Page 8 of 15
PE1.3 | Developmental Milestones and Assessment — SDL Guide
Learning Objectives
- Define development and distinguish it from growth and maturation
- Describe age-precise normal developmental milestones across gross motor, fine motor/adaptive, language, and personal-social domains from birth to 5 years
- Explain the biological mechanisms and environmental factors that determine the pace and sequence of development
- Describe standardised developmental assessment tools used in India and explain their clinical application
- Identify features of global developmental delay, domain-specific delay, and developmental regression, and initiate appropriate referral
INSTRUCTIONS
Every child neurology consultation, every well-child visit, every developmental concern raised by a parent—all begin with the same question: 'Is this child's development on track?' Answering that question requires knowing what normal development looks like at each age, understanding what drives it, and knowing how to assess it systematically. This module provides that foundation. The milestone ages in this module are high-yield for clinical examinations and, more importantly, for real clinical decision-making that directly affects children's outcomes.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 3 (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 26–28 (textbook)
- Developmental and Behavioural Pediatrics, Bharat Kapila (textbook)
- IAP Standard Treatment Guidelines: Developmental Delay (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An 18-month-old boy is brought to the paediatric OPD. His mother says he is 'a bit slow.' He does not yet walk independently, does not point to objects, has no words, and does not wave bye-bye. The mother asks: 'Is this normal? All children develop differently, don't they?' You think: is this within normal variation, or is it a child who is already missing multiple milestones in multiple domains—and whose window for effective early intervention is closing? To answer, you need to know not just that a child 'should be walking by 18 months,' but the full age-precise developmental map across all four domains, and what it means when a child falls behind in more than one of them.
WHY THIS MATTERS
Developmental assessment is the paediatric equivalent of a neurological examination—it provides objective, reproducible information about the functional status of the developing brain. Developmental delay affects approximately 10% of children globally, and in India, factors including prematurity, malnutrition, recurrent infections, and poverty create a particularly high-risk environment. The rationale for early identification is compelling: neuroplasticity—the brain's capacity for reorganisation in response to experience—is greatest in the first three years of life. Interventions delivered during this critical window (speech therapy, physiotherapy, sensory integration, structured stimulation) are disproportionately effective compared with the same interventions delivered after age 5. Every month of undetected delay in a high-risk child is a month of lost neuroplasticity. The clinician who can recognise developmental delay early and refer appropriately is providing one of the most high-yield interventions in all of paediatrics.
RECALL
From Physiology, recall that neurological maturation follows two predictable directional sequences:
• Cephalocaudal sequence: control develops from head → neck → trunk → legs (hence head control before sitting before standing).
• Proximodistal sequence: control develops from shoulder → elbow → wrist → fingers (hence reaching before grasping before pincer).
From the preceding growth module, recall that development is qualitative acquisition of function (distinct from growth, which is quantitative increase in size). From your clinical exposure, recall that language is the most sensitive early marker of cognitive development—speech delay is often the presenting complaint in autism spectrum disorder, intellectual disability, and hearing impairment.
Why Developmental Assessment Matters: The Clinical Case for Milestone Monitoring
Developmental monitoring is the systematic longitudinal process of observing whether a child is meeting age-appropriate milestones across the four developmental domains at each clinical contact. It is distinct from developmental screening (a brief standardised test applied to all children at defined ages) and from developmental evaluation (a comprehensive multidisciplinary diagnostic assessment of a child who has failed screening). All three form a nested cascade: monitoring detects concerns, screening confirms them, and evaluation diagnoses and plans intervention.
The clinical importance of early detection is grounded in the concept of critical and sensitive periods in brain development. Certain developmental processes—language acquisition, binocular vision, emotional regulation—have windows during which the brain is maximally responsive to appropriate input. Absence of that input during the sensitive period results in permanent, often irreversible deficits. A child with bilateral hearing loss identified at 3 months and fitted with hearing aids and enrolled in early intervention will develop near-normal language; the same child identified at 3 years will face a language gap that years of subsequent therapy cannot fully close. The paediatrician who asks about milestones at every well-child visit is, in effect, the child's neuroplasticity guardian.
