Page 9 of 15
EN3.3 | Rigid Flexible Laryngoscopy — SDL Guide (Part 2)
Procedure: Rigid Indirect Laryngoscopy (70° Hopkins Rod)
Rigid indirect laryngoscopy using the 70° Hopkins rod telescope provides higher-resolution images of the larynx than the flexible scope and is the preferred instrument for detailed assessment of the glottis, including mucosal lesion characterisation and stroboscopic examination of the vocal cord mucosal wave. The technique is performed transorally with the patient awake and seated, without passage through the nasal cavity.
Patient positioning:
The patient sits upright with the neck slightly extended (the 'sniffing the morning air' position) — this aligns the oral cavity, pharynx, and larynx into a more direct line of sight. The mouth is fully open. If the patient has a prominent gag reflex, topical lignocaine spray applied to the posterior tongue and oropharynx 5 minutes before the procedure is essential.
Tongue traction:
The patient's tongue is held firmly forward and downward by the examiner (using a gauze square wrapped around the tongue and gripped between the examiner's thumb and index finger). This prevents the tongue from retracting into the oropharynx and blocking the view. The patient must relax and not pull the tongue back — explaining this beforehand reduces the struggle.
Scope introduction:
The 70° Hopkins rod laryngoscope is introduced into the oropharynx with the non-dominant hand, guiding the tip gently to the posterior oropharynx just in front of the posterior pharyngeal wall. The scope is angled at 70° — looking upward and forward, toward the larynx, which sits anterior to the oesophageal inlet. A camera system on the eyepiece projects the image to a monitor.
Laryngeal survey:
Once the larynx is in view, survey the epiglottis, aryepiglottic folds, false cords, true vocal cords (pearly white, medial), rima glottidis, arytenoids, and the piriform fossae (lateral to the aryepiglottic folds — an important site for hypopharyngeal tumour). Ask the patient to produce a sustained 'E' sound to assess cord adduction, and to inspire to assess abduction.
Stroboscopy:
Attaching a stroboscopic light source to the Hopkins rod scope allows slow-motion visualisation of the vocal cord mucosal wave — the travelling wave of mucosal vibration during phonation. Normal cords show a complete, symmetrical mucosal wave. In early glottic carcinoma, the mucosal wave is reduced or absent over the lesion (the stiffened mucosa no longer vibrates normally) — this finding identifies an apparently small lesion as potentially invasive, and is not detectable with standard non-stroboscopic illumination. Stroboscopy is the voice clinic's investigation for differentiating benign lesions (preserved mucosal wave) from potentially malignant ones (absent or asymmetric wave).
SELF-CHECK
A 62-year-old male with a 4-week history of hoarseness undergoes flexible nasopharyngolaryngoscopy. On saying 'E,' the left true vocal cord fails to adduct and remains in the paramedian position, while the right cord crosses the midline to compensate. The most likely anatomical explanation for the left cord palsy is:
A. Right recurrent laryngeal nerve palsy from a cervical spine lesion compressing the nerve in the neck
B. Left recurrent laryngeal nerve palsy — the left RLN has a longer intrathoracic course, looping around the aortic arch, making it vulnerable to thoracic pathology
C. Bilateral vocal cord palsy due to a central brainstem lesion affecting both vagus nerves
D. Left superior laryngeal nerve palsy from a thyroid swelling compressing the external branch
Reveal Answer
Answer: B. Left recurrent laryngeal nerve palsy — the left RLN has a longer intrathoracic course, looping around the aortic arch, making it vulnerable to thoracic pathology
Unilateral left vocal cord palsy with the cord in the paramedian position, with compensatory right cord crossing to the midline ('compensation'), is the classic endoscopic picture of left RLN palsy. The left RLN has a longer intrathoracic course — it descends into the thorax, loops under the aortic arch, and ascends in the tracheo-oesophageal groove — making it vulnerable to thoracic causes: left apical lung carcinoma (Pancoast tumour), aortic aneurysm, enlarged mediastinal nodes, and cardiac/oesophageal surgery. In any patient with unexplained left vocal cord palsy, chest X-ray and CT of the neck and thorax is mandatory to exclude an underlying malignancy. The right RLN loops around the right subclavian artery in the neck and is more often affected by neck pathology (thyroid, neck nodes).
