Page 14 of 23
EN4.8 | Complications of CSOM — SDL Guide (Part 2)
Intracranial Complications: Diagnosis
Intracranial complications of CSOM are life-threatening emergencies. They arise when infection or its products breach the dura and enter the intracranial compartment through the mechanisms described above. Mortality remains significant (10–40%) despite modern antibiotics and neurosurgical capabilities — the key determinant of outcome is the speed of diagnosis and the promptness of combined surgical (ENT + neurosurgery) and antibiotic management. Any CSOM patient with headache, fever, altered consciousness, neck stiffness, papilloedema, or focal neurological deficits must be treated as having an intracranial complication until proven otherwise. The investigation sequence is: urgent contrast-enhanced CT head and temporal bones → lumbar puncture only if CT excludes raised ICP and mass effect (LP in the context of an intracranial abscess risks tonsillar herniation) → blood cultures → IV antibiotics immediately. Do not delay antibiotics while awaiting imaging in a patient who is haemodynamically unstable or showing signs of rapid neurological deterioration.
Provided image
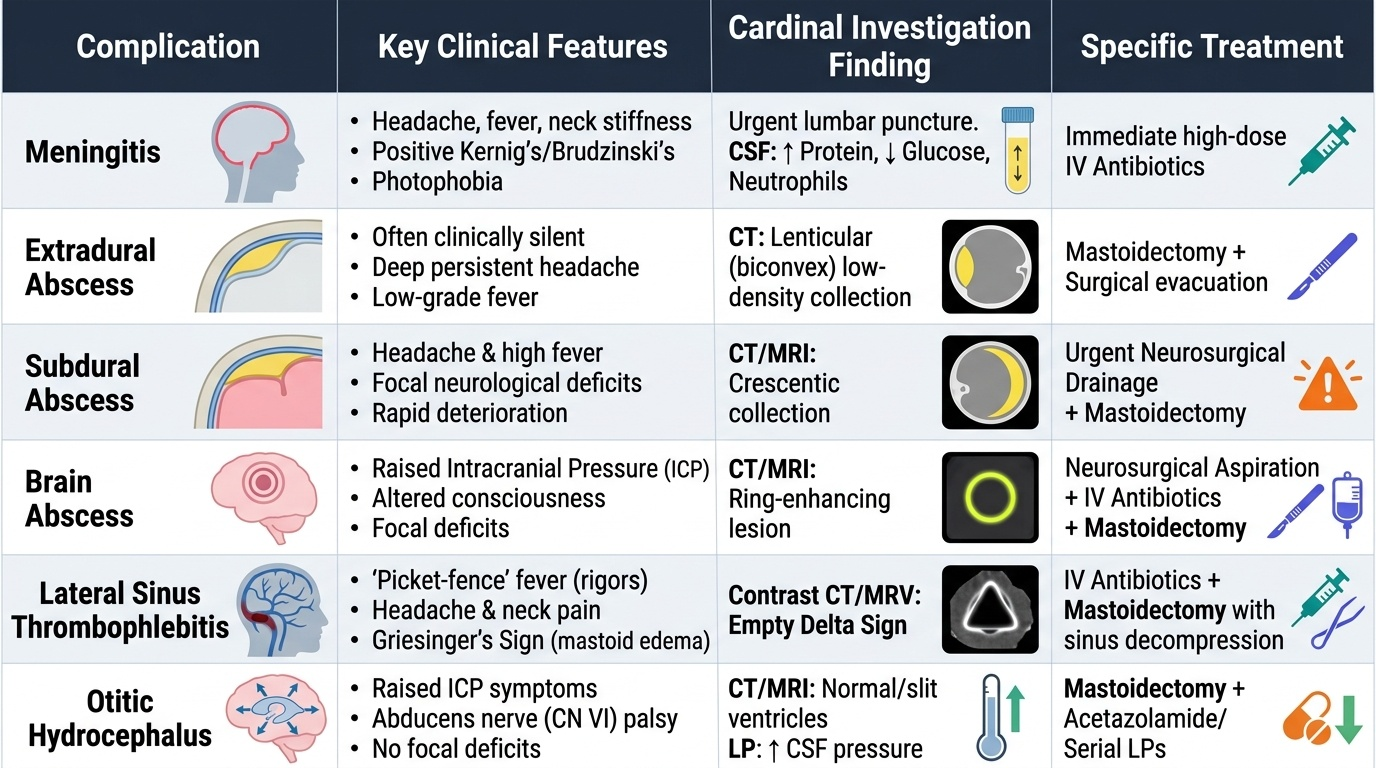
1. Extradural (epidural) abscess:
Pus collects between the dural surface and the inner table of the temporal bone from direct bone erosion. Often clinically silent (the dura resists penetration initially). May present with headache and low-grade fever. CT: lenticular low-density collection adjacent to the petrous bone. Management: mastoidectomy with evacuation of extradural pus; ENT procedure can drain both.