In India, developmental screening has been integrated into national programmes. The Rashtriya Bal Swasthya Karyakram (RBSK) provides community-level screening for developmental delays, disabilities, and deficiencies in children 0–18 years through dedicated mobile health teams at Anganwadis and schools. The four 'D's of RBSK are Defects at birth, Deficiencies, Diseases, and Developmental delays and disabilities. Understanding normal milestones is the prerequisite for any clinician participating in this surveillance system.
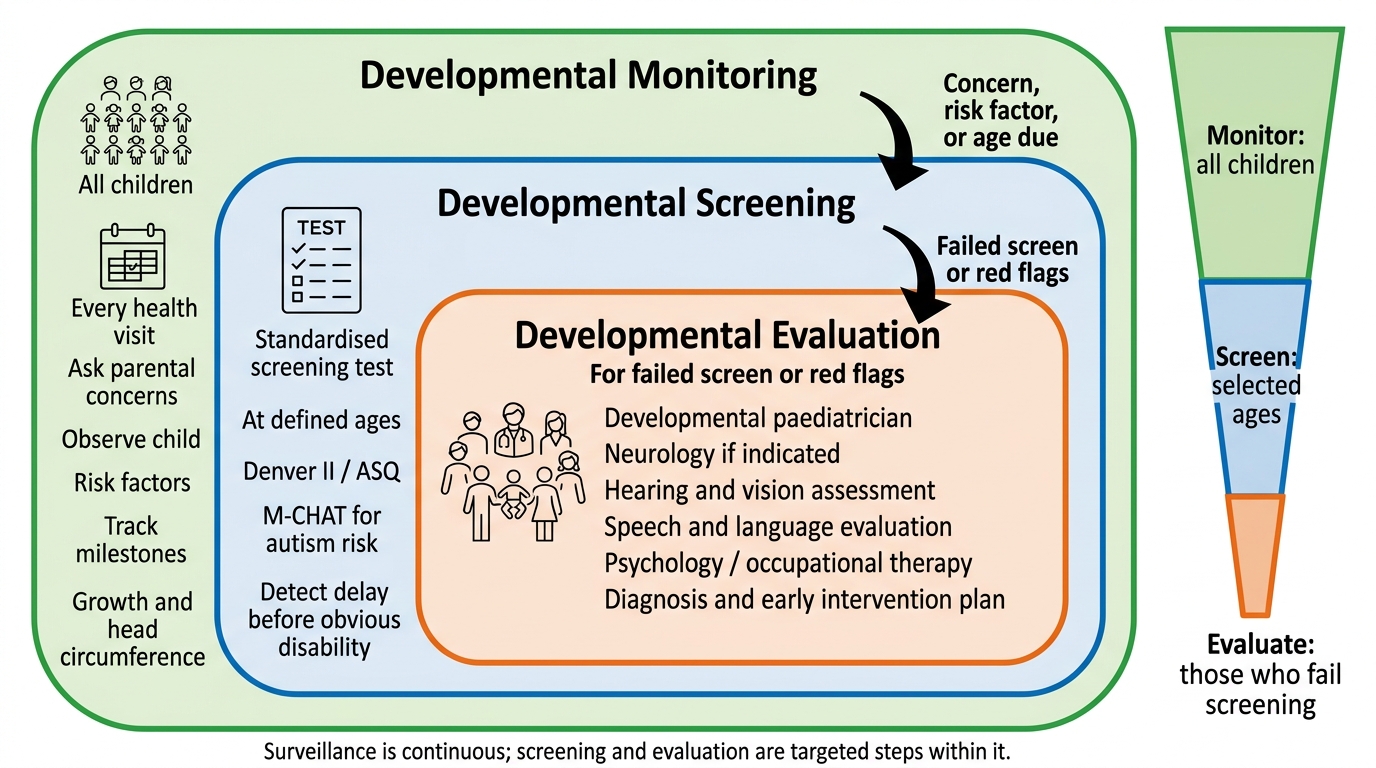
Three Levels of Developmental Surveillance
The Four Domains of Development: Normal Milestones from Birth to 5 Years
Development proceeds in four semi-independent but interacting domains. It is essential to learn milestones by domain and by age together—not as a memorised list but as a functional map that tells you what a child of a given age should be able to do with their body (gross motor), their hands and eyes (fine motor/adaptive), their voice and language comprehension (language), and their social world (personal-social). The ages given below are from Ghai's Essential Pediatrics and Nelson's Textbook, and reflect standard Indian/international paediatric teaching. Milestones represent median attainment ages—meaning approximately half of typically developing children will achieve a milestone before the stated age and half after. What matters clinically is not the exact age of attainment relative to the median, but whether the child falls within the expected range for that milestone and whether all four domains are progressing proportionally. A child consistently at the 25th percentile for every domain is developing normally; a child at the 50th percentile for gross motor but the 5th percentile for language is showing domain-specific asymmetry that warrants evaluation. The table below provides the high-yield milestones that form the core of clinical developmental assessment at each key age point.
