Page 11 of 29
EN4.24 | Allergic Rhinitis — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The diagnosis of allergic rhinitis is clinical in most cases — the characteristic combination of the four cardinal symptoms (sneezing, watery rhinorrhoea, nasal itch, bilateral obstruction), pale boggy turbinates, positive personal or family history of atopy, and allergen-specific symptoms confirmed by SPT is sufficient. The investigation role is to confirm the diagnosis when the clinical picture is uncertain and to identify specific allergens for targeted management. The most important diagnostic discipline is to distinguish allergic rhinitis from vasomotor rhinitis, because the two conditions look superficially similar on rhinoscopy (both have turbinate hypertrophy) but respond to entirely different treatments — a patient with vasomotor rhinitis will not benefit from an allergy workup, allergen avoidance, or immunotherapy, and the approach must shift to neural hyperreactivity management. The key differentiating features are in the history, not the examination.
The differential diagnosis for rhinitis includes several important conditions that share nasal symptoms but have different pathophysiology and management:
- Vasomotor rhinitis (non-allergic rhinitis): perennial, bilateral nasal obstruction and rhinorrhoea without sneezing, itch, or eye symptoms; triggers are non-allergen (cold air, perfumes, smoke, humidity changes); allergy tests negative; turbinates hypertrophied but not as pale as in allergic rhinitis. Key distinguisher: no itch, no sneezing, negative allergy test.
- Acute viral rhinitis (common cold): infectious onset, associated fever, sore throat, systemic symptoms; lasts 5–10 days; self-limiting; clear discharge that becomes mucopurulent.
- Chronic rhinosinusitis (CRS): thick mucopurulent discharge, facial pain/pressure, hyposmia; CT PNS shows sinus mucosal thickening; responds to nasal irrigation and antibiotic courses; some CRS is allergic (CRS with polyps).
- Rhinitis medicamentosa: rebound congestion from prolonged topical decongestant use; no sneezing/itch; relieved only by the decongestant; negative allergy test.
- Non-allergic rhinitis with eosinophilia syndrome (NARES): eosinophilia on nasal smear but negative allergy tests; may respond to INCS.
- Nasal polyps (ethmoidal polyposis): bilateral pale grey masses from the middle meatus; anosmia; associated with allergic rhinitis and aspirin sensitivity (Samter's triad — polyps + asthma + aspirin sensitivity).
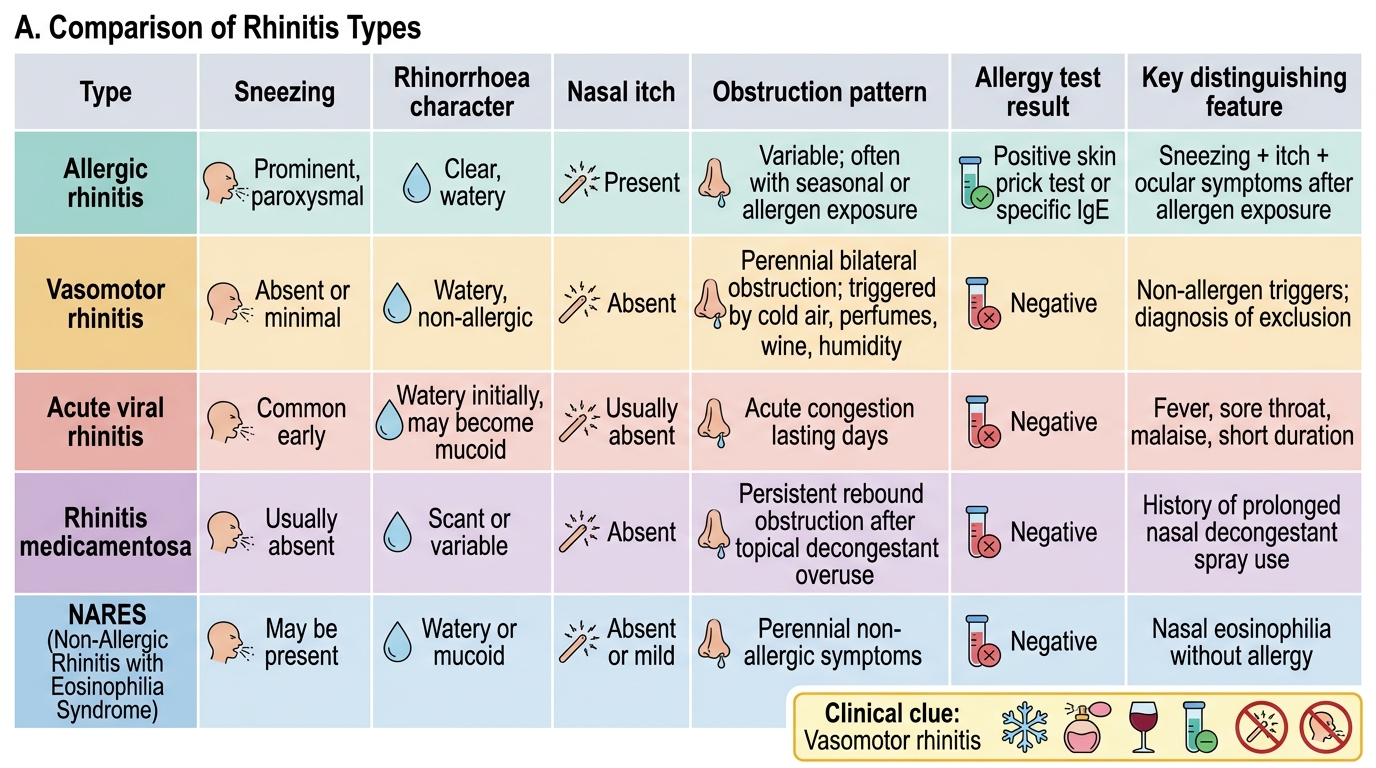
Comparison of Rhinitis Types
SELF-CHECK