2. Subdural abscess:
Pus collects between the dura and the arachnoid mater. More dangerous than extradural — direct contact with the brain surface. Presents with headache, fever, focal neurological deficits, and rapid deterioration. CT/MRI: crescentic collection along the inner dural surface. Management: urgent neurosurgical drainage + mastoidectomy.
3. Meningitis:
The most common intracranial complication of CSOM. Presents with the classic meningitis triad: headache + fever + neck stiffness (Kernig's and Brudzinski's signs positive), plus photophobia. In CSOM-related meningitis, the causative organism is typically gram-negative (Proteus, Pseudomonas, H. influenzae) or anaerobic — different from the community-acquired S. pneumoniae/N. meningitidis pattern. CSF: elevated protein, reduced glucose, neutrophilic pleocytosis. Management: IV antibiotics (broad-spectrum covering gram-negatives and anaerobes) + mastoidectomy to eradicate the source. Lumbar puncture only after CT excludes mass lesion.
4. Brain abscess:
The most dangerous intracranial CSOM complication, with the highest mortality. Two commonest sites: temporal lobe abscess (from middle ear infection spreading through the tegmen) and cerebellar abscess (from mastoid infection spreading through the posterior fossa dura). The classical stages of a brain abscess (cerebritis → capsule formation → mature abscess) mean that in the early cerebritis stage symptoms may be subtle before the characteristic mass effect appears. CT with contrast: ring-enhancing lesion with surrounding oedema in the temporal lobe or cerebellum. MRI is superior for detection. Management: neurosurgical drainage (aspiration or excision of abscess) + mastoidectomy + IV antibiotics.
5. Lateral (sigmoid) sinus thrombophlebitis:
Thrombus forms in the sigmoid sinus from direct spread of infection through the sigmoid plate. Classic presentation: spiking picket-fence fever with rigors (repeated cycles of high fever followed by drenching sweats) + evidence of bacteraemia (positive blood cultures). May have signs of raised ICP. CT (with contrast) or MR venography: filling defect in the sigmoid sinus — the 'empty delta sign' on contrast CT. Management: anticoagulation (controversial) + IV antibiotics + mastoidectomy; if thrombus extends, jugular vein ligation may be considered.
6. Otitic hydrocephalus:
Raised intracranial pressure without a demonstrable abscess, associated with CSOM — probably from lateral sinus thrombosis impairing CSF absorption at the arachnoid villi, or from direct dural reaction. Presents with headache, papilloedema, and visual blurring; LP shows markedly elevated opening pressure but NORMAL CSF chemistry (unlike meningitis). CT brain: normal or small ventricles with diffuse cerebral oedema. Management: serial LPs, acetazolamide to reduce CSF production, mastoidectomy to remove the source.
