Page 13 of 23
EN4.8 | Complications of CSOM — SDL Guide
Learning Objectives
- Identify the clinical red-flag symptoms that indicate a complication of CSOM and distinguish them from uncomplicated disease
- Classify CSOM complications as extracranial (intratemporal) or intracranial and describe the clinical features and investigations for each major complication
- Describe the management principles for extracranial and intracranial complications of CSOM, including the role of surgery and antibiotics
- Recognise Gradenigo syndrome and the specific features of lateral sinus thrombophlebitis and brain abscess from CSOM
INSTRUCTIONS
Complications of CSOM are among the most serious and potentially fatal conditions in clinical ENT practice. Even in the antibiotic era, they carry significant mortality when diagnosed late. The key clinical insight is that complications arise from CSOM that has been neglected, mismanaged, or has progressed despite treatment — and that early recognition of the transition from uncomplicated to complicated disease is a life-saving skill. This module equips you to recognise the warning signs, classify the complication, choose the correct investigations, and initiate the appropriate emergency management.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th edition, Ch 8 (Complications of CSOM) (textbook)
- Hazarika P — Textbook of ENT and Head and Neck Surgery, 3rd edition, Ch 12 (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th edition, Vol 2 (Otology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old man is brought to casualty with a 3-day history of worsening headache, fever (38.8°C), and right-sided ear discharge. His family says he has had recurrent ear infections since childhood and the ear has been 'smelling bad' for months. This morning he developed right-sided facial weakness and began vomiting. On examination he has left lateral rectus palsy, the right pinna is pushed outward with post-auricular erythema and fluctuance, and the right tympanic membrane shows an attic crust with a foul-smelling attic perforation. What complications are present? Which is immediately life-threatening, and what is your first management action?
WHY THIS MATTERS
Complications of CSOM represent the most serious end of the chronic ear disease spectrum — and they remain relevant in modern clinical practice, especially in India and other settings where CSOM is prevalent, follow-up is inconsistent, and access to early surgical intervention is limited. Despite effective antibiotics and improved surgical techniques, intracranial complications of CSOM still carry a mortality of 10–40% when diagnosed late, and extracranial complications can result in permanent hearing loss, facial paralysis, or labyrinthine damage. The majority of these complications arise from squamosal (unsafe) CSOM with cholesteatoma, because the enzymatic bone erosion that characterises cholesteatoma creates direct pathways from the middle ear to the dura, the sigmoid sinus, the labyrinth, and the facial nerve. However, mucosal CSOM can also cause complications — particularly when infected middle ear pus is under tension without drainage, or when long-standing infection with virulent organisms (Pseudomonas, anaerobes) extends through pre-formed bony channels. The clinician who understands the anatomy of spread and the clinical signatures of each complication will be able to diagnose CSOM complications before they become irreversible. Competency EN4.8 requires you to describe clinical features, choose investigations, and describe management of CSOM complications.
RECALL
From your previous modules, recall the anatomy of the middle ear cleft and its relationships. The middle ear is surrounded by structures of vital importance: superiorly, the tegmen tympani (a thin plate of bone separating the middle ear from the middle cranial fossa); posteriorly, the mastoid air cell system and the sigmoid sinus (separated from the mastoid by only a thin bony plate — the sigmoid plate); inferiorly, the jugular bulb and the internal jugular vein; medially, the labyrinth (cochlea and semicircular canals) and the internal auditory canal; anteriorly, the internal carotid artery. The facial nerve runs in a bony canal through the middle ear and mastoid — first horizontally above the oval window (tympanic/horizontal segment), then vertically down through the mastoid (mastoid/vertical segment). Recall that the petrous apex — the medial tip of the petrous bone — houses the apex air cells and sits adjacent to the abducens nerve (CN VI) in Dorello's canal. This anatomical proximity explains the Gradenigo triad when petrous apex infection occurs.