Interpretation of Laryngoscopic Findings
Accurate interpretation of laryngoscopic findings requires systematic inspection of each laryngeal region — not only the true cords — and integration of dynamic observations (cord mobility) with static mucosal appearances. The most important clinical decisions based on laryngoscopic findings are: is there a malignant lesion that needs urgent biopsy? Is there a vocal cord palsy whose cause needs further investigation? Is there a benign vocal cord lesion that needs voice therapy or microlaryngoscopy?
Provided image
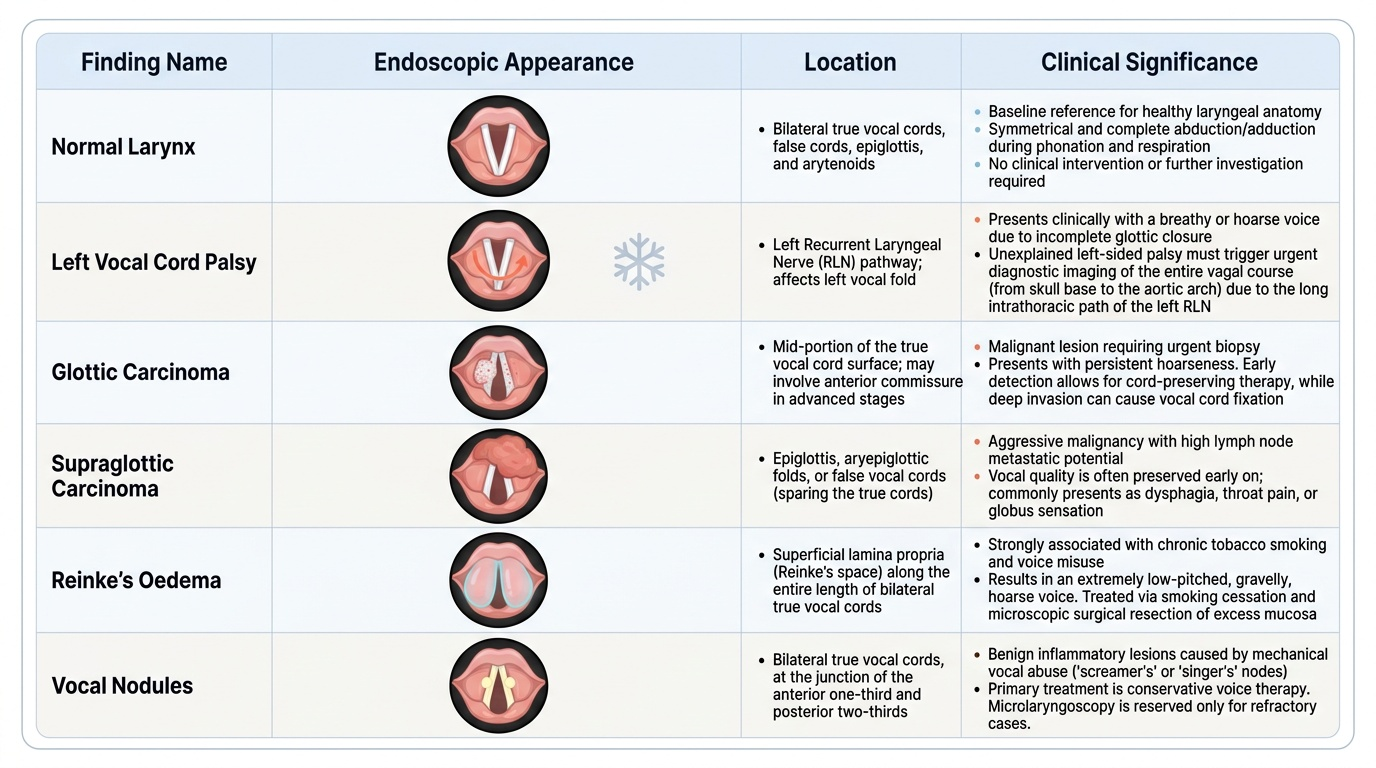
Normal larynx:
The true vocal cords are pearly white, smooth, and sharply marginated. They are symmetrical in size and position. On phonation ('E'), both cords adduct to the midline simultaneously and completely, closing the rima glottidis. On inspiration, both cords abduct symmetrically to open the rima glottidis in a diamond shape. The false (vestibular) cords are pink, slightly lateral, and do not move into the glottis normally. The epiglottis is pale pink and curves anteriorly. The arytenoids are mound-shaped, posteriorly placed, and move laterally and medially with abduction/adduction. The piriform fossae are visible lateral to the aryepiglottic folds — should be smooth and symmetrical.
