Page 9 of 15
PE1.3 | Developmental Milestones and Assessment — SDL Guide (Part 2)
Factors Affecting Development: Biological and Environmental Determinants
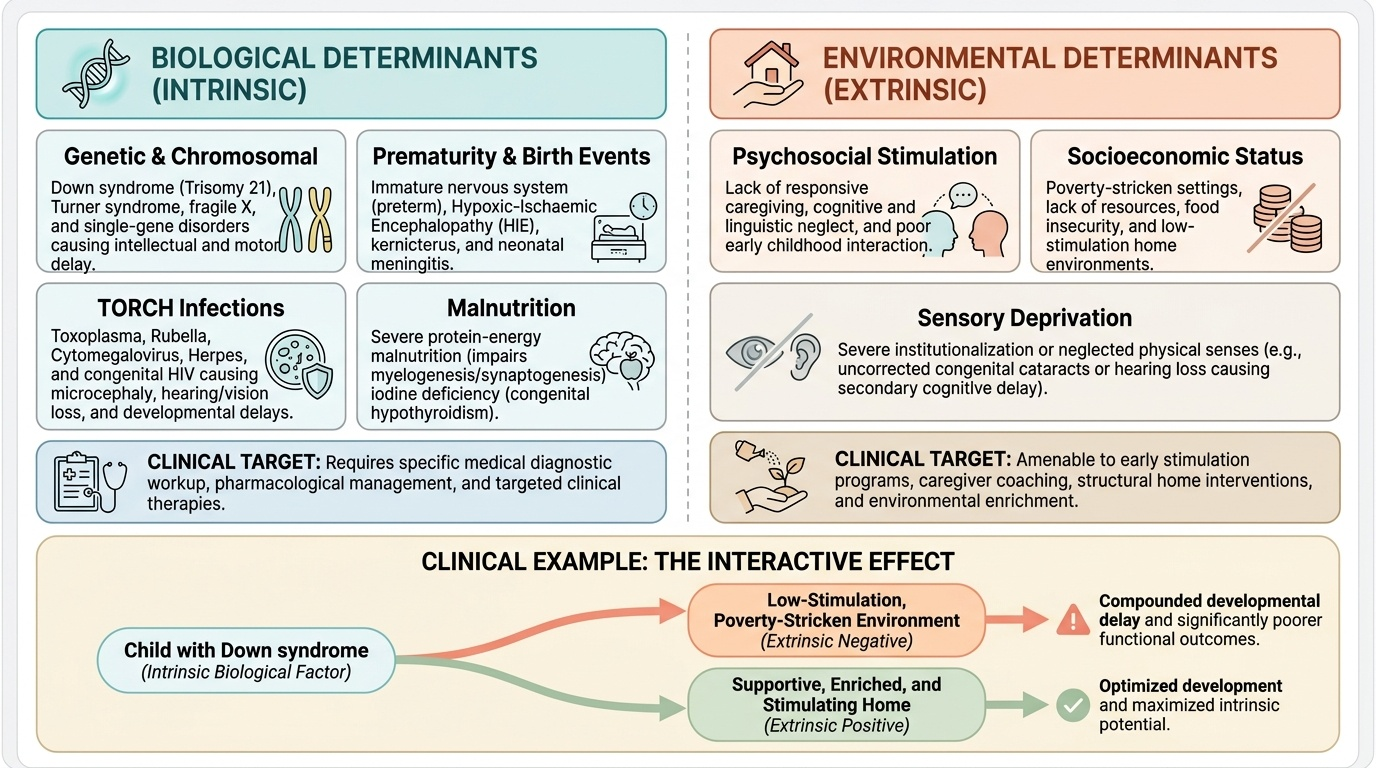
Development, like growth, is the result of an interaction between the child's genetic and biological endowment and the environment in which development takes place. Both categories of factors can delay, accelerate, or distort development, and the clinical approach to a child with suspected delay requires systematic consideration of both. The distinction between biological and environmental determinants is clinically important because it shapes both the aetiological workup and the therapeutic targets: biological causes often require specific diagnosis and medical management, while environmental deficits are amenable to stimulation and caregiver interventions. In many children, both categories operate simultaneously—a child with Down syndrome (biological) who also grows up in a poverty-stricken, low-stimulation environment (environmental) will have worse developmental outcomes than the same child in a supportive, enriched home. Understanding which factors are modifiable is the key to identifying where intervention can make a difference within a given child's circumstances.
Provided image
Biological (intrinsic) factors include:
- Genetic and chromosomal conditions: Down syndrome (trisomy 21) causes intellectual disability and motor delay; Turner syndrome, fragile X syndrome, and single-gene disorders each have characteristic developmental profiles.
- Prematurity: preterm infants have immature nervous systems; developmental assessment uses corrected age (subtract weeks of prematurity from chronological age) up to 2 years.
- Perinatal events: hypoxic-ischaemic encephalopathy (HIE) following birth asphyxia is a leading cause of cerebral palsy and intellectual disability; neonatal hypoglycaemia, hyperbilirubinaemia (kernicterus causing athetoid cerebral palsy), and neonatal meningitis all have neurological sequelae.
- Congenital infections (TORCH): Toxoplasma, Rubella, Cytomegalovirus, Herpes cause microcephaly, intellectual disability, hearing and vision loss; congenital HIV affects neurodevelopment.
- Malnutrition: severe protein-energy malnutrition, especially before 2 years, directly impairs brain myelination and synaptogenesis. Iodine deficiency causes hypothyroidism, with irreversible intellectual disability if untreated.
Environmental (extrinsic) factors include:
- Psychosocial stimulation: responsive caregiving, language-rich environments, play, and emotional security are the most powerful environmental drivers of cognitive and language development. The absence of stimulation in early childhood—due to neglect, poverty, or parental mental illness—has lasting effects on brain structure and function.
- Socioeconomic deprivation: poverty creates compound risk through poor nutrition, inadequate stimulation, higher infection burden, and reduced access to healthcare and early intervention services.
- Sensory deprivation: undetected hearing loss is the most common preventable cause of language delay; undetected visual impairment delays fine motor and adaptive development.
- Chronic illness: any condition causing recurrent hospitalisation, pain, or fatigue reduces the time and energy available for developmental exploration and practice.
SELF-CHECK
A 12-month-old infant born at 28 weeks gestation (corrected age 5 months) does not yet hold his head steadily. The most appropriate interpretation is:
A. Global developmental delay requiring urgent neurological referral
B. Age-appropriate development when corrected age is used
C. Gross motor delay in isolation
D. Evidence of cerebral palsy
Reveal Answer
Answer: B. Age-appropriate development when corrected age is used
Head control is typically achieved at ~3 months. This infant's corrected age is 12 − 3.5 (months of prematurity) = approximately 5 months corrected. At 5 months corrected age, head control without head lag would be expected to be emerging but inconsistent head stability is still within range. For preterm infants, corrected age (not chronological age) must be used for developmental assessment up to 24 months. Without applying corrected age, this child would appear severely delayed when development is actually tracking appropriately.
CLINICAL PEARL
Developmental regression—loss of previously acquired milestones—is always pathological and requires urgent evaluation. Unlike developmental delay (in which a child is slow to acquire skills but continues to progress), regression indicates active neurological deterioration. Causes include neurodegenerative disorders (metachromatic leukodystrophy, Rett syndrome in girls, neuronal ceroid lipofuscinosis), metabolic disorders with neurological involvement, epileptic encephalopathy (West syndrome with infantile spasms causing loss of social responsiveness), and psychosocial trauma (causing temporary regression in language or toilet training). A parent reporting that a child 'used to say 10 words and now says nothing' is describing regression, not delay—and this distinction mandates immediate specialist referral. Do not reassure and review: investigate.
Methods of Developmental Assessment
Developmental assessment in clinical practice combines three complementary approaches: a structured developmental history, direct clinical observation, and when indicated, standardised screening or diagnostic tools. No single approach is sufficient alone; a complete assessment uses all three in sequence. The developmental history provides the longitudinal dimension—what a child could do at earlier time points and whether there has been any regression. Clinical observation provides the cross-sectional snapshot—what the child can do right now, in front of you, with appropriate elicitation. Standardised tools provide a normative comparison—whether the child's demonstrated skills fall within the expected range for the reference population, and whether the pattern of delay across domains is consistent with a specific diagnostic category. Together, these three approaches give the clinician both the breadth (all four domains assessed) and the depth (historical trajectory, current status, normative benchmarking) needed to make a well-founded clinical judgment. The choice of which standardised tool to use depends on the child's age, the clinical setting, and the tool's normative population—which is why knowing the Indian-validated tools separately from the international ones matters in practice.
Provided image
Developmental history is the foundation of assessment. It should cover:
- Age of attainment of specific milestones in each domain (ask about gross motor, fine motor, language, and social skills systematically by age).
- Developmental regression: has the child lost any previously acquired skills?
- Perinatal history: gestational age, birth asphyxia, NICU admission, neonatal jaundice, seizures.
- Family history: developmental delay, intellectual disability, hearing/vision loss, consanguinity.
- Social history: language spoken at home, quality of caregiving, access to stimulation.
Clinical observation of the child during the consultation provides real-time developmental information: Does the child make eye contact? Do they respond to their name? Can they follow simple commands? Can they manipulate objects brought to them? A structured elicitation of several key milestones appropriate for the child's age can be performed in 5–10 minutes of directed observation.
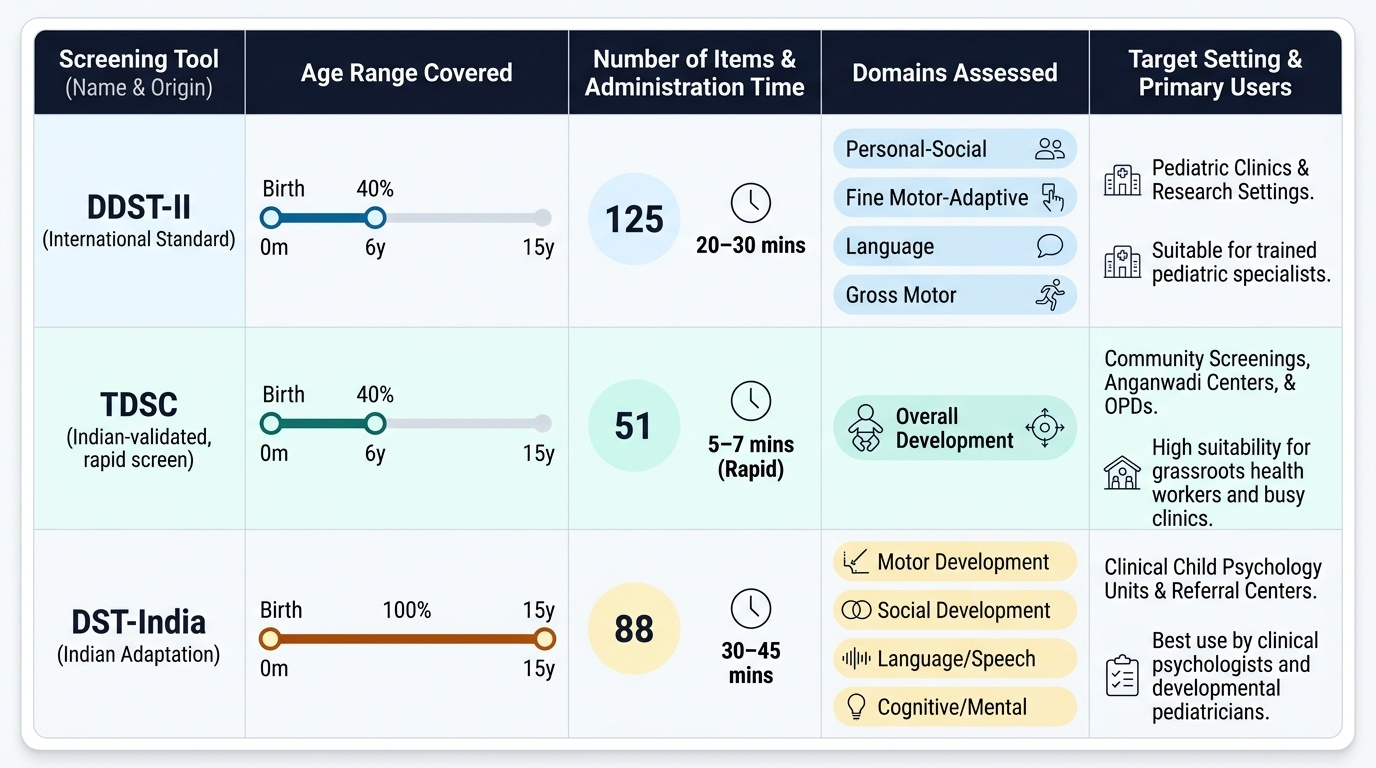
Standardised developmental screening tools used in India:
- Denver Developmental Screening Test II (DDST-II): widely used globally; assesses gross motor, fine motor/adaptive, language, and personal-social domains from birth to 6 years; uses items drawn from a US-normative population. An adapted Indian version is available. The DDST-II uses a visual timeline format: items are represented as bars spanning the age range over which 25–90% of children pass them.
- Trivandrum Developmental Screening Chart (TDSC): developed and validated on South Indian children aged 0–2 years; 17 items selected from the Bayley Scale of Infant Development; designed for use by community health workers with minimal training. Advantages: Indian normative data, brevity, community usability.
- Developmental Screening Test (DST) — Bharat Kapila: Indian standardised tool covering birth to 15 years; provides developmental quotient (DQ) calculation; widely used in Indian developmental paediatric practice.
Clinical Application: Identifying Developmental Delay and Initiating Action