Clinical Presentation: When CSOM Becomes Dangerous
The cardinal clinical feature that signals the transition from uncomplicated to complicated CSOM is the onset of new symptoms in a patient with a previously stable chronic ear. In uncomplicated CSOM — both mucosal and squamosal types — the disease is characterised by ear discharge and hearing loss but an absence of pain, systemic illness, neurological symptoms, or balance disturbance. The appearance of any of the following symptoms in a patient with known or suspected CSOM must be treated as a complication until proven otherwise: otalgia (ear pain), headache, fever (especially spiking or swinging in pattern), vertigo, facial weakness, or any neurological symptom (altered consciousness, confusion, neck stiffness, papilloedema, diplopia). The clinician must not be reassured by the fact that CSOM has been 'stable' for years — cholesteatoma in particular can be silently expanding for a long period and then suddenly break through into a previously safe bony boundary. Similarly, the cessation of discharge in a patient with active CSOM — so-called 'sudden drying up' — can paradoxically indicate that pus has broken through the tegmen or another bony barrier into a new space, and the outward drainage has been replaced by intracranial accumulation.
Red-flag symptoms in CSOM — any present = investigation and specialist referral urgently:
- New or worsening otalgia or mastoid tenderness
- Headache (especially persistent, progressive, or severe) in a CSOM patient
- Fever — especially spiking, swinging, or associated with rigors
- Post-auricular swelling, redness, or pinna displacement (subperiosteal abscess)
- Vertigo or imbalance (labyrinthine involvement)
- Facial weakness — ipsilateral lower motor neuron pattern (facial nerve erosion)
- Neurological signs: confusion, neck stiffness, papilloedema, focal deficits, diplopia (lateral rectus palsy)
- Sudden cessation of ear discharge in a previously discharging CSOM (drainage may have redirected intracranially)
Anatomy of Spread: How Infection Reaches Dangerous Sites
Understanding how infection spreads from the middle ear to produce extracranial and intracranial complications requires mapping the anatomical routes available to the spreading organism. There are three main mechanisms of spread, and they operate simultaneously in most complicated CSOM cases — understanding which mechanism is active in a given case helps the surgeon predict what structures are at risk.
The first mechanism is direct bone erosion — the most common mechanism in squamosal CSOM with cholesteatoma. Collagenases secreted by the cholesteatoma matrix progressively dissolve adjacent bone, allowing the expanding cyst and its inflammatory reaction to breach the tegmen tympani (→ middle cranial fossa), the mastoid cortex (→ subperiosteal abscess), the sigmoid sinus plate (→ lateral sinus thrombophlebitis), the semicircular canal walls (→ labyrinthine fistula and labyrinthitis), the facial nerve canal (→ facial palsy), or the petrous apex (→ petrositis/Gradenigo syndrome). This mechanism is gradual, enzyme-driven, and painless in its early stages — reinforcing why cholesteatoma can cause serious damage before clinical symptoms appear.
The second mechanism is spread through vascular channels — particularly relevant in mucosal CSOM with virulent organisms. Thrombophlebitis of the diploic veins and emissary veins connecting the mastoid to the sigmoid sinus or the middle cranial fossa allows infection to spread haematogenously to the intracranial compartment. This is the principal mechanism of lateral sinus thrombophlebitis and perisinus abscess.
The third mechanism is spread through pre-formed anatomical pathways — channels that exist normally in the petrous bone but are widened or exploited by infection. Hyrtl's fissure (a congenital developmental gap in the floor of the internal auditory canal) and the cochlear aqueduct can allow infection to spread from the middle ear to the subarachnoid space. Round window membrane rupture can allow toxic products to enter the perilymph.