Vocal cord palsy:
Unilateral vocal cord palsy presents on laryngoscopy as one cord remaining stationary in the paramedian or intermediate (cadaveric) position during both phonation and respiration — the affected cord does not adduct on phonation and does not abduct on inspiration. The contralateral cord may cross the midline to compensate (adducts beyond midline toward the affected side), which partially restores voice. The voice is breathy or hoarse because the cords do not fully close. Left-sided palsy is more common than right-sided because the left RLN's longer intrathoracic course exposes it to more pathologies. Any unexplained unilateral cord palsy requires imaging of the entire vagal course from skull base to the aortic arch.
Glottic carcinoma:
Appears as an irregular, raised, or ulcerated mucosal lesion on the true vocal cord surface, most commonly at the mid-cord. The cord surface is white, irregular, or nodular — the normal pearly-white smooth mucosa is disrupted. Early lesions are confined to the surface; advanced lesions may cross the anterior commissure, involve the subglottis, or fix the cord (invasive). Cord fixity — inability to abduct or adduct the cord — indicates invasion of the cricoarytenoid joint or paraglottic space, which upstages the tumour significantly. Glottic carcinoma classically presents with early hoarseness (because even a small cord lesion disrupts the mucosal wave) and has good prognosis because of the poor lymphatic supply of the vocal cord surface — nodal spread is late. This is why the three-week hoarseness rule is so valuable: catching glottic carcinoma at T1 (cord mobile, lesion confined) is associated with very high cure rates.
Supraglottic carcinoma:
Appears as a mass on the epiglottis, aryepiglottic fold, or false cord. Presents late because the supraglottis has a rich lymphatic supply that allows early nodal spread before the primary lesion causes significant symptoms. The presenting complaint is often referred otalgia (ear pain via Arnold's nerve — the auricular branch of the vagus), dysphagia, or a neck lump from metastatic nodes. Hoarseness is a late symptom in supraglottic carcinoma, occurring only when the lesion grows large enough to involve the true cords. Prognosis is poorer than glottic carcinoma because of early bilateral nodal spread.
Reinke's oedema:
Bilateral, diffuse, gelatinous/polypoid swelling of the superficial lamina propria (Reinke's space) of both true vocal cords — the cords appear pale, translucent, and sausage-like. Strongly associated with cigarette smoking. Voice is markedly rough and lowered in pitch. Management: smoking cessation is mandatory (the oedema recurs if smoking continues); surgical aspiration or cordectomy under microlaryngoscopy if symptomatic.
Vocal cord nodules:
Bilateral symmetric small white fibrous nodules at the junction of the anterior one-third and posterior two-thirds of the true vocal cord — the point of maximum vibration impact. Associated with vocal abuse (teachers, singers, salespeople). Both cords are affected at the same point because the nodules on each cord impact each other during phonation. Voice is hoarse and breathy. Management: voice therapy first; microlaryngoscopy excision only if voice therapy fails.
