Page 8 of 15
EN3.3 | Rigid Flexible Laryngoscopy — SDL Guide
Learning Objectives
- State the clinical indications for laryngoscopy including the critical threshold of persistent hoarseness exceeding three weeks
- Describe the three principal laryngoscopy instruments — rigid 70° Hopkins rod (transoral indirect), flexible nasopharyngolaryngoscope, and rigid direct laryngoscope — and their respective clinical roles
- Describe the step-by-step technique of flexible nasopharyngolaryngoscopy and rigid indirect laryngoscopy (70° Hopkins rod), including patient positioning, preparation, and systematic survey of the larynx
- Interpret key laryngoscopic findings including normal vocal cord appearance and movement, unilateral vocal cord palsy, glottic and supraglottic carcinoma, Reinke's oedema, and vocal cord nodules
- Distinguish glottic from supraglottic laryngeal carcinoma by endoscopic presentation, pattern of spread, and prognosis, including the significance of the left recurrent laryngeal nerve's intrathoracic course
INSTRUCTIONS
Laryngoscopy — direct visualisation of the larynx — is one of the most clinically consequential skills in ENT. The decision to perform laryngoscopy on a patient with persistent hoarseness is the intervention that converts a vague symptom into a diagnosis; in the case of laryngeal carcinoma, it is the investigation that determines whether the patient is curable or not. The NMC EN3.3 competency requires you to observe and describe the indications and steps of both rigid and flexible laryngoscopy. As a final-year student you will observe this procedure during your ENT clinical posting; your ability to understand the instruments, interpret the findings you see on the monitor, and apply the key factual rules — particularly the three-week hoarseness threshold, the left recurrent laryngeal nerve anatomy, and the glottic vs supraglottic carcinoma distinction — is the clinical objective of this SDL.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 38: Clinical Methods of Examination of the Larynx; Ch. 40: Malignant Tumours of the Larynx (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat, 3rd ed., Ch. 20: Laryngoscopy and Microlaryngoscopy (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 3: Laryngology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old male retired schoolteacher presents with a six-week history of hoarseness. He has been a 30-pack-year smoker. His GP attributed the hoarseness to 'throat infection' and gave two courses of antibiotics. When he presents to ENT, you pick up the flexible nasopharyngolaryngoscope, pass it through the left nostril, advance it to the oropharynx, and look down at the laryngeal inlet. On the left true vocal cord, you see an irregular, pale, raised mucosal lesion at the mid-cord, approximately 8 mm across. The cord is moving. You document: 'Irregular mass on the left true vocal cord; cord mobile; consistent with early glottic carcinoma.' Six weeks of antibiotic treatment, and the diagnosis was waiting on the cord all along. This is why the three-week hoarseness rule exists. What does the laryngoscope show you, and how do you get to this view?
WHY THIS MATTERS
Laryngoscopy is the definitive examination for any patient with a laryngeal complaint, and persistent hoarseness is the most common laryngeal symptom. The clinical rule is unambiguous: hoarseness lasting more than three weeks in an adult requires laryngoscopy to exclude malignancy. This threshold exists because glottic carcinoma — the most common form of laryngeal cancer — produces hoarseness as its first and earliest symptom, at a stage when the tumour is still curable. Delaying laryngoscopy by attributing hoarseness to viral infection or acid reflux converts a potentially curable early glottic cancer into an inoperable one. Under EN3.3, you are expected to observe and describe laryngoscopy in your clinical posting and to understand both the instruments and the clinical logic behind the three-week threshold. Additionally, understanding vocal cord palsy — why the left cord is more often affected than the right, and what thoracic pathologies cause it — is essential for the differential diagnosis of a patient who presents with a breathy voice and a motionless left cord.
RECALL
Recall from your anatomy sessions the three regions of the larynx. The supraglottis comprises the epiglottis, the aryepiglottic folds, the arytenoids, and the false (vestibular) cords (ventricular folds). The glottis comprises the true vocal cords and the rima glottidis (the space between them). The subglottis extends from the inferior surface of the true cords to the lower border of the cricoid cartilage. The muscles of the larynx that move the vocal cords are innervated by the recurrent laryngeal nerve (RLN), a branch of the vagus nerve. The left RLN has a significantly longer intrathoracic course than the right: it descends into the thorax, loops under and around the aortic arch (ligamentum arteriosum), and ascends in the tracheo-oesophageal groove to the larynx. The right RLN loops around the right subclavian artery in the neck and has a shorter extrathoracic course. The consequence is that the left RLN is vulnerable to compression or invasion by thoracic masses — lung carcinoma (particularly left-sided apical tumours), aortic aneurysm, enlarged mediastinal lymph nodes, and cardiac surgery.
