Page 8 of 23
EN4.{6,10} | Mucosal CSOM with Myringotomy and Tympanoplasty — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The diagnosis of mucosal CSOM is primarily clinical, combining a characteristic history (chronic recurrent odourless discharge, conductive hearing loss, no pain) with otoscopic confirmation of a central TM perforation in the pars tensa without cholesteatoma or attic involvement. The most important diagnostic distinction — and the one with the greatest clinical consequence — is between the mucosal (safe) and squamosal (unsafe) types of CSOM. This is not merely an academic categorisation: the unsafe type requires surgical intervention (mastoidectomy) regardless of symptoms, while the safe type can be managed conservatively until surgical conditions are optimal. The clinician who can make this distinction rapidly and reliably at the otoscope, without needing advanced imaging, is demonstrating the core ENT clinical competency that underlies all further management of chronic ear disease.
Safe vs Unsafe CSOM — the defining comparison:
| Feature | Mucosal CSOM (Safe, Tubotympanic) | Squamosal CSOM (Unsafe, Atticoantral) |
|---|---|---|
| Perforation site | Central, pars tensa | Attic (pars flaccida) or marginal |
| Annulus involvement | No — TM rim present on all sides | Yes — marginal type has no TM rim |
| Cholesteatoma | ABSENT | PRESENT |
| Discharge | Mucoid/mucopurulent, odourless/mildly offensive | Scanty, foul-smelling (keratin + secondary infection) |
| Hearing loss | Conductive only (usually) | Conductive ± sensorineural if labyrinth eroded |
| Bone erosion | Absent or minimal | Significant — ossicles, tegmen, labyrinthine capsule, facial canal |
| Complications | Rare in uncomplicated disease | Common — mastoiditis, labyrinthitis, meningitis, brain abscess |
| Surgery urgency | Elective (tympanoplasty when ear is dry) | URGENT mastoidectomy regardless of symptoms |
Additional differentials:
ASOM with spontaneous perforation: Acute onset (days, not months/years); fever and severe otalgia precede discharge; discharge purulent; TM hyperaemic around the perforation; perforation usually heals within 2–4 weeks with treatment. The chronicity of CSOM (>12 weeks by definition) distinguishes it.
Tympanosclerosis: White chalky calcification visible in the TM or on the ossicles — residual from old ASOM or previous ear surgery. TM is intact (no active perforation). Tympanosclerosis of the ossicles can cause conductive loss without perforation.
Otitis externa: Infection of the external canal, not the middle ear; TM usually normal when visible; tragal tenderness; history of water exposure or scratching.
SELF-CHECK
A 28-year-old presents with foul-smelling right ear discharge, mild dull otalgia, and 10 years of ear problems. Otoscopy shows a crust in the right attic with a small attic perforation in the pars flaccida. Whitish pearly debris is visible behind the crust. This finding indicates:
A. Mucosal (safe) CSOM — the attic location is within normal central perforation variation
B. Otitis externa — the crust and debris are consistent with canal skin desquamation
C. Squamosal (unsafe) CSOM with cholesteatoma — attic perforation with pearly debris requires urgent mastoidectomy
D. Tympanosclerosis — the white debris is calcification and requires no intervention
Reveal Answer
Answer: C. Squamosal (unsafe) CSOM with cholesteatoma — attic perforation with pearly debris requires urgent mastoidectomy
An attic perforation (in the pars flaccida) with whitish pearly debris is the otoscopic signature of squamosal (unsafe) CSOM with cholesteatoma. The attic location, foul odour, and pearly debris (keratin matrix of cholesteatoma) are the classic triad. This is an UNSAFE type requiring urgent mastoidectomy. Calling an attic perforation 'within normal variation' of a central perforation is a dangerous error. Tympanosclerosis is white but is a calcification of the TM surface — it does not present as perforation with pearly debris filling the attic space.
Management: Medical and Surgical (Myringotomy and Tympanoplasty)
Management of mucosal CSOM has two phases: a conservative phase aimed at achieving a dry, infection-free ear, and a surgical phase (tympanoplasty) aimed at definitive repair of the TM perforation and restoration of hearing. The principle is that surgery should never be performed on a wet, actively infected ear — hence the conservative phase must precede surgery and the ear must be dry for a minimum of 6 weeks before tympanoplasty. Trying to graft an infected, discharging ear leads to graft failure and recurrence. This sequencing principle is one of the most operationally important rules in CSOM management. The reason it matters so much is pathological: in an actively infected middle ear, the mucosal surface cannot support the fascia graft, the operative field is obscured, and the graft is exposed to proteolytic enzymes from the infection that prevent fibroblast ingrowth and neovascularisation — the two processes on which graft take depends.