SELF-CHECK
A 25-year-old with known squamosal CSOM develops spiking fever (39.5°C → 36.8°C → 39.5°C pattern) with rigors over 4 days, and positive blood cultures. He is not confused and has no focal neurological deficits. CT brain is normal. MR venography shows a filling defect in the right sigmoid sinus. The diagnosis is:
A. Brain abscess in the temporal lobe — requires neurosurgical aspiration
B. Lateral sinus (sigmoid sinus) thrombophlebitis — presents with the characteristic spiking picket-fence fever, rigors, bacteraemia, and sigmoid sinus filling defect on imaging
C. Bacterial meningitis — requires lumbar puncture and IV antibiotics
D. Otitic hydrocephalus — requires serial lumbar punctures and acetazolamide
Reveal Answer
Answer: B. Lateral sinus (sigmoid sinus) thrombophlebitis — presents with the characteristic spiking picket-fence fever, rigors, bacteraemia, and sigmoid sinus filling defect on imaging
The spiking picket-fence fever (repeated cycles of high fever and rigors), bacteraemia (positive blood cultures), and sigmoid sinus filling defect on MR venography are the classical features of lateral sinus (sigmoid sinus) thrombophlebitis — a complication of CSOM where infection from the mastoid spreads to the adjacent sigmoid sinus, forming an infected thrombus. The characteristic fever pattern reflects septic emboli released from the thrombus into the circulation. Management is IV antibiotics + mastoidectomy + consideration of anticoagulation. Brain abscess would show a ring-enhancing mass on CT; meningitis would have CSF abnormalities on LP; otitic hydrocephalus would show raised LP pressure with normal CSF chemistry but no sinus filling defect.
Management of CSOM Complications
The management of CSOM complications follows a single overriding principle: stabilise the patient, institute appropriate antibiotic cover, and remove the source of infection surgically — in that order and simultaneously. No CSOM complication is adequately treated by antibiotics alone; all require surgical eradication of the primary focus in the ear and mastoid. The specific surgical intervention (mastoidectomy, drainage of abscess, neurosurgical involvement) depends on the complication, but the ENT component of surgical management is non-negotiable in every case. Speed of action determines outcome: the difference between a patient who survives a brain abscess neurologically intact and one who does not is often the time elapsed between symptom onset and definitive surgical and antibiotic intervention.
General principles for all CSOM complications:
- Immediate hospital admission — no outpatient management for any confirmed complication
- IV antibiotics immediately: Start broad-spectrum cover including gram-negatives and anaerobes (e.g. ceftriaxone or cefotaxime + metronidazole + aminoglycoside cover guided by local resistance patterns). Adjust based on culture sensitivity when available. High-dose IV regimen.
- Imaging: Urgent contrast CT head and temporal bones for all patients with suspected intracranial complication; MRI venography for suspected lateral sinus thrombosis; CT neck for extracranial neck collections
- Neurosurgery liaison: For all intracranial complications — shared decision-making on timing and method of neurosurgical drainage vs ENT mastoidectomy
- LP only after CT excludes raised ICP: Do not perform LP in a patient with suspected brain abscess or raised ICP without imaging first
Specific surgical management:
- Subperiosteal/mastoid abscess: Mastoidectomy + evacuation of abscess; incision of the post-auricular abscess if fluctuant
- Bezold's abscess: Mastoidectomy + neck incision and drainage of the neck collection
- Facial nerve palsy from CSOM: Emergency mastoidectomy with facial nerve decompression; decompression within 2 weeks of palsy onset gives the best recovery prognosis
- Labyrinthitis: IV antibiotics; mastoidectomy to remove the cholesteatoma or primary focus; labyrinthectomy only if suppurative labyrinthitis with dead ear (to drain the infected labyrinth and prevent meningitis)
- Meningitis: IV antibiotics (gram-negative and anaerobic cover) + mastoidectomy after meningitis is controlled (usually at 48–72 hours of IV antibiotics unless worsening)
- Brain abscess: IV antibiotics + CT-guided neurosurgical drainage (aspiration or excision) + mastoidectomy to eradicate source
- Lateral sinus thrombophlebitis: IV antibiotics + mastoidectomy to remove infected bone adjacent to the sinus; anticoagulation is controversial but used in some centres to prevent propagation; jugular vein ligation if septic emboli continue
- Extradural/subdural abscess: Usually drained at the time of mastoidectomy (extradural); subdural may require separate neurosurgical craniotomy
- Otitic hydrocephalus: Treat the CSOM (mastoidectomy); serial LPs to reduce pressure; acetazolamide to reduce CSF production; may resolve once the source is removed
- Petrositis (Gradenigo): IV antibiotics + mastoidectomy + petrous apex drainage (most recover without direct petrous apex surgery)
CLINICAL PEARL
Two clinical pearls to memorise for CSOM complications: First, 'sudden drying of the ear' in a patient with active CSOM is NOT reassuring — it may mean that pus has broken through the tegmen into the cranial cavity, replacing outward canal drainage with intracranial accumulation. Always image a CSOM patient whose discharge suddenly stops if they have any systemic symptoms. Second, do NOT perform a lumbar puncture before imaging in a CSOM patient with headache and fever: if a brain abscess is present, LP will precipitate tonsillar herniation and death. Image first, LP only after CT confirms no mass lesion or raised ICP.
