Page 10 of 29
EN4.24 | Allergic Rhinitis — SDL Guide
Learning Objectives
- Elicit a structured history from a patient with allergic rhinitis, identifying the pattern (intermittent vs persistent), severity, and trigger allergens
- Describe the IgE-mediated pathophysiology of allergic rhinitis and how it explains the symptom complex
- Describe the clinical features and classify allergic rhinitis using the ARIA criteria
- Choose appropriate investigations — skin prick test, serum-specific IgE, nasal cytology — and interpret results
- Describe the principles of management including allergen avoidance, pharmacotherapy (INCS, antihistamines, decongestants), and allergen immunotherapy
INSTRUCTIONS
Allergic rhinitis affects approximately 20–30% of the Indian population and is among the top five most common chronic conditions seen in primary care and ENT outpatient departments. It significantly impairs quality of life, work and school performance, and sleep. EN4.24 requires you to take a correct history, describe clinical features, choose investigations, and describe management principles. Understanding allergic rhinitis also provides the pathophysiological foundation for asthma (the same atopic diathesis), eczema, and anaphylaxis.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery. 8th ed. Chapter on Allergic Rhinitis (textbook)
- Hazarika P, Nayak DR, Balakrishnan R. Textbook of Ear, Nose and Throat — Head and Neck Surgery. Chapter on Rhinitis (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery. 8th ed. Vol 2: Rhinology — Allergic Rhinitis (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old medical student comes to the ENT OPD in April. Every year around this time, she gets 4–6 weeks of intense nasal symptoms: profuse watery nasal discharge, violent sneezing attacks (10–15 sneezes in a row on waking), nasal and palatal itch, and red watery eyes. She misses classes because she cannot concentrate. Her mother and elder sister have the same problem. She has tried chlorpheniramine, which helps slightly but makes her drowsy. On examination: pale, boggy, slightly bluish inferior turbinates bilaterally, with watery secretions pooled in the nasal floor. You suspect allergic rhinitis. What pathophysiology explains every one of her symptoms? What investigation confirms the trigger? And what treatment will actually work without sedating her?
WHY THIS MATTERS
Allergic rhinitis is the most common immune-mediated disease of the upper airway and affects an estimated 400 million people worldwide. In India, it is strongly driven by house dust mite, cockroach allergen, and seasonal grass and tree pollens. It frequently co-exists with asthma — the 'united airway' concept holds that both diseases share the same atopic, IgE-mediated mechanism and that uncontrolled nasal allergic inflammation worsens bronchial disease. As a final-year student, you will see patients with allergic rhinitis in every specialty posting; the dermatologist treats their eczema, the pulmonologist treats their asthma, and the ophthalmologist treats their allergic conjunctivitis. The ENT surgeon manages their nasal disease — but the understanding of the shared atopic diathesis belongs to you as the treating physician, regardless of specialty.
RECALL
Recall from your immunology and pathology sessions the mechanism of Type I hypersensitivity. In atopy, a genetically predisposed individual produces IgE antibodies in response to normally harmless environmental proteins called allergens (house dust mite, pollen, animal dander, cockroach, mould spores). IgE binds to high-affinity receptors on the surface of mast cells (in mucosal tissue) and basophils (in blood). On re-exposure to the allergen, cross-linking of IgE–allergen complexes on mast cells triggers degranulation — release of preformed mediators including histamine, tryptase, and heparin. Histamine acting on H1 receptors on mucosal blood vessels and nerve endings produces vasodilatation (congestion), increased vascular permeability (watery rhinorrhoea), smooth muscle contraction, and stimulation of sensory nerve endings (itch and sneezing). This is the early phase (occurs within minutes). A late phase reaction (4–8 hours later) is driven by newly synthesised mediators — leukotrienes (LTB4, LTC4, LTD4), prostaglandins, and platelet-activating factor — and involves recruitment of eosinophils, T-helper 2 (Th2) lymphocytes, and basophils. The late phase accounts for the chronic nasal blockage and mucosal hyper-reactivity that persists between allergen exposures.