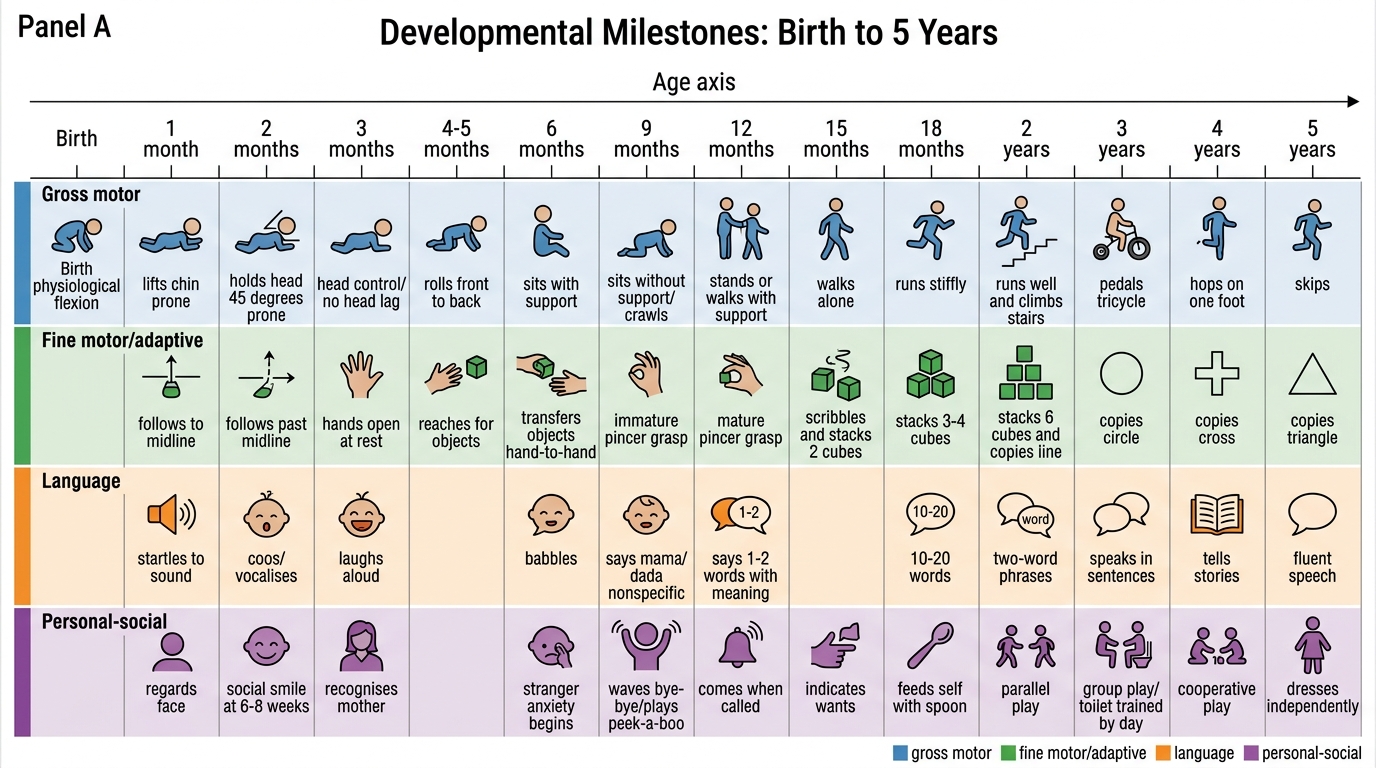
Developmental Milestones: Birth to 5 Years
| Age | Gross Motor | Fine Motor/Adaptive | Language | Personal-Social |
|---|---|---|---|---|
| 1 month | Lifts chin prone | Follows to midline | Startles to sound | Regards face |
| 2 months | Holds head to 45° prone | Follows past midline | Coos, vocalises | Social smile (6–8 weeks) |
| 3 months | Neck holding (head control, no head lag) | Hands open at rest | Laughs aloud | Recognises mother |
| 4–5 months | Rolls front to back | Reaches for objects | Squeals, turns to voice | Enjoys play |
| 6 months | Sits with support, transfers objects hand-to-hand | Palmar grasp, bangs objects | Babbles (da-da, ma-ma — non-specific) | Stranger anxiety begins |
| 9 months | Sits without support, stands with support | Pincer grasp (index-thumb) | Says mama/dada specifically | Waves bye-bye, plays peek-a-boo |
| 12 months | Walks with support; cruises | Releases cube in cup | First words (1–2 meaningful words) | Comes when called, imitates actions |
| 15 months | Walks alone (12–15 months) | Tower of 2 cubes | 4–6 words | Uses spoon, points to wants |
| 18 months | Runs, walks up stairs with help | Tower of 3–4 cubes | 10+ words; 2-word phrases (18–24 months) | Symbolic play begins |
| 24 months | Walks up/down stairs (two feet/step) | Tower of 6–7 cubes | 50+ words; 2-word sentences | Parallel play; uses 'mine' |
| 3 years | Rides tricycle, jumps on both feet | Tower of 9 cubes, copies circle | 3-word sentences, names colours | Group play, dresses with help |
| 5 years | Skips, hops on one foot | Copies triangle, ties shoelaces | Full sentences, asks meaning of words | Plays cooperative games, independent in toileting |
High-yield age-precise landmarks (PE known-traps):