Clinical Indications for Laryngoscopy
Laryngoscopy is indicated whenever a clinical history or examination suggests laryngeal pathology that cannot be assessed without direct visualisation. The larynx lies behind the tongue and cannot be inspected by any other means. While a clinical history and neck examination provide important clues, only direct laryngoscopy answers the question: 'Is there a structural abnormality of the vocal cords?' This question matters most when the answer could be laryngeal carcinoma. The larynx is a highly specialised structure responsible for phonation, airway protection during swallowing, and (via subglottic pressure) forced expiration. Symptoms that arise from laryngeal pathology — hoarseness, dysphagia, stridor, referred ear pain, or voice fatigue — therefore carry a broad differential that spans benign vocal cord lesions, inflammatory conditions, functional disorders, and malignancy. Because these symptoms cannot be further characterised without direct visual inspection, the threshold for performing laryngoscopy in clinical practice is deliberately low. The following indications represent the full range of clinical scenarios in which laryngoscopy is the diagnostic standard and should be requested without delay.
Voice disorders:
- Persistent hoarseness exceeding 3 weeks in any adult: this is the critical clinical threshold. Hoarseness persisting beyond three weeks requires laryngoscopy to exclude laryngeal carcinoma. This rule is non-negotiable — the most common cause of chronic hoarseness that is missed until late presentation is glottic carcinoma diagnosed as 'chronic laryngitis.' Do not wait beyond three weeks.
- Change in voice quality (breathiness, roughness, voice fatigue) in professional voice users (teachers, singers, actors) — even without hoarseness exceeding three weeks
- Sudden or progressive voice deterioration
Suspected laryngeal malignancy:
- Any patient with hoarseness, dysphagia, referred otalgia (pain referred to the ear via Arnold's nerve — the auricular branch of the vagus), or unexplained neck lymphadenopathy — laryngoscopy followed by biopsy if a lesion is found
- Haemoptysis with laryngeal cause
Vocal cord palsy:
- Breathy or bovine voice, absent cough reflex, aspiration — assessment of cord mobility
- Known or suspected thoracic, neck, or skull-base pathology affecting the vagus or RLN
- Post-thyroid surgery, post-cardiac surgery, post-oesophagectomy
Airway assessment:
- Stridor (noisy breathing due to partial laryngeal or tracheal obstruction) — laryngoscopy to determine level (supraglottic, glottic, subglottic, tracheal)
- Suspected laryngeal foreign body
- Pre-anaesthetic airway assessment in a difficult airway patient
- Assessment of subglottic stenosis
Other indications:
- Laryngeal trauma (road traffic accident, assault, iatrogenic injury)
- Chronic cough when laryngopharyngeal reflux or posterior laryngitis is suspected
- Pre-operative assessment of laryngeal anatomy before thyroid or parathyroid surgery
Instruments: Rigid and Flexible Laryngoscopes
Three principal instruments are used for laryngoscopy in clinical practice, each with distinct optical principles, indications, and limitations. Understanding the differences between them allows you to know which instrument the surgeon is reaching for and why, and to describe the procedure accurately in an OSCE or examination setting. The choice of instrument is determined by the clinical purpose (diagnostic vs therapeutic), the patient's anatomy (gag reflex, neck mobility), and the available setting (outpatient clinic vs operating theatre).