Clinical Presentation of Allergic Rhinitis
The clinical presentation of allergic rhinitis is driven by the histamine and leukotriene-mediated effects on the nasal mucosa and is characterised by four cardinal symptoms that cluster together and distinguish allergic rhinitis from most other forms of rhinitis. Recognising the full symptom complex, rather than any single symptom, is the key to accurate diagnosis. Each of the four symptoms maps directly onto a specific pathophysiological mechanism — this is one of the few clinical situations where knowing the mechanism allows you to predict the symptom and vice versa, making allergic rhinitis an excellent teaching case for the principle that mechanism-based clinical reasoning is superior to rote memorisation. In the history, the four symptoms should always be asked about together; the presence of all four in a young atopic patient with a relevant family history is virtually diagnostic without requiring investigation.
The four cardinal symptoms of allergic rhinitis are:
1. Watery rhinorrhoea — profuse, thin, clear nasal discharge (increased mucosal gland secretion and vascular transudation driven by histamine and leukotrienes).
2. Paroxysmal sneezing — repetitive, violent sneezing attacks (often 10–20 consecutive sneezes), particularly on waking or on exposure to the trigger; driven by histamine acting on H1 receptors on the nasal trigeminal nerve endings.
3. Nasal itch — persistent or episodic nasal itch, often accompanied by palatal and ocular itch (the patient rubs the nose upward with the palm — the "allergic salute").
4. Nasal obstruction — bilateral nasal congestion, particularly in the late-phase reaction; due to inferior turbinate mucosal oedema.
Classification (ARIA guidelines): The internationally used ARIA (Allergic Rhinitis and its Impact on Asthma) classification grades allergic rhinitis by:
- Duration: Intermittent (<4 days per week OR <4 consecutive weeks) vs Persistent (≥4 days per week AND >4 consecutive weeks).
- Severity: Mild (no impairment of daily activities, sleep, work, or school) vs Moderate-severe (one or more of: sleep disturbance, impairment of activities, impairment of work/school, troublesome symptoms).
Associated features: Eye symptoms (allergic conjunctivitis — red, watery, itchy eyes) are present in up to 50% of patients. Post-nasal drip (nasal secretions draining into the throat) causes throat clearing, cough, and pharyngeal discomfort. Hyposmia (reduced sense of smell) may occur from mucosal oedema obscuring the olfactory cleft.
Trigger patterns: Seasonal allergic rhinitis (hay fever) is triggered by tree pollens (spring), grass pollens (early summer), or weed pollens (late summer/autumn), varying by geography. Perennial (year-round) allergic rhinitis is triggered by house dust mite (HDM), cockroach, animal dander, and mould — all present year-round. Many Indian patients have both seasonal and perennial triggers.
