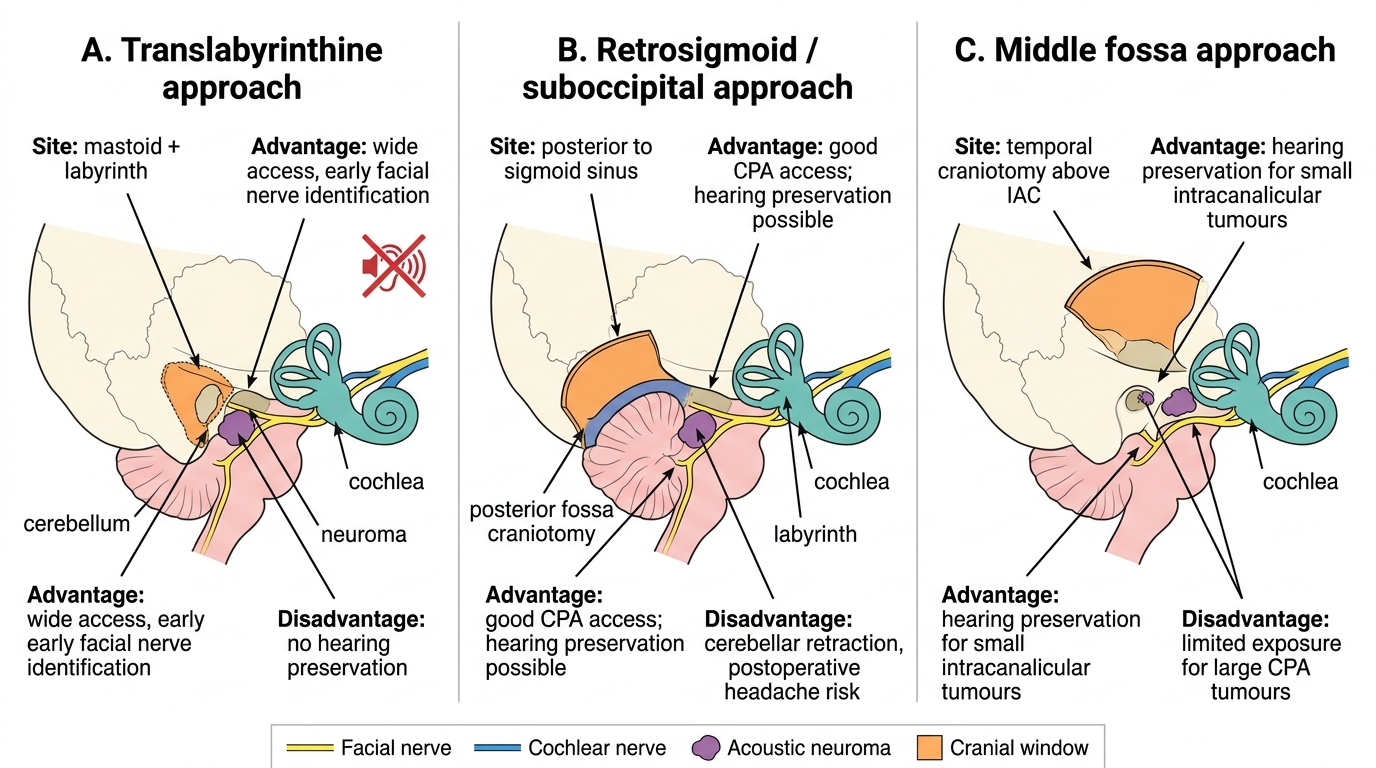
The surgical approaches are:
| Approach | Route | Hearing preservation | Best for |
|---|---|---|---|
| Translabyrinthine | Through mastoid and labyrinth | No (destroys cochlea) | Large tumours; non-serviceable hearing |
| Retrosigmoid (suboccipital) | Posterior fossa craniotomy behind sigmoid sinus | Yes (if cochlear function intact) | Medium-large tumours; hearing preservation possible |
| Middle fossa | Temporal craniotomy superior to IAC | Yes | Small intracanalicular tumours; hearing preservation in young patients |
Surgical Approaches for Acoustic Neuroma
The facial nerve is the primary concern in acoustic neuroma surgery. The facial nerve runs anterosuperiorly in the IAC and is typically stretched over the tumour capsule. Intraoperative facial nerve monitoring is mandatory. Facial nerve outcome is graded using the House-Brackmann (HB) scale: HB I = normal function, HB VI = total palsy. For expert surgeons operating on small tumours, HB I–II outcome is expected in >90% of cases; for large tumours the facial nerve may be thinned or adherent, increasing palsy risk.