Vocal cord polyp:
Usually unilateral, pedunculated or sessile, at the free edge of one vocal cord. Smooth, pale or red surface. Associated with vocal abuse or single episode of voice misuse. Management: microlaryngoscopic excision.
CLINICAL PEARL
Two rules from laryngoscopy must be memorised verbatim and applied without exception: (1) Persistent hoarseness >3 weeks = laryngoscopy to exclude malignancy. This rule is the diagnostic safety net for glottic carcinoma — the most curable head-and-neck cancer when caught early, and one of the least curable when caught late. Attributing hoarseness to reflux, viral laryngitis, or voice overuse without performing laryngoscopy is an indefensible clinical error after three weeks. (2) Left vocal cord palsy = image the entire left vagal and RLN course from skull base to aortic arch. The left RLN's long intrathoracic loop under the aortic arch means that a lung carcinoma, aortic aneurysm, or mediastinal node at the AP window can be the cause. A chest X-ray is the minimum investigation; CT neck and thorax is needed for any unexplained case.
Applied Practice: Case Scenarios
These three cases represent the core laryngoscopic presentations you will encounter in clinical practice. For each case, decide on the most likely laryngoscopic finding and the immediate management step before reading the discussion.
Case 1 — The teacher with 5 weeks of hoarseness:
A 52-year-old male primary school teacher presents with 5 weeks of progressive hoarseness. He is a 25-pack-year smoker. His GP noted inflamed posterior laryngeal wall on mirror examination and prescribed a proton pump inhibitor for 'laryngopharyngeal reflux.' No improvement. Flexible laryngoscopy: on the right true vocal cord, there is a small white irregular raised lesion at the mid-cord, approximately 6 mm. The cord is mobile. No cervical lymphadenopathy.
Interpretation: Irregular raised cord lesion, cord mobile — most consistent with early glottic carcinoma (T1). The hoarseness threshold (>3 weeks) was met at 5 weeks. Cord mobility confirms the lesion has not invaded the paraglottic space or cricoarytenoid joint.
Management: Urgent microlaryngoscopy under general anaesthesia for biopsy and histological diagnosis. If biopsy confirms squamous cell carcinoma, stage the tumour. T1 glottic carcinoma (cord mobile, lesion confined) can be treated by radiotherapy or CO2 laser microlaryngoscopic resection with high cure rates.
Case 2 — The patient with a breathy voice after cardiac surgery:
A 68-year-old woman underwent coronary artery bypass grafting via median sternotomy three months ago. She has had a persistently breathy voice and difficulty swallowing since surgery. Flexible laryngoscopy: the left true vocal cord is in the paramedian position on both phonation and inspiration — it neither adducts nor abducts. The right cord crosses the midline to compensate during phonation. No mucosal lesion. No neck mass.
Interpretation: Left vocal cord palsy, iatrogenic — likely secondary to left RLN injury during cardiac surgery (the left RLN passes near the pericardium and the surgical field of coronary bypass). Paramedian position indicates partial denervation (complete denervation places the cord in an intermediate/cadaveric position).
Management: Reassurance — most iatrogenic RLN injuries after cardiac surgery recover within 6–12 months. Speech therapy and swallowing assessment. Laryngeal electromyography (EMG) to assess RLN integrity. If no recovery at 12 months: medialisation laryngoplasty or injection augmentation to bulk up the paralysed cord and restore closure.
Case 3 — Reinke's oedema:
A 55-year-old woman who has smoked 20 cigarettes per day for 30 years presents with a progressively deepening, rough voice over 3 years. She describes her voice as 'like a man's voice.' Flexible laryngoscopy: both true vocal cords appear diffusely swollen, pale, and translucent — resembling two pale sausages filling the glottis. Both cords remain mobile. No discrete lesion.