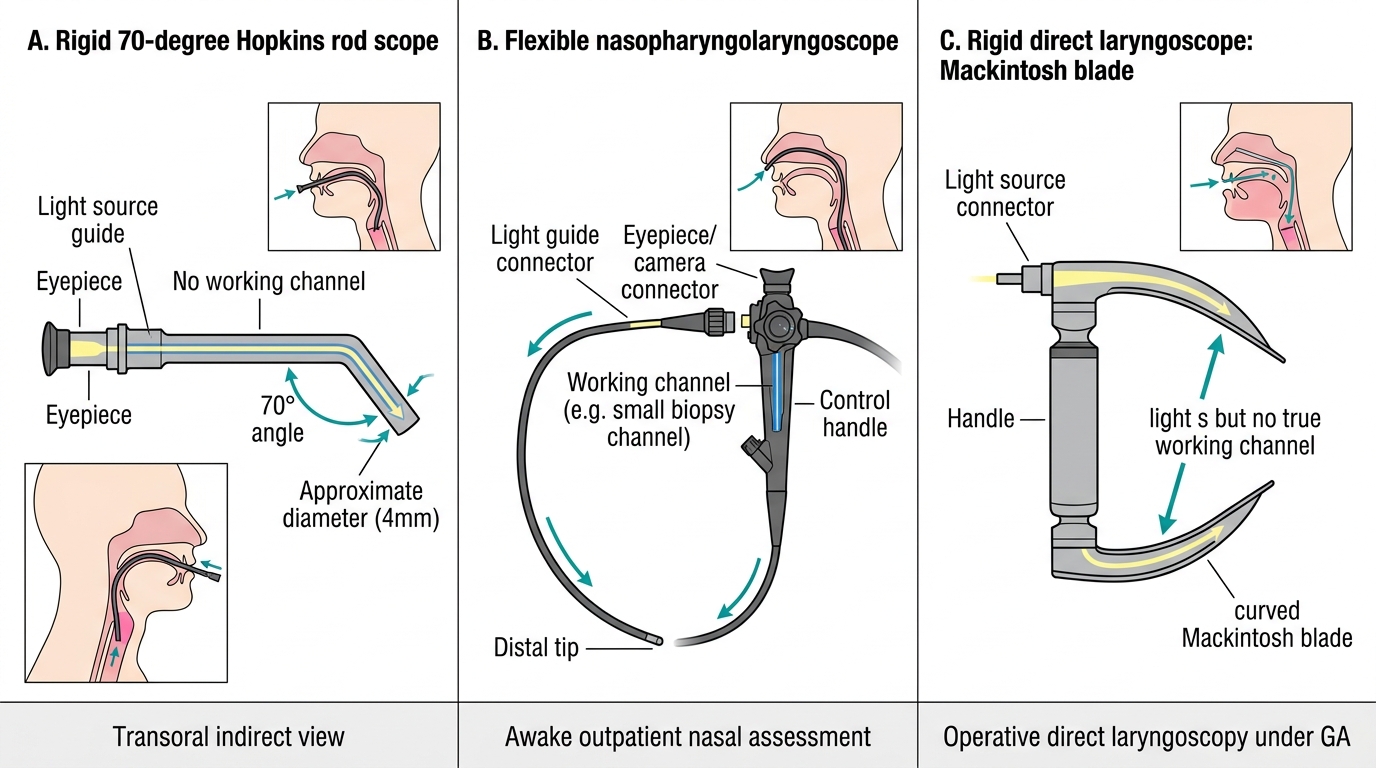
1. Flexible nasopharyngolaryngoscope (flexible laryngoscope):
This is the primary diagnostic instrument for outpatient laryngeal assessment. It is a thin (3–4 mm diameter) flexible fibre-optic or chip-tip endoscope with a distal bending section controlled by a thumb lever on the handle. It is passed through the nasal cavity (inferior meatus), through the pharynx, and down to the laryngeal inlet, where the true vocal cords are visualised from above. The patient remains awake, seated upright, and breathing through the nose throughout. The flexible scope's main advantages are patient comfort (no general anaesthesia), the ability to assess vocal cord mobility during phonation (the patient is awake and can follow commands — 'say E,' 'cough'), and the ability to pass through a narrow or restricted airway that would not accommodate a rigid instrument. Chip-tip (distal CCD) endoscopes provide superior image quality compared to older fibre-optic versions by placing the camera chip at the distal tip of the scope rather than transmitting the image through fibre bundles.
2. Rigid indirect laryngoscope (70° Hopkins rod — transoral):
A rigid 70° Hopkins rod telescope is passed through the open mouth, with the patient's tongue held forward with gauze, to a position above the oropharynx and below the soft palate, from which the larynx is viewed at a 70° angle. The image quality is excellent — higher resolution than a flexible scope — and the instrument is used in the outpatient clinic for detailed assessment of glottic lesions and for stroboscopy (dynamic assessment of mucosal wave vibration). Its disadvantage is that it requires a cooperative patient without a strong gag reflex, and it cannot be passed in cases of restricted mouth opening or a retroflexed epiglottis.
3. Rigid direct laryngoscope (Mackintosh/Lindholm — for microlaryngoscopy):
A rigid metal laryngoscope blade is passed through the mouth under general anaesthesia with the patient supine and the neck extended (the 'sniffing' position), directly lifting the epiglottis to expose the laryngeal inlet and the true cords. The surgeon then uses an operating microscope for magnified inspection and micro-instruments (Kleinsasser forceps, CO2 laser) for biopsy and surgery. This is the direct laryngoscopy under GA (also called microlaryngoscopy or suspension laryngoscopy) used for biopsy of laryngeal lesions, laser resection, and vocal cord surgery. It is not a diagnostic outpatient procedure — it is the operative procedure that follows a diagnostic flexible laryngoscopy showing a suspicious lesion.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Comparison of Common Laryngoscopy Instruments
SELF-CHECK
A 45-year-old woman with a hoarse voice for 5 weeks is referred to the ENT outpatient clinic. She is cooperative and has no gag problem. The most appropriate laryngoscopy instrument for her initial diagnostic assessment in the outpatient clinic is:
A. Rigid direct laryngoscope under general anaesthesia with microscopic magnification
B. Flexible nasopharyngolaryngoscope passed through the nasal cavity while the patient is awake
C. Rigid 70° Hopkins rod scope passed transorally with the patient fully paralysed
D. Plain soft tissue X-ray of the neck to look for laryngeal mass before endoscopy
Reveal Answer
Answer: B. Flexible nasopharyngolaryngoscope passed through the nasal cavity while the patient is awake
Flexible nasopharyngolaryngoscopy is the standard outpatient diagnostic tool for laryngeal assessment. It requires no general anaesthesia, can be performed in the awake cooperative patient, allows assessment of vocal cord mobility during phonation (the patient can follow voice commands), and is well tolerated. Rigid direct laryngoscopy under GA is the operative procedure used after a suspicious lesion is found on flexible laryngoscopy, for biopsy and microsurgery — not for initial diagnosis. The 70° Hopkins rod transoral scope is used for specific indications (stroboscopy, detailed glottic inspection) and requires patient cooperation without gag reflex. Plain X-ray cannot visualise mucosal laryngeal pathology.
Procedure: Flexible Nasopharyngolaryngoscopy
Flexible nasopharyngolaryngoscopy is the workhorse outpatient procedure for laryngeal assessment. When you observe it in your ENT posting, understanding each step allows you to follow the procedure actively and to communicate findings accurately. The procedure takes approximately 5–10 minutes in a cooperative adult and is well tolerated with adequate preparation.
Preparation:
Apply xylometazoline 0.1% nasal decongestant to the nostril to be used (usually the more patent side as assessed by asking the patient or by brief anterior rhinoscopy). Wait 5 minutes. Apply 4% lignocaine spray to the nasal cavity and oropharynx. The nasal decongestant widens the inferior meatus for comfortable scope passage; the lignocaine reduces discomfort and gag reflex. The scope's distal tip can be warmed or treated with anti-fog solution before insertion to prevent condensation obscuring the image at body temperature.
Patient positioning:
The patient sits upright in the ENT chair at approximately 90°, head in neutral position or very slightly forward. Do not tilt the head back — a backward tilt makes the larynx move posteriorly and may obscure the view. The surgeon sits or stands facing the patient.
Passing the scope:
With the scope held in the dominant hand and the bending lever accessible, introduce the tip gently into the selected nostril, directing it along the floor of the nasal cavity (inferior meatus) — the inferior meatus is the most patent space in most patients. Advance steadily under vision, noting the inferior turbinate above. When the nasopharynx is reached, survey the adenoid, torus tubarius, and fossa of Rosenmüller bilaterally as the scope passes through. Continue advancing — the oropharynx and soft palate come into view, followed by the base of tongue and the epiglottis.
Laryngeal survey:
With the scope tip at the level of the oropharynx, bend the distal end slightly downward using the thumb lever to look over the base of tongue and visualise the laryngeal inlet. Identify the following structures from peripheral to central:
- Epiglottis (anterior, omega-shaped or curled — may obscure the anterior larynx if large or retroflexed)
- Aryepiglottic folds (lateral margins of the laryngeal inlet, leading from the epiglottis to the arytenoids)
- False (vestibular) cords (pink, lateral, below the aryepiglottic folds)
- True vocal cords (pearly white, medial, below the false cords — the key structures)
- Rima glottidis (the gap between the true cords — should be diamond-shaped on full abduction)
- Arytenoids (posterior, move medially with adduction and laterally with abduction)
Dynamic assessment:
Ask the patient to say 'E' (or 'eee') — both true vocal cords should adduct (come together) symmetrically. Ask the patient to breathe in deeply — both cords should abduct (move apart) symmetrically. Ask the patient to cough — note the laryngeal closure reflex. Any asymmetry, immobility, or abnormal mass or mucosal lesion is documented.
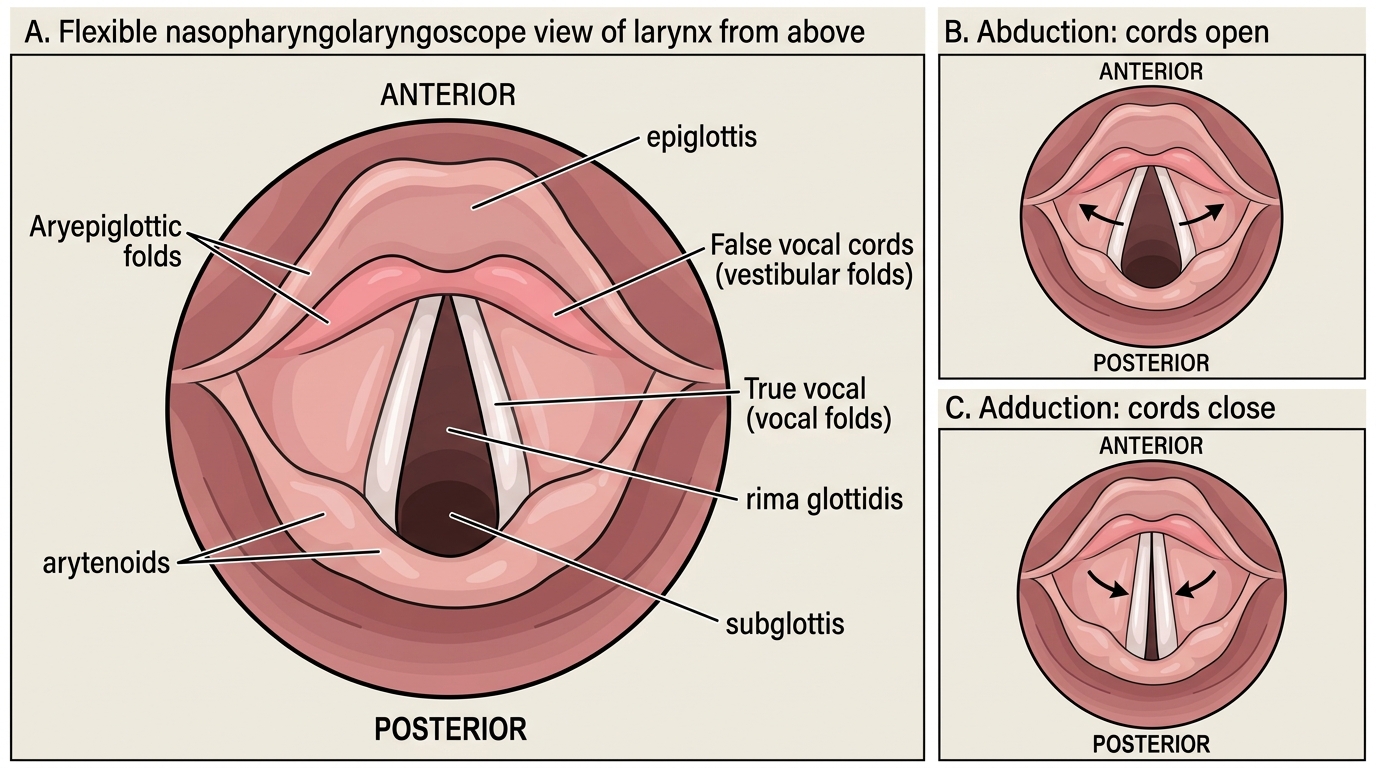
Flexible Laryngoscopic View of the Larynx