A 30-year-old patient with a 5-year history of nasal symptoms — bilateral obstruction, rhinorrhoea, and post-nasal drip — reports that symptoms are worst on entering cold or air-conditioned environments, after drinking wine, and when exposed to perfumes. There is no sneezing, no ocular symptoms, and no seasonal variation. Skin prick test is negative to all 20 common allergens. The most likely diagnosis is:
A. Intermittent allergic rhinitis — false-negative SPT
B. Vasomotor rhinitis (non-allergic rhinitis)
C. Rhinitis medicamentosa from over-the-counter nasal sprays
D. Chronic rhinosinusitis with polyps
Reveal Answer
Answer: B. Vasomotor rhinitis (non-allergic rhinitis)
The classic features of vasomotor rhinitis are: perennial bilateral nasal obstruction and rhinorrhoea WITHOUT sneezing, without nasal itch, without eye symptoms, and without a seasonal pattern; triggered by non-allergen stimuli (cold, humidity, perfumes, wine, exercise, emotional stress); and negative allergy tests. This contrasts with allergic rhinitis where sneezing, itch, and eye symptoms are prominent, and the SPT is positive. Vasomotor rhinitis is a diagnosis of exclusion — allergic, infectious, and drug-related causes must be ruled out first.
Principles of Management
The management of allergic rhinitis follows a stepped approach based on symptom severity (ARIA classification), allergen trigger identification, and comorbidities (asthma, sinusitis, polyps). Three pillars underpin management: allergen avoidance, pharmacotherapy, and allergen immunotherapy. The choice among them depends on whether the trigger can be avoided, which symptoms dominate, and whether the disease is intermittent or persistent.
Pillar 1 — Allergen avoidance:
The most effective but often most difficult intervention. For house dust mite (HDM): impermeable mattress and pillow covers, washing bedding at 60°C weekly, reducing soft furnishings, HEPA filter vacuuming. For pollen: staying indoors during high-pollen count days, keeping windows closed, wearing wraparound sunglasses. For animal dander: removing the pet (hard to achieve) or at minimum keeping it out of the bedroom. Avoidance alone is rarely sufficient but reduces the allergen load and improves pharmacotherapy effectiveness.
Pillar 2 — Pharmacotherapy:
Intranasal corticosteroids (INCS) — mometasone furoate, fluticasone propionate/furoate, budesonide — are the most effective pharmacological treatment for persistent or moderate-severe allergic rhinitis. They reduce all four symptoms (obstruction, rhinorrhoea, sneezing, itch) and, uniquely, are effective for nasal obstruction (unlike antihistamines). Require 2–4 weeks of regular use for full effect. Minimal systemic absorption at standard doses. First-line treatment for moderate-severe persistent allergic rhinitis.