- Social smile: 6–8 weeks (NOT 3 months — a common error)
- Neck control (no head lag): ~3 months
- Sits without support: 6–8 months
- Pincer grasp: ~9–10 months
- First meaningful words: ~12 months
- Walks alone: 12–15 months (NOT 18 months — 18 months is the upper limit of normal)
- 2-word phrases: 18–24 months
- 2-word sentences (mature): ~24 months
SELF-CHECK
A 10-month-old infant can sit without support, picks up a small raisin with index finger and thumb, says 'mama' specifically for his mother, and waves bye-bye. His development is:
A. Delayed in gross motor domain
B. Delayed in fine motor domain
C. Age-appropriate across all four domains
D. Delayed in language domain
Reveal Answer
Answer: C. Age-appropriate across all four domains
At 10 months, sitting without support (by 6–8 months), pincer grasp with index finger and thumb (by 9–10 months), first specific word 'mama' (by 12 months — ahead of schedule), and waving bye-bye (by 9 months) are all at or ahead of the expected range. All four domains are age-appropriate.
Mechanisms Underlying Development: Neural Maturation and Environmental Inputs
The developmental milestone sequence is not arbitrary—it is the observable expression of predictable neurological maturation. Two anatomical directions govern the sequence: cephalocaudal maturation (from the head downward) explains why head control precedes trunk control, which precedes standing and walking; proximodistal maturation (from the body axis outward to the extremities) explains why shoulder control (reaching) precedes wrist control (transferring), which precedes finger control (pincer grasp). These sequences are constants—a child cannot skip them, and cannot reliably acquire distal control before proximal control is established.