Family history of atopy (asthma, eczema, allergic rhinitis) is strongly positive in 50–80% of patients — atopy runs in families as an autosomal polygenic trait.
Pathophysiology of Allergic Rhinitis
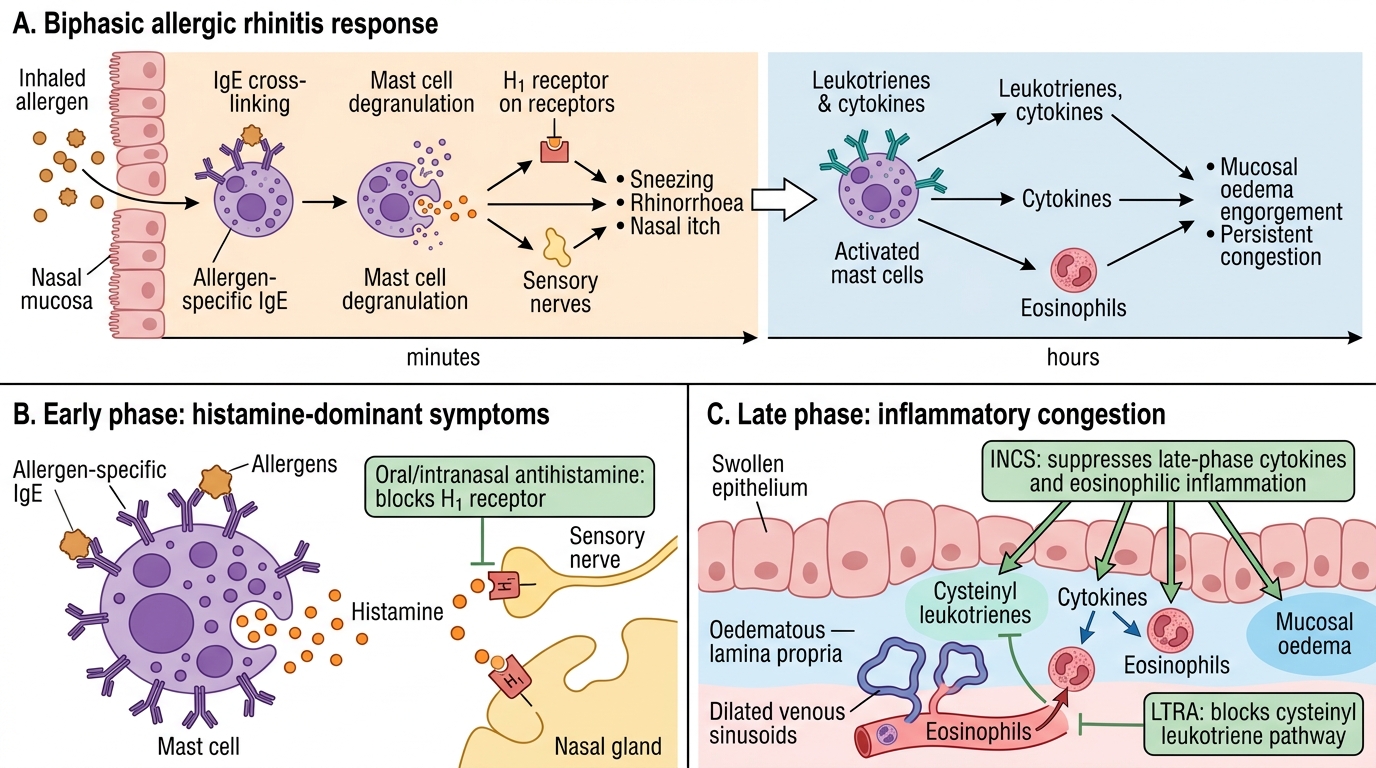
The pathophysiology of allergic rhinitis is a two-phase IgE-mediated immune response that explains both the immediate symptoms on allergen exposure and the chronic mucosal remodelling that causes persistent obstruction. Understanding the two phases allows you to predict which drugs work at which stage — a direct link between mechanism and pharmacotherapy. This is not merely academic: when a patient asks why their antihistamine helps sneezing but not their blocked nose, the answer is in the two phases — the early phase (histamine-driven, antihistamine-sensitive) versus the late phase (leukotriene/cytokine-driven, INCS-sensitive). Patients who understand this are more adherent to INCS therapy, which requires daily use over weeks for full benefit.
The early-phase reaction (within seconds to 30 minutes of allergen exposure) is driven by mast cell degranulation releasing histamine and other preformed mediators. Histamine acts on H1 receptors in the nasal mucosa to produce:
- Increased vascular permeability → watery rhinorrhoea
- Vasodilation of submucosal sinusoids → congestion
- Stimulation of sensory nerve endings → itch and sneezing reflex
Antihistamines (H1-receptor antagonists) work primarily at this phase — they block histamine-mediated sneezing, rhinorrhoea, and itch but have limited effect on congestion (which is partly leukotriene-mediated).
The late-phase reaction (4–8 hours after exposure, lasting 12–24 hours) is driven by newly synthesised mediators — principally cysteinyl leukotrienes (LTC4, LTD4, LTE4) and cytokines (IL-4, IL-5, IL-13) — that recruit eosinophils, Th2 lymphocytes, and basophils into the nasal mucosa. This cellular infiltration causes persistent mucosal oedema (nasal obstruction) and priming of the mucosa for exaggerated responses to subsequent exposures. Intranasal corticosteroids (INCS) work at this level — they suppress the late-phase inflammatory cascade, reduce eosinophil infiltration, and decrease mucosal oedema. This is why INCS take 2–4 weeks for full effect and are superior to antihistamines for nasal obstruction.
Nasal hyperreactivity: After repeated allergen exposures, the nasal mucosa becomes primed and hyper-reactive — triggering symptoms in response to non-allergic stimuli (cold air, strong smells, smoke, exercise). This primed state is the mechanism behind the 'entanglement' of allergic and vasomotor rhinitis, and is the reason patients often cannot identify a single trigger.
The united airway: The same Th2-dominant atopic inflammation occurs in the bronchial mucosa of asthma. Up to 40% of allergic rhinitis patients have co-existing asthma, and poorly controlled nasal disease worsens bronchial hyper-reactivity through nasal-bronchial reflexes and aspiration of nasal secretions. Treating rhinitis improves asthma control — clinically important.