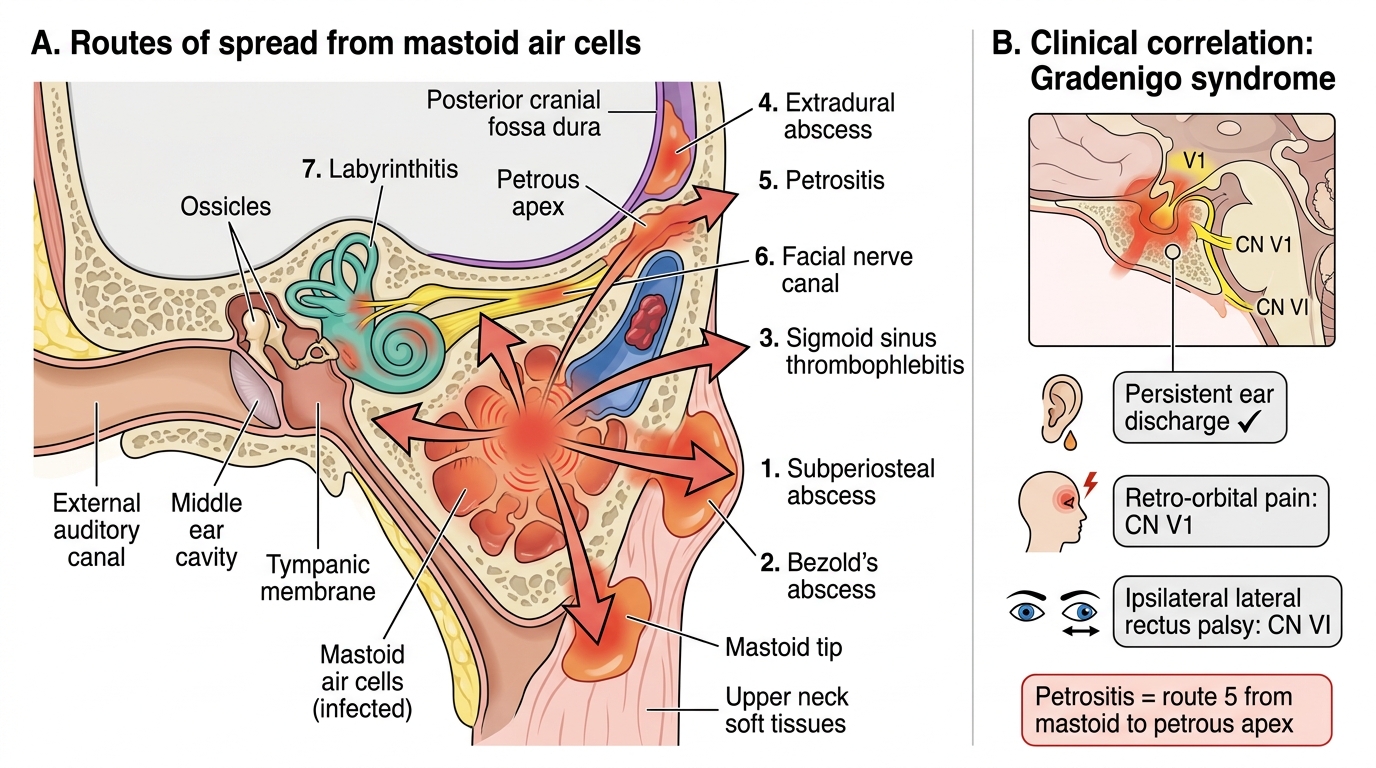
Routes of Spread from Mastoid Infection
SELF-CHECK
A 30-year-old with squamosal CSOM develops a deep, constant pain behind the right eye (in the distribution of the ophthalmic division of the trigeminal nerve), diplopia on right lateral gaze, and a persistently draining right ear. This triad is called:
A. Ramsey Hunt syndrome — geniculate ganglion herpes zoster causing otalgia, facial palsy, and ear blistering
B. Gradenigo syndrome — petrous apex infection causing persistent ear discharge, retroorbital pain (V1), and ipsilateral CN VI palsy
C. Meniere's triad — endolymphatic hydrops causing vertigo, sensorineural hearing loss, and tinnitus
D. Bezold's abscess — mastoid tip perforation causing neck swelling and cranial nerve involvement
Reveal Answer
Answer: B. Gradenigo syndrome — petrous apex infection causing persistent ear discharge, retroorbital pain (V1), and ipsilateral CN VI palsy
Gradenigo syndrome is the triad of: (1) persistent ear discharge, (2) deep pain in the distribution of CN V1 (ophthalmic, retroorbital), and (3) ipsilateral lateral rectus palsy (CN VI palsy) — caused by infection of the petrous apex, which lies adjacent to the abducens nerve (CN VI) in Dorello's canal and the trigeminal ganglion at the apex. It is a complication of CSOM in which mastoid infection extends medially to the petrous tip. It is rare but classic and must not be confused with Gradenigo's other eponyms.