Self-Assessment: Complications of CSOM
At this point in the module, consolidate the two-tier classification of CSOM complications — extracranial (intratemporal) and intracranial — and the emergency action required for each. The extracranial group includes subperiosteal mastoid abscess, Bezold's abscess, zygomatic abscess, masked mastoiditis, facial nerve palsy, labyrinthitis, and petrositis (Gradenigo syndrome). Each has a specific clinical signature: post-auricular swelling with pinna displacement for subperiosteal abscess; deep neck swelling tracking from the mastoid tip for Bezold's; the classic Gradenigo triad (persistent discharge + CN V1 retroorbital pain + CN VI lateral rectus palsy) for petrositis; sudden SNHL + vertigo for labyrinthitis; and ipsilateral LMN facial palsy for facial nerve erosion. The intracranial group includes extradural abscess (often silent), subdural abscess (rapid neurological deterioration), meningitis (most common intracranial complication), brain abscess (temporal lobe or cerebellar; most dangerous), lateral sinus thrombophlebitis (picket-fence fever, bacteraemia, sinus filling defect), and otitic hydrocephalus (raised ICP, normal CSF chemistry). The investigation sequence in all cases: urgent CT head and temporal bones → LP only if no mass lesion or raised ICP → blood cultures → IV antibiotics → surgical planning. All complications require mastoidectomy to remove the source.
Key facts for self-testing:
- Most common intracranial complication: meningitis
- Most dangerous (highest mortality): brain abscess
- Gradenigo triad: persistent discharge + retroorbital pain (V1) + lateral rectus palsy (CN VI)
- Picket-fence fever + sigmoid sinus filling defect = lateral sinus thrombophlebitis
- Spiking fever → bacteraemia → septic emboli = sigmoid sinus thrombophlebitis
- Normal CSF chemistry + raised opening pressure = otitic hydrocephalus
- Sudden cessation of discharge in active CSOM = possible tegmen breach
- Never LP before CT in suspected intracranial CSOM complication
SELF-CHECK
A 35-year-old with squamosal CSOM develops sudden-onset severe vertigo, vomiting, and complete loss of hearing in the affected ear over 12 hours. On examination he cannot stand without support and has spontaneous nystagmus beating toward the unaffected ear. The most likely complication and the immediate clinical concern is:
A. Acute ASOM — treat with oral amoxicillin
B. Suppurative labyrinthitis — urgent concern is spread of infection into the subarachnoid space producing meningitis; requires IV antibiotics and mastoidectomy
C. Benign paroxysmal positional vertigo (BPPV) — reassure and prescribe Epley manoeuvre
D. Lateral sinus thrombophlebitis — requires MR venography and anticoagulation
Reveal Answer
Answer: B. Suppurative labyrinthitis — urgent concern is spread of infection into the subarachnoid space producing meningitis; requires IV antibiotics and mastoidectomy
Sudden complete sensorineural hearing loss + severe acute vestibular dysfunction (severe vertigo + nystagmus beating to the healthy side) in a patient with squamosal CSOM = suppurative labyrinthitis — bacterial invasion of the labyrinth through a cholesteatoma-created fistula or through the round window. The immediate clinical concern is that suppurative labyrinthitis can spread through the cochlear aqueduct or internal auditory canal into the subarachnoid space, causing meningitis. Management is IV antibiotics immediately + mastoidectomy. BPPV causes brief positional vertigo (not constant severe vertigo with hearing loss). Lateral sinus thrombophlebitis presents with spiking fever and bacteraemia, not acute profound hearing loss.