Biphasic Mechanism of Allergic Rhinitis and Drug Targets
SELF-CHECK
A 25-year-old with allergic rhinitis complains that his oral antihistamine controls his sneezing and runny nose reasonably well but his nasal congestion remains severe throughout the day. The most likely reason is:
A. He has developed tolerance to antihistamines from prolonged use
B. Nasal congestion in allergic rhinitis is predominantly driven by the late-phase leukotriene/cytokine response, which antihistamines do not adequately address
C. Antihistamines are ineffective for any symptom of allergic rhinitis at standard doses
D. His congestion is due to a co-existing DNS that needs septoplasty
Reveal Answer
Answer: B. Nasal congestion in allergic rhinitis is predominantly driven by the late-phase leukotriene/cytokine response, which antihistamines do not adequately address
Sneezing, rhinorrhoea, and itch are primarily early-phase, histamine-mediated symptoms — antihistamines (H1-receptor antagonists) are effective for these. Nasal congestion, however, is predominantly driven by the late-phase reaction: leukotriene-mediated and cytokine-mediated mucosal oedema and eosinophil infiltration that persists for hours to days. Antihistamines have limited anti-congestion effect because they do not block leukotrienes or the late-phase inflammatory cascade. Intranasal corticosteroids (INCS) are superior for congestion because they suppress the late-phase response. Leukotriene receptor antagonists (montelukast) are a useful add-on for congestion, particularly when asthma co-exists.
Examination and Investigations
The clinical examination of a patient with allergic rhinitis reveals signs that directly reflect the underlying mucosal inflammation driven by histamine and eosinophilic infiltration. Recognising these signs on anterior rhinoscopy is the first step; investigations then confirm the diagnosis and identify the specific allergen triggers, which is important both for allergen avoidance counselling and for planning allergen immunotherapy. The examination also must actively look for complications of long-standing allergic rhinitis — nasal polyps, which develop in a subset of patients with severe, persistent, eosinophilic disease and cause anosmia and further obstruction beyond what the mucosal swelling alone produces. Identifying polyps on rhinoscopy changes the management plan significantly (adding or escalating INCS; considering FESS if polyps are large).
Anterior rhinoscopy findings in allergic rhinitis:
- Inferior turbinates: pale (greyish-white or bluish-white), swollen, and boggy — the pallor distinguishes allergic turbinate from infective (red, swollen) turbinate.
- Nasal mucosa: wet and glistening with watery secretions pooled in the nasal floor.
- Nasal polyps: in chronic, severe, long-standing allergic rhinitis, ethmoidal polyps may develop — bilateral, multiple, pale grey, translucent masses arising from the middle meatus. Polyps cause anosmia and worsen obstruction. Note: polyps in allergic rhinitis are BILATERAL and MULTIPLE (ethmoidal type) — do NOT confuse with the unilateral, single antrochoanal (Killian's) polyp.
- Septal deviation: may coexist and compound obstruction.
The allergic salute and transverse nasal crease: chronic upward rubbing of the nose (to relieve itch) creates a horizontal crease across the lower third of the nose — a clinical sign of long-standing allergic rhinitis in children.
Investigations:
- Skin prick test (SPT): the gold standard for identifying IgE-mediated sensitisation. Small amounts of allergen extracts are applied to the forearm skin via a lancet prick. A wheal-and-flare response (≥3 mm diameter) at 15 minutes indicates sensitisation. The SPT tests multiple allergens simultaneously (HDM, cockroach, grass pollen, tree pollen, animal dander, mould). Simple, inexpensive, immediate results. Avoid if the patient is on antihistamines (within 72 hours) — antihistamines suppress the wheal response.
- Serum-specific IgE (sIgE, RAST/ImmunoCAP): blood test measuring IgE antibodies to specific allergens; preferred when SPT is not available, in children who cannot cooperate with skin testing, or when the patient cannot stop antihistamines. More expensive than SPT.
- Total serum IgE: elevated in atopic individuals (>100 IU/mL); non-specific — elevated also in parasitic infections, very common in India. Not useful for identifying specific allergens.
- Nasal cytology (nasal smear): a nasal smear stained with Giemsa or Hansel's stain showing >10–25% eosinophils supports an allergic aetiology.
- CT PNS: not required for uncomplicated allergic rhinitis; indicated if nasal polyps or sinusitis are suspected on clinical grounds.