Extracranial Complications: Examination and Investigation
Extracranial (intratemporal) complications of CSOM are those that spread outside the middle ear and mastoid but do not breach the dura or enter the cranial cavity. They are dangerous but have a better prognosis than intracranial complications when recognised and treated promptly. The clinician's examination and investigation strategy for each extracranial complication targets the specific anatomical structure involved. Every CSOM patient presenting with new symptoms should have a complete otoscopic examination under microscopy, a facial nerve assessment (House-Brackmann grade), a neurological examination, and an immediate HRCT of the temporal bones. The following are the principal extracranial complications and their clinical signatures.
1. Subperiosteal mastoid abscess:
Pus collects between the mastoid cortex (after it is eroded) and the periosteum, displacing the pinna outward and anteriorly. Classic signs: post-auricular swelling, erythema, and tenderness with loss of the post-auricular crease; pinna pushed outward and downward. Distinguished from simple mastoid tenderness by fluctuance. CT: eroded mastoid cortex with collection. Management: incision and drainage + mastoidectomy.
2. Bezold's abscess:
Pus erodes through the mastoid tip (the inferior aspect of the mastoid process) and tracks into the neck along the posterior belly of the digastric muscle and the sternocleidomastoid muscle. Signs: deep neck swelling below the mastoid tip, limited and painful neck movement, dysphagia if tracking to parapharyngeal space. CT neck reveals the collection tracking from the mastoid tip. Management: mastoidectomy + neck drainage of the abscess.
3. Zygomatic abscess:
Rare — pus tracks anteriorly through the zygomatic air cells, presenting as swelling anterior to and above the ear (over the zygomatic arch). CT shows zygomatic air cell involvement.
4. Masked mastoiditis:
Acute mastoiditis in which prior antibiotic treatment has suppressed systemic signs without eradicating the infection — the mastoid becomes a 'ticking time bomb' of suppurative infection without the classic signs of acute mastoiditis. Suspect in a patient with CSOM who has been given antibiotics but continues to have persistent ear discharge, ongoing hearing loss, and low-grade mastoid tenderness without the full acute presentation. CT is diagnostic (opacified mastoid air cells, bone osteitis).
5. Facial nerve palsy:
Ipsilateral lower motor neuron facial palsy (incomplete eye closure, drooped corner of mouth, loss of forehead wrinkle on the affected side) from erosion of the facial nerve canal by cholesteatoma, most commonly at the tympanic (horizontal) segment above the oval window or the vertical (mastoid) segment. House-Brackmann grading documents severity. CT shows facial canal dehiscence. Facial palsy in CSOM is a surgical emergency: immediate mastoidectomy with facial nerve decompression is required to prevent permanent paralysis.
6. Labyrinthitis:
Infection spreads into the labyrinth via a labyrinthine fistula (cholesteatoma eroding through the semicircular canal), round window diffusion, or haematogenous spread. Presents with sensorineural hearing loss + vertigo + nausea in a CSOM patient — a sudden SNHL or new vestibular dysfunction in CSOM must always raise the question of labyrinthine involvement. Types: serous labyrinthitis (toxic, reversible if treated) and suppurative labyrinthitis (bacterial invasion — leads to permanent deafness and may spread to meningitis). CT/MRI: fistula sign at the lateral semicircular canal; labyrinthine opacification in suppurative type.
7. Petrositis (Gradenigo syndrome):
Infection extends medially from the mastoid into the pneumatised petrous apex, involving the petrous apex air cells adjacent to the abducens nerve (CN VI) in Dorello's canal and the trigeminal ganglion. Classic triad: persistent ear discharge + deep retroorbital pain (CN V1 distribution) + ipsilateral CN VI palsy (lateral rectus palsy → inability to abduct the affected eye → diplopia on lateral gaze). CT/MRI: opacified petrous apex with erosion. Management: mastoidectomy + petrous apex drainage.