Oral antihistamines (H1-receptor antagonists): second-generation (non-sedating) agents — cetirizine, loratadine, fexofenadine, desloratadine — are first-line for mild intermittent or predominantly sneezing/rhinorrhoea-type symptoms. Provide rapid relief (within 1 hour). Less effective for nasal obstruction than INCS.
Intranasal antihistamines (azelastine): faster onset than oral antihistamines (minutes), useful for on-demand relief; modest anti-inflammatory effect beyond H1-blockade.
Leukotriene receptor antagonists (LTRAs) (montelukast): useful add-on therapy, particularly when allergic rhinitis co-exists with asthma (a single agent treats both). Effective for congestion (leukotrienes drive late-phase obstruction).
Oral decongestants (pseudoephedrine): rapid relief of congestion; short-term use only (cardiovascular side effects — tachycardia, hypertension — limit long-term use).
Combination INCS + antihistamine: additive benefit for patients not controlled on monotherapy; some intranasal combinations (azelastine + fluticasone) are available.
Pillar 3 — Allergen immunotherapy (AIT):
The only treatment that modifies the underlying immune response and provides long-term disease modification (symptom relief persisting years after stopping treatment). AIT works by inducing allergen tolerance via generation of regulatory T cells and IgG4 'blocking antibodies' that compete with IgE. Available as:
- Subcutaneous immunotherapy (SCIT): monthly injections of gradually increasing allergen doses over 3–5 years; requires specialist supervision.
- Sublingual immunotherapy (SLIT): daily allergen tablets or drops under the tongue; self-administered at home; good evidence for HDM, grass, and tree pollen.
Indications for AIT: moderate-severe persistent allergic rhinitis not adequately controlled with pharmacotherapy; documented specific IgE sensitisation; preference for long-term disease modification over lifelong pharmacotherapy.
CLINICAL PEARL
The most common management error in allergic rhinitis is prescribing a sedating first-generation antihistamine (chlorpheniramine) as first-line therapy. Chlorpheniramine crosses the blood-brain barrier, causes sedation, and impairs cognitive function and driving — it worsens the very quality-of-life impairments the patient is consulting for. Second-generation antihistamines (cetirizine, loratadine, fexofenadine) are non-sedating at standard doses, pharmacologically superior (longer half-life, more selective H1 blockade), and are the correct first choice. Reserve chlorpheniramine for acute urticaria or when sedation is deliberately intended (e.g. a patient who needs to sleep through an unavoidable allergen exposure).
Self-Assessment
Apply your understanding of this module to the following clinical scenario before attempting the quiz questions below:
A 28-year-old woman with a 10-year history of year-round sneezing, watery rhinorrhoea, and nasal obstruction also has mild exercise-triggered wheeze. She has been on cetirizine daily for 5 years with good control of sneezing but persistent bilateral nasal obstruction that worsens in the afternoon. SPT is strongly positive for house dust mite and cockroach, weakly positive for grass pollen. Nasal endoscopy shows bilateral pale grey polyps in the middle meatus.
Classify her allergic rhinitis by ARIA criteria. Why does her antihistamine not control her obstruction? What is the implication of the nasal polyps? List her treatment priorities in order. What investigation would she need before you consider allergen immunotherapy?
SELF-CHECK
Which of the following is the most appropriate first-line pharmacotherapy for a 20-year-old university student with persistent moderate-severe allergic rhinitis (perennial, HDM-triggered) who is most bothered by bilateral nasal congestion and has poor sleep quality?
A. Oral chlorpheniramine 4 mg three times daily
B. Daily intranasal mometasone furoate spray
C. Daily oral cetirizine 10 mg
D. Pseudoephedrine 60 mg twice daily as needed
Reveal Answer
Answer: B. Daily intranasal mometasone furoate spray
For persistent moderate-severe allergic rhinitis with nasal congestion as the dominant symptom, intranasal corticosteroids (INCS) such as mometasone furoate are the most effective pharmacological treatment and are the ARIA-guideline recommended first-line therapy. INCS suppress both early- and late-phase inflammation, address all four symptoms including congestion, and improve sleep quality. Oral cetirizine (a non-sedating antihistamine) is first-line for mild intermittent rhinitis or when sneezing/rhinorrhoea dominate, but is inferior to INCS for congestion. Chlorpheniramine (first-generation antihistamine) is sedating and therefore inappropriate for a student needing to function academically. Pseudoephedrine provides short-term congestion relief but is not appropriate for daily use due to cardiovascular side effects and rebound.