Hearing preservation in surgery requires:
- Small tumour (<1.5 cm)
- Serviceable preoperative hearing (Gardner-Robertson class I–II: SRT ≤50 dB, SDS ≥50%)
- Suitable anatomy for a hearing-preservation approach (retrosigmoid or middle fossa)
Complications of microsurgery: CSF leak (most common — 10–15%), meningitis, cerebellar or brainstem injury, facial palsy, hearing loss (total on the operated side for translabyrinthine), headache, lower cranial nerve palsies with large tumours.
CLINICAL PEARL
The single most important clinical rule for acoustic neuroma is: any patient with unexplained unilateral SNHL — regardless of degree — deserves an MRI with gadolinium through the internal auditory canals. The audiogram cannot exclude an acoustic neuroma; tumours can be present with any degree of hearing loss, including normal hearing. The cost of missing an acoustic neuroma is years of untreated tumour growth, potential facial palsy from a larger tumour, and ultimately reduced surgical options. A second key rule: bilateral acoustic neuromas in a patient under 30 years old is NF2 until proven otherwise — arrange genetic counselling and NF2 screening.
Self-Assessment: Acoustic Neuroma
Use the following questions to assess your understanding of acoustic neuroma. Work through each one before checking the answer. Self-assessment at this stage is most effective when you verbalise your reasoning — as if presenting to a senior colleague — rather than simply recognising the correct option. Research consistently shows that retrieval practice (attempting to recall before re-reading) produces stronger long-term retention than passive review. Cover the SDL and attempt to answer each question from memory first; then check your response against the relevant section above. Pay particular attention to the EN known-traps: tuning-fork interpretation in SNHL versus conductive hearing loss, and the clinical distinction between acoustic neuroma and Meniere's disease as causes of unilateral audiovestibular symptoms.
Key concept checks:
- Why is the tumour called a 'vestibular schwannoma' rather than an 'acoustic neuroma'?
- In the IAC, which nerve is positioned anterosuperiorly?
- What audiological pattern (speech audiometry) distinguishes retrocochlear from cochlear SNHL?
- Name three features on MRI that distinguish acoustic neuroma from meningioma.
- Which surgical approach preserves hearing and is best for small intracanalicular tumours?
- What is the House-Brackmann grading scale used for?
- What is the annual growth rate of a typical acoustic neuroma?
Review your answers against the content above. If you struggled with the tuning-fork interpretation or the IAC anatomy, revisit the recall block and the anatomy section before proceeding.
SELF-CHECK
A 45-year-old patient with a 2.5 cm right acoustic neuroma has moderate SNHL (SRT 55 dB) on that side and is otherwise fit. The neurosurgical team is planning microsurgical excision. Which surgical approach is MOST likely to be used, and why?
A. Middle fossa approach, because it is the easiest for the surgeon
B. Translabyrinthine approach, because hearing preservation is no longer feasible at this SRT level and it provides the widest exposure
C. Retrosigmoid approach, because it always preserves hearing regardless of the audiogram
D. Observation alone, because surgery is never indicated for tumours under 3 cm
Reveal Answer
Answer: B. Translabyrinthine approach, because hearing preservation is no longer feasible at this SRT level and it provides the widest exposure
At SRT 55 dB the hearing is non-serviceable (SRT >50 dB = Gardner-Robertson class III or worse), meaning hearing preservation surgery is not warranted. The translabyrinthine approach sacrifices residual hearing but provides the widest, most direct access to the IAC and CPA, with the best facial nerve visualisation from the lateral end of the canal — making it the preferred approach when hearing preservation is not a goal. The middle fossa approach is reserved for small intracanalicular tumours with serviceable hearing. The retrosigmoid approach can preserve hearing but is not universally superior — and at 2.5 cm with non-serviceable hearing, translabyrinthine is often preferred. Surgery is absolutely indicated for growing tumours, large tumours, and symptomatic patients.