Page 7 of 23
EN4.{6,10} | Mucosal CSOM with Myringotomy and Tympanoplasty — SDL Guide
Learning Objectives
- Elicit and document a history in a patient with CSOM and correctly identify the mucosal (tubotympanic) type based on history and otoscopic features
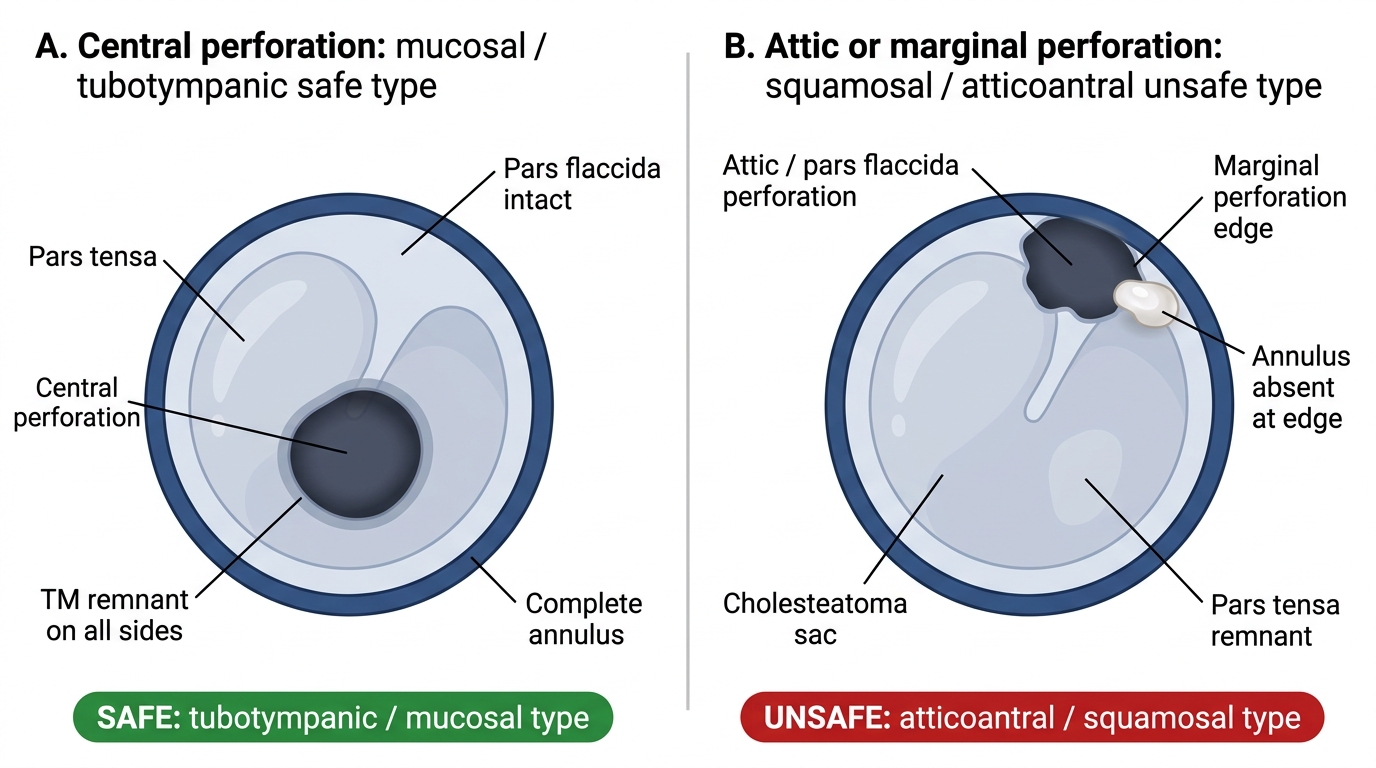
- Distinguish mucosal (safe) CSOM from squamosal (unsafe) CSOM using the central vs marginal/attic perforation and the presence or absence of cholesteatoma
- Describe the clinical features, otoscopic findings, and investigations appropriate for mucosal CSOM
- Describe the indications for and steps involved in myringoplasty and tympanoplasty (Wullstein Types I–V) for mucosal CSOM
INSTRUCTIONS
Chronic suppurative otitis media (CSOM) is one of the most common ENT problems encountered in India and is a leading cause of preventable conductive hearing loss. The mucosal (tubotympanic) type — also called the 'safe' type — is the more common variant and is characterised by a central tympanic membrane perforation, mucosal middle ear disease, and absence of cholesteatoma. Understanding the safe/unsafe distinction is the most critical clinical skill in ENT practice: incorrectly classifying an unsafe CSOM as safe can delay lifesaving surgery. This module covers the safe type and its definitive surgical repair — myringoplasty and tympanoplasty.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th edition, Ch 6 (CSOM) (textbook)
- Hazarika P — Textbook of ENT and Head and Neck Surgery, 3rd edition, Ch 9-10 (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th edition, Vol 2 (Otology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old man comes to your OPD with a 10-year history of right ear discharge that comes and goes with every cold. He has had this since childhood following repeated ear infections. The discharge is mucoid, odourless, and not associated with pain. His hearing on the right is reduced. On otoscopy you see a large central perforation in the lower half of the right tympanic membrane; the middle ear mucosa is visible and looks pale pink and moist. There is no whitish debris, no bleeding tissue, and no discharge at this visit. The pars flaccida is completely intact. Is this a safe or unsafe CSOM? What does the perforation location tell you, and how will you proceed?
WHY THIS MATTERS
Chronic suppurative otitis media (CSOM) is one of the most prevalent chronic ear diseases in developing countries, including India, where an estimated 5–10% of children are affected. It is the most common preventable cause of conductive hearing loss in children and young adults in low and middle-income countries. The vast majority of CSOM cases (approximately 80%) are of the mucosal (tubotympanic, 'safe') type, which arises as the end result of inadequately treated or recurrent ASOM in childhood. Despite being called 'safe,' mucosal CSOM causes significant morbidity: the persistent central TM perforation produces chronic conductive hearing loss, recurrent episodes of discharge, and social stigma. More importantly, understanding the safe type in detail prepares you to recognise the unsafe type — because the critical clinical skill is not just diagnosing CSOM, but correctly classifying it as safe or unsafe. Missing an unsafe CSOM is one of the most serious errors in ENT practice because it can lead to life-threatening intracranial complications. Competencies EN4.6 and EN4.10 together require you to take a history, describe clinical features, choose investigations, describe management, and describe the operative steps of myringotomy and tympanoplasty.
RECALL
Before studying CSOM, consolidate key anatomical and clinical concepts from earlier modules. Recall that the tympanic membrane is divided into four quadrants, and that the pars tensa (the large taut central portion) and the pars flaccida (Shrapnell's membrane — the small slack superior portion above the lateral process of the malleus) have different anatomical properties. The pars flaccida lacks the fibrous middle layer of the pars tensa and is therefore more susceptible to inward retraction under negative pressure. Recall that ASOM is the most common antecedent of CSOM: inadequately treated or recurrent ASOM leads to TM perforation that fails to heal. From your anatomy sessions recall the annulus fibrosus — the ring of fibrocartilage that anchors the TM to the tympanic bone; when a perforation involves the annulus, the TM has no rim of healthy tissue to support re-epithelialisation or surgical grafting. Finally, recall the Eustachian tube's role in maintaining middle ear health: in CSOM, persistent ET dysfunction maintains negative middle ear pressure that perpetuates the disease even after the acute infection resolves.
Clinical Presentation of Mucosal (Tubotympanic) CSOM
The clinical presentation of mucosal CSOM is dominated by two cardinal features: chronic or recurrent otorrhoea (ear discharge) and chronic conductive hearing loss. In contrast to ASOM, there is no fever and no severe otalgia — the absence of pain is one of the most clinically important features of uncomplicated mucosal CSOM and can be used to reassure patients that their disease is under control, while also serving as a red-flag indicator (onset of pain or headache in a previously painless CSOM suggests the development of a complication). The typical history follows a recognisable pattern: recurrent acute ear infections in childhood → initial episodes of ear discharge associated with fever → eventual resolution but incomplete TM healing → residual perforation → subsequent episodes of discharge triggered by URTIs or water entry into the ear without fever or severe pain. The discharge in mucosal CSOM is characteristically mucoid or mucopurulent, and — in uncomplicated disease — it is odourless or only mildly offensive. A frankly offensive, foul-smelling discharge with associated otalgia should immediately raise the suspicion of unsafe CSOM with cholesteatoma, where infected keratin debris produces a characteristic foul odour.
History of presenting illness — key questions:
- Duration of ear discharge (months to years), frequency (intermittent vs persistent), and triggers (URTIs, water entry)
- Character of discharge: colour, consistency (mucoid vs purulent vs thick cheesy), odour (odourless/mild = safe; offensive/foul = suspect unsafe)
- Hearing loss: gradual, bilateral or unilateral, worse on the affected side; duration
- Pain: ABSENT in uncomplicated mucosal CSOM; any new or worsening otalgia = red flag for complication or unsafe disease
- Tinnitus: present in some cases as a result of the conductive loss
- History of childhood ear infections, ASOM episodes, previous ear surgery
- Vertigo or facial weakness: both are red flags for complications regardless of type
Predisposing and perpetuating factors:
- Childhood recurrent ASOM (most common antecedent)
- Poverty, crowded living conditions, poor nutrition (affect immune response and access to care)
- Swimming (water entering through the perforation introduces pathogens)
- Delayed or inadequate antibiotic treatment of childhood ASOM
Anatomy and Pathophysiology of Mucosal CSOM
The pathophysiology of mucosal CSOM is best understood through the central principle of the safe vs unsafe distinction — the single most important conceptual divide in the management of chronic ear disease. Mucosal CSOM is called the 'safe' type not because it carries zero risk, but because in its uncomplicated form it does not erode bone, does not produce cholesteatoma, and carries a relatively low risk of intracranial complications. The squamosal (atticoantral, 'unsafe') type, by contrast, involves cholesteatoma, bone erosion, and high complication risk — it demands urgent surgical intervention and is covered in a separate module. Grasping this distinction at a deep anatomical level — not just as a label — is what allows the clinician to look at an otoscopic image and immediately classify the disease, choose the appropriate management pathway, and avoid the catastrophic error of treating unsafe CSOM conservatively while cholesteatoma silently erodes the ossicles, tegmen, or facial nerve canal.
The safe/unsafe distinction rests on two anatomical observations:
1. Location of the TM perforation:
- Mucosal (safe) type = central perforation in the pars tensa. A central perforation is one surrounded by a rim of residual TM on all sides — the annulus fibrosus is intact. The perforation may be small, medium, or large (subtotal), but healthy TM tissue remains as a border. Because the pars tensa forms the floor and walls of the mesotympanum, a central perforation exposes the mucosal middle ear but not the attic, the epitympanum, or the mastoid antrum — areas of dangerous communication where cholesteatoma forms.
- Squamosal (unsafe) type = attic or marginal perforation. An attic perforation is in the pars flaccida (Shrapnell's membrane) — the superior slacker portion of the TM. A marginal perforation extends to the annulus with no TM rim remaining at the edge. Both types allow squamous epithelium to migrate into the middle ear, forming a cholesteatoma — a destructive cyst of desquamating keratin-producing epithelium.
2. Disease process:
- Mucosal type: The middle ear mucosa is inflamed and oedematous, producing mucoid secretions. The ossicles are usually intact (though may be partially eroded in long-standing disease). No cholesteatoma is present. The pathological process is confined to the mucosa of the mesotympanum and Eustachian tube.
- Squamosal type: Cholesteatoma is present — keratin-filled squamous epithelium expands in the middle ear, secreting collagenases that erode bone (ossicles, tegmen, labyrinthine bone, facial nerve canal) and eventually breach the skull base or dura.
Why perforations in ASOM fail to heal: After ASOM, the TM heals by re-epithelialisation from the edges of the perforation. In some cases — particularly after repeated infections, large perforations, or perforations involving the posterior quadrant where the blood supply is poorer — healing fails. The Eustachian tube dysfunction that caused the ASOM persists, creating chronic negative middle ear pressure that prevents natural healing. The residual perforation then becomes a route for recurrent contamination.
Tympanic Membrane Perforations: Safe vs Unsafe Types
SELF-CHECK
A 30-year-old has a 15-year history of right ear discharge. Otoscopy shows a large perforation in the lower two-thirds of the pars tensa. The pars flaccida is intact. The annulus is visible at all margins of the perforation. There is no whitish debris. Based on the perforation characteristics, this is CSOM of which type, and why?
A. Squamosal (unsafe) type — because the perforation is large and the hearing loss is significant
B. Mucosal (safe, tubotympanic) type — because the perforation is central in the pars tensa with TM remnant on all sides and no involvement of pars flaccida or annulus erosion
C. Squamosal (unsafe) type — because the pars tensa perforation suggests posterior extension to the attic
D. Cannot be determined without a CT temporal bone
Reveal Answer
Answer: B. Mucosal (safe, tubotympanic) type — because the perforation is central in the pars tensa with TM remnant on all sides and no involvement of pars flaccida or annulus erosion
A central perforation in the pars tensa — surrounded by a rim of intact TM tissue on all sides, with an intact pars flaccida and no annulus erosion — is the defining feature of mucosal (safe, tubotympanic) CSOM. The size of the perforation alone does not determine safety. The absence of whitish debris (cholesteatoma), odourless discharge, and intact pars flaccida all reinforce the safe classification. An unsafe (squamosal/atticoantral) type would show an attic perforation, marginal perforation with annulus erosion, or whitish pearly debris indicating cholesteatoma.
Examination and Investigations in Mucosal CSOM
The examination in mucosal CSOM begins with a thorough otoscopic assessment and hearing evaluation, supplemented by investigations to quantify hearing loss, assess ossicular integrity, and evaluate Eustachian tube function before planning surgery. The goal of examination is twofold: confirm the safe mucosal type (by excluding cholesteatoma, attic perforation, and marginal perforation) and assess the surgical candidacy of the patient (hearing level, ear status, ET function). This dual purpose shapes the examination sequence: the first part is diagnostic (is this safe or unsafe?) and the second is pre-operative (is this patient ready for tympanoplasty?). Every otoscopic examination of a CSOM ear must include explicit inspection of the pars flaccida — the failure to examine this superior quadrant is the single most common reason an attic perforation is missed and an unsafe CSOM is incorrectly classified as safe.
Otoscopic examination — systematic approach:
Clean the external auditory canal of discharge and wax with gentle suction or wicking. Then examine the TM systematically:
- Perforation location and size: Confirm it is a central perforation in the pars tensa; estimate size as small (<25% of TM), medium (25–50%), large (50–75%), or subtotal (>75%). The pars flaccida must be specifically examined — if it appears retracted, thickened, or has any defect, the classification must be reconsidered
- Pars flaccida: Must be intact and visible; any crust, retraction pocket, or perforation in the pars flaccida suggests unsafe type
- Middle ear mucosa: Visible through the perforation — in mucosal CSOM it appears pale pink or red and oedematous; mucoid secretion may be present; NO whitish pearly debris, no granulations eroding bone
- Ossicles: The handle of malleus and the umbo are identifiable from the perforation margin; note whether the incus long process or stapes is visible (their absence may indicate erosion)
- Retraction pockets: Should be specifically looked for in all quadrants; a deep retraction pocket in the posterosuperior quadrant can hide early cholesteatoma
Hearing assessment:
- Tuning fork tests (512 Hz): Rinne negative on the affected side (BC > AC) confirming conductive hearing loss; Weber lateralises to the affected ear; ABC (absolute bone conduction) test — if normal (same as examiner's), ossicular chain and cochlear function are intact. A reduced ABC suggests sensorineural component or mixed loss.
- Pure-tone audiometry (PTA): Shows conductive hearing loss with an air-bone gap; the size of the gap correlates roughly with perforation size and ossicular integrity. A purely conductive air-bone gap of 20–40 dB with normal bone conduction thresholds is characteristic of uncomplicated mucosal CSOM. If the bone conduction threshold is elevated, suspect inner ear involvement (labyrinthine or toxic damage from chronic infection)
Investigations:
- CT of the temporal bone (HRCT): Not routine for uncomplicated mucosal CSOM, but indicated when: (1) ossicular erosion suspected, (2) need to plan the extent of surgery, (3) complication suspected. HRCT is MANDATORY in squamosal/unsafe CSOM — but for straightforward mucosal CSOM, otoscopy + PTA are often sufficient for surgical planning
- Eustachian tube function tests: Critical before tympanoplasty. A simple test: the patient performs the Valsalva manoeuvre and the surgeon observes air bubbling through the middle ear (via the perforation). Eustachian tube patency is necessary for surgical success — grafting a TM onto a middle ear with severely dysfunctional ET leads to early graft failure and recurrence of retraction
- Culture and sensitivity: Of discharge when present; guides choice of topical antibiotic