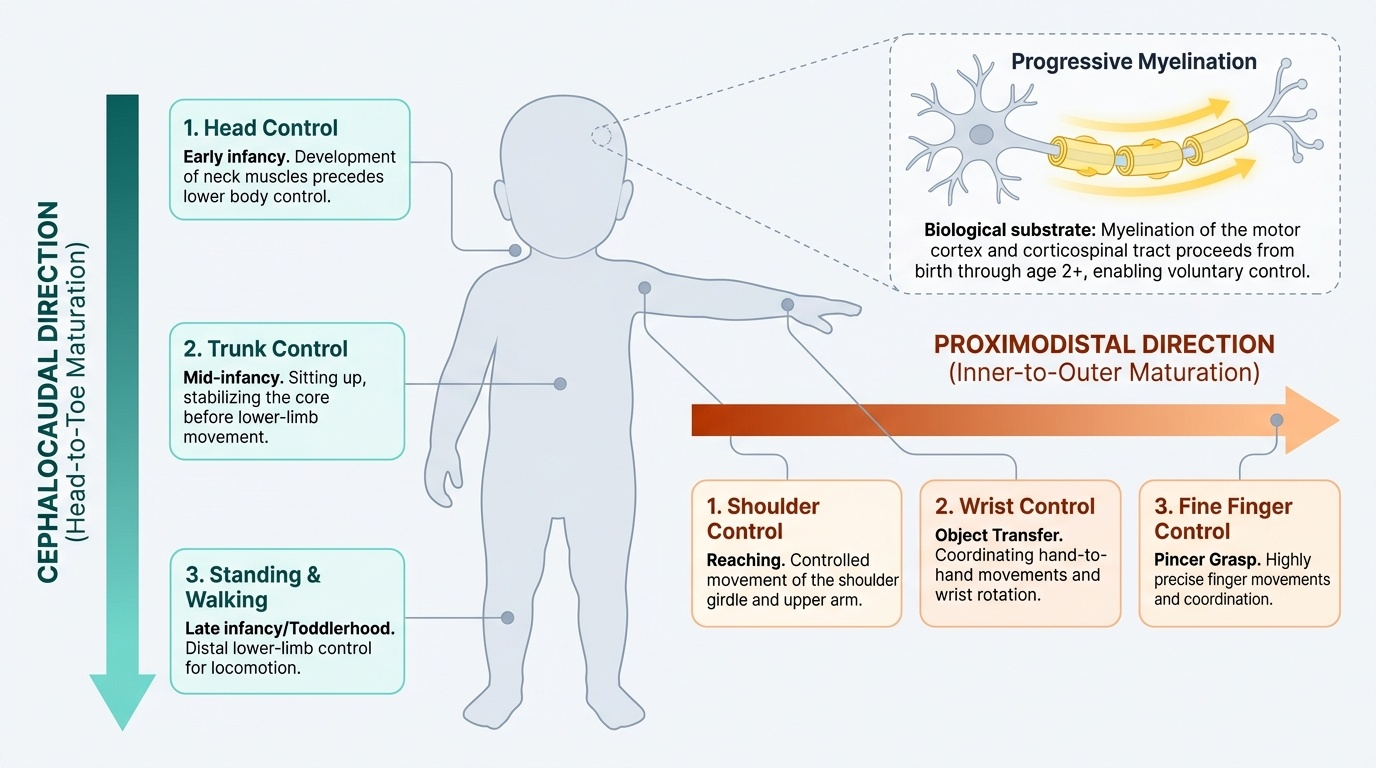
Provided image
At the cellular level, the maturation sequence corresponds to progressive myelination of neural pathways. Myelination of motor cortex fibres and the corticospinal tract proceeds from birth through the first 2 years and beyond, and is the biological substrate for the increasing precision and voluntary control visible in the milestone sequence. Premature infants have delayed myelination and therefore developmental delay proportional to the degree of prematurity; corrected age (chronological age minus weeks of prematurity) should be used for developmental assessment in infants born before 37 weeks, up to age 2 years.
Critical and sensitive periods are windows of heightened neuroplasticity during which specific developmental processes are maximally responsive to input. Language has a critical period extending through approximately age 7; early visual experience is critical for binocular vision and stereopsis in the first 6 months; early social-emotional stimulation shapes the stress-regulation systems of the developing brain (the basis of adverse childhood experiences research). Disruption of appropriate input during these windows—through sensory deprivation, emotional neglect, or neurological injury—produces deficits that become progressively harder to remediate as plasticity declines.