Interpretation: Bilateral Reinke's oedema — characteristic diffuse gelatinous swelling of the superficial lamina propria (Reinke's space) of both vocal cords, classically associated with long-term smoking. The pitched-down rough voice reflects the mass-loading effect of oedematous cords on vibratory frequency.
Management: Smoking cessation is mandatory and is the first treatment — the oedema will recur if smoking continues. If voice quality is unacceptable after stopping smoking, microlaryngoscopic aspiration or cordoplasty to evacuate the oedema fluid. Biopsy to exclude malignant transformation if there are any suspicious areas on close inspection.
SELF-CHECK
A 60-year-old male smoker presents with 8 weeks of progressive hoarseness. Flexible laryngoscopy shows a white irregular mass on the left vocal cord with cord fixity (the cord does not move on phonation). The most important clinical implication of cord fixity in this patient is:
A. Cord fixity indicates Reinke's oedema, which is a benign and reversible finding in smokers
B. Cord fixity indicates invasion of the paraglottic space or cricoarytenoid joint, upstaging the laryngeal carcinoma beyond T1
C. Cord fixity is a normal variant in a long-term smoker and does not change the management
D. Cord fixity indicates a vocal cord polyp that has compressed the joint — it resolves after microlaryngoscopic polypectomy
Reveal Answer
Answer: B. Cord fixity indicates invasion of the paraglottic space or cricoarytenoid joint, upstaging the laryngeal carcinoma beyond T1
Cord fixity — failure of the affected cord to abduct or adduct — in the context of an irregular mass on the vocal cord indicates invasion of the cricoarytenoid joint, the paraglottic space, or the intrinsic laryngeal muscles. This is a critical finding that upstages laryngeal carcinoma from T1 (mobile cord, superficial lesion) to at least T3 (fixed cord, deep invasion). T3 glottic carcinoma requires a much more aggressive treatment strategy than T1 (partial laryngectomy or chemoradiotherapy rather than radiotherapy or endoscopic resection). Reinke's oedema also fixes the cord shape but does NOT cause fixity of cord motion — the cord still moves in oedema. Cord fixity is never a normal variant.
Self-Assessment
The questions below test the key knowledge points from this SDL, mapped to the EN-skills arc. Before your ENT clinical posting, you should be able to answer all six questions without reference. The most important single fact to retain from this SDL is the three-week hoarseness rule — it is the primary preventive tool against late presentation of curable laryngeal carcinoma, and its application (or failure to apply it) defines competent from incompetent laryngeal clinical assessment. The RLN anatomy question and the glottic versus supraglottic distinction are high-frequency examination topics; both appear in MBBS OSCE stations and clinical short cases nationwide. A student who can name all three laryngoscopy instruments but does not know which anatomical feature of the left RLN makes left cord palsy more common than right cord palsy — or who cannot explain why glottic carcinoma has a better prognosis than supraglottic carcinoma — has gaps in the interpretive knowledge that this SDL aims to build. Use these questions as a calibration tool before your posting, not a revision exercise after.
- State the clinical threshold that mandates laryngoscopy for a patient presenting with hoarseness. Explain why this threshold exists in terms of the natural history of glottic carcinoma.
- What are the three main laryngoscopy instruments used in ENT practice? For which clinical setting (outpatient vs theatre, awake vs GA) is each used?
- Describe the patient preparation before flexible nasopharyngolaryngoscopy, naming the agents used and the sequence of steps.
- During flexible laryngoscopy, you ask the patient to say 'E.' The right cord adducts normally but the left cord remains stationary in the paramedian position. State the diagnosis and name the anatomical reason why the left cord is more commonly affected than the right.
- Distinguish glottic carcinoma from supraglottic carcinoma: state where each arises, which presents earlier and why, which has the better prognosis and why, and the significance of cord fixity.
- A patient with bilateral gelatinous swelling of both vocal cords is found to be a 30-pack-year smoker. State the diagnosis, the first step in management, and the reason the first step is not surgery.