Provided image
Conservative management (to achieve a dry ear):
- Aural toilet: Dry mopping of the ear using a soft wick or suction to remove discharge; this is the single most effective conservative measure and should be performed at each clinic visit and taught to the patient for home care
- Topical antibiotic ear drops: Ciprofloxacin 0.3% ear drops (safe for use in perforated TM) are first-line; avoid aminoglycoside drops (gentamicin, neomycin) in perforated TM — ototoxic when they enter the middle ear through the perforation
- Systemic antibiotics: Used when active discharge with systemic signs (fever, cellulitis) is present; oral amoxicillin-clavulanate or ciprofloxacin based on culture; not indicated for routine management of chronic mucosal CSOM without active infection
- Treatment of Eustachian tube dysfunction: Intranasal corticosteroids and decongestants to reduce ET orifice mucosal oedema; treat allergic rhinitis; adenoidectomy if adenoid hypertrophy is a contributing factor
- Water precautions: Cotton wool with Vaseline in the ear during bathing; avoid swimming until TM is repaired
Surgical management — Tympanoplasty:
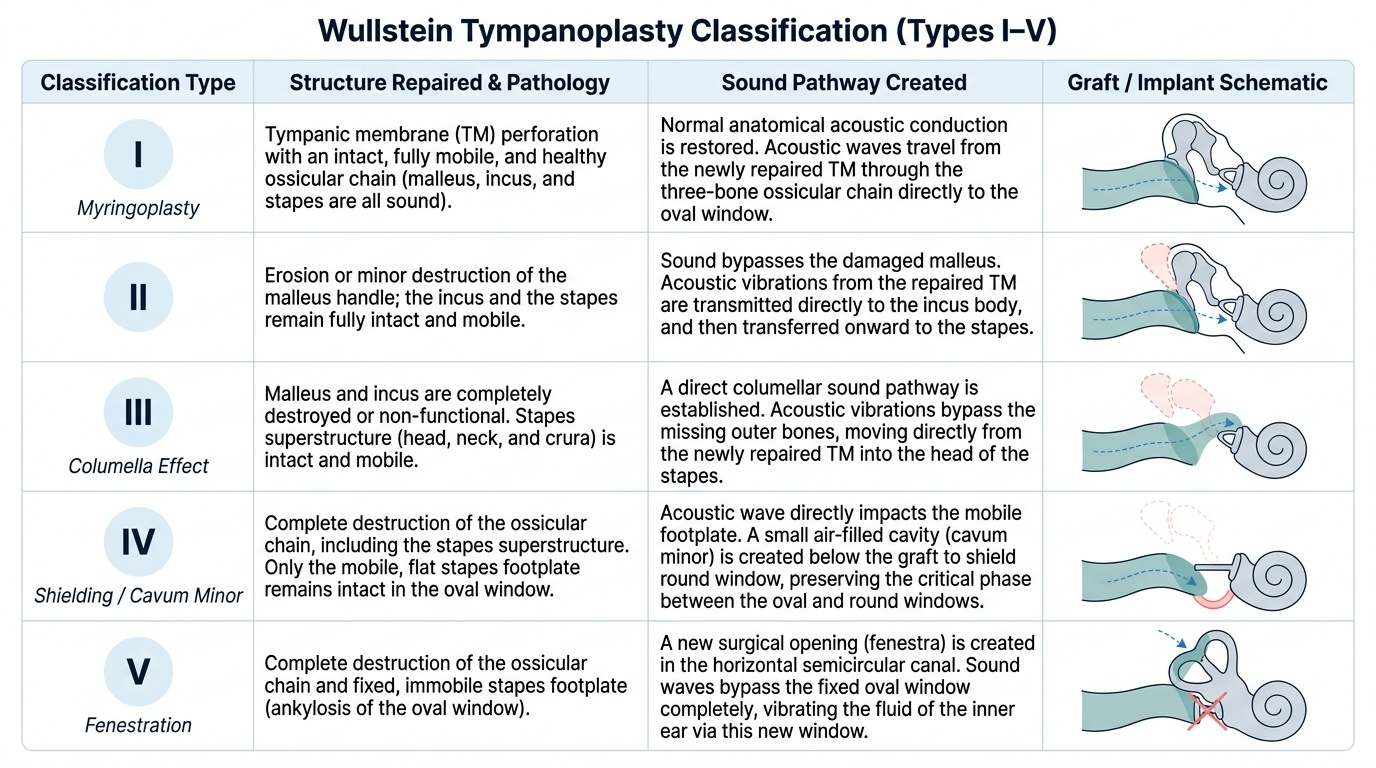
Wullstein Classification of Tympanoplasty (Types I–V):
| Type | Procedure | Mechanism | Indication |
|---|---|---|---|
| I | Myringoplasty — TM repair only; ossicles intact | Restores intact TM over functioning ossicular chain | TM perforation with intact mobile ossicular chain (most common) |
| II | TM graft placed on incus head | Bridging erosion of malleus handle | Malleus eroded but incus present |
| III | TM graft placed directly on stapes head (columella effect) | Stapes-to-TM transmission | Malleus and incus both eroded; stapes intact and mobile |
| IV | TM graft placed over stapes footplate; oval window baffle | Round window protected from direct sound by graft position | Stapes superstructure eroded; footplate mobile |
| V | Fenestration of horizontal semicircular canal | Bypass via new fenestra | Fixed stapes footplate (otosclerosis) — rarely used now |
Myringoplasty (Tympanoplasty Type I) — Operative Steps:
1. Pre-operative assessment: confirm dry ear for ≥6 weeks; PTA to confirm conductive loss; assess ET function; consent for the procedure
2. Anaesthesia: general anaesthesia (or local in cooperative adults)
3. Approach: post-aural (Wilde's incision behind the ear, most common) or endaural incision
4. Harvest graft: temporalis fascia is the most commonly used graft material — thin, durable, avascular (non-reactive), easy to harvest; alternative grafts: tragal cartilage perichondrium (more rigid, useful for large perforations or revision surgery), fat plug (for small anterior perforations)
5. Freshen the perforation edges: remove the epithelial edge of the perforation (the epidermal layer) using a round knife or micro-forceps to create a raw rim that will bond with the graft
6. Elevate a TM flap (tympanomeatal flap): elevate the posterior TM edge from the canal wall to access the middle ear and inspect the ossicular chain
7. Inspect the middle ear and ossicular chain: confirm ossicular mobility; remove any mucosal disease; assess ET orifice
8. Place the graft: the fascia graft is placed in the underlay position (deep to the TM remnant) — the graft lies between the TM and the middle ear, supported by Gelfoam packing placed in the middle ear space to hold the graft in position during healing
9. Re-drape the TM remnant over the graft; pack the canal with Gelfoam
10. Close the post-aural wound in layers; pack the outer canal with BIPP ribbon gauze
11. Post-operative: antibiotic cover; ear pack removal at 2–3 weeks; assess graft uptake at 6 weeks; PTA at 3 months to assess hearing gain
CLINICAL PEARL
The most critical operative principle in tympanoplasty is: the underlay technique for graft placement is the standard. The fascia graft is placed UNDER the TM remnant (between it and the middle ear), not on top. The graft is supported internally by Gelfoam soaked in antibiotic solution. This position allows the TM remnant's epithelial layer to migrate over the graft surface and fuse with it. An overlay technique (placing the graft on top of the TM remnant) risks anterior blunting of the TM angle — a complication that causes a persistent anterior perforation and a sharp angle deformity at the anterior canal wall junction.
Self-Assessment: Mucosal CSOM and Tympanoplasty
Before attempting the final self-check question, ensure you can fluently articulate the following framework. The single most important concept in this module is the safe/unsafe distinction: mucosal CSOM is safe because it has a central pars tensa perforation without cholesteatoma; squamosal CSOM is unsafe because it has an attic or marginal perforation with cholesteatoma, bone erosion, and high complication risk. Conflating these two types — or failing to examine the pars flaccida and attic systematically — is the most serious clinical error in CSOM management. The management algorithm for mucosal CSOM follows a logical sequence: achieve a dry ear by conservative means (aural toilet, safe topical drops, treat ET dysfunction), confirm ear is dry for ≥6 weeks, then perform tympanoplasty. Tympanoplasty is classified by Wullstein's five types according to the ossicular status — Type I (myringoplasty, most common) repairs only the TM when ossicles are intact; higher types reconstruct progressively greater ossicular defects. Graft material of choice is temporalis fascia, placed in the underlay position. Hearing improvement is assessed by PTA at 3 months post-operatively.
Key consolidation checklist:
- Safe type = tubotympanic = mucosal = central perforation in pars tensa
- Unsafe type = atticoantral = squamosal = attic/marginal perforation + cholesteatoma
- Most common causative organisms in mucosal CSOM discharge: Pseudomonas aeruginosa, Staphylococcus aureus, Proteus mirabilis (often polymicrobial)
- Safe topical ear drops in perforated TM: ciprofloxacin; aminoglycosides (gentamicin) are CONTRAINDICATED
- Minimum dry ear duration before tympanoplasty: 6 weeks
- Wullstein Type I = myringoplasty (TM repair only)
- Graft of choice: temporalis fascia; placed underlay
SELF-CHECK
A patient with mucosal CSOM has stopped discharging for 8 weeks following aural toilet and topical ciprofloxacin. PTA shows a moderate conductive hearing loss of 35 dB with normal bone conduction. Otoscopy shows a large central perforation in a dry, clean pars tensa. The pars flaccida is intact. The most appropriate next step is:
A. Continue watchful waiting for a further 6 months to see if the perforation closes spontaneously
B. Start systemic oral antibiotics for 2 more weeks before planning surgery
C. Perform myringoplasty (tympanoplasty Type I) with temporalis fascia graft using the underlay technique
D. Perform radical mastoidectomy because the large perforation indicates unsafe disease
Reveal Answer
Answer: C. Perform myringoplasty (tympanoplasty Type I) with temporalis fascia graft using the underlay technique
This patient has a dry central pars tensa perforation (confirming safe mucosal CSOM), has been dry for 8 weeks (exceeding the minimum 6-week dry requirement), and has significant conductive hearing loss that is surgically correctable. The appropriate intervention is myringoplasty (tympanoplasty Type I) — repair of the TM perforation with temporalis fascia graft placed underlay, which will restore the ossicular sound pathway and close the air-bone gap. Spontaneous closure of a large perforation in an adult is uncommon after years of CSOM; additional antibiotics are not needed in a currently dry ear; radical mastoidectomy is indicated for unsafe CSOM with cholesteatoma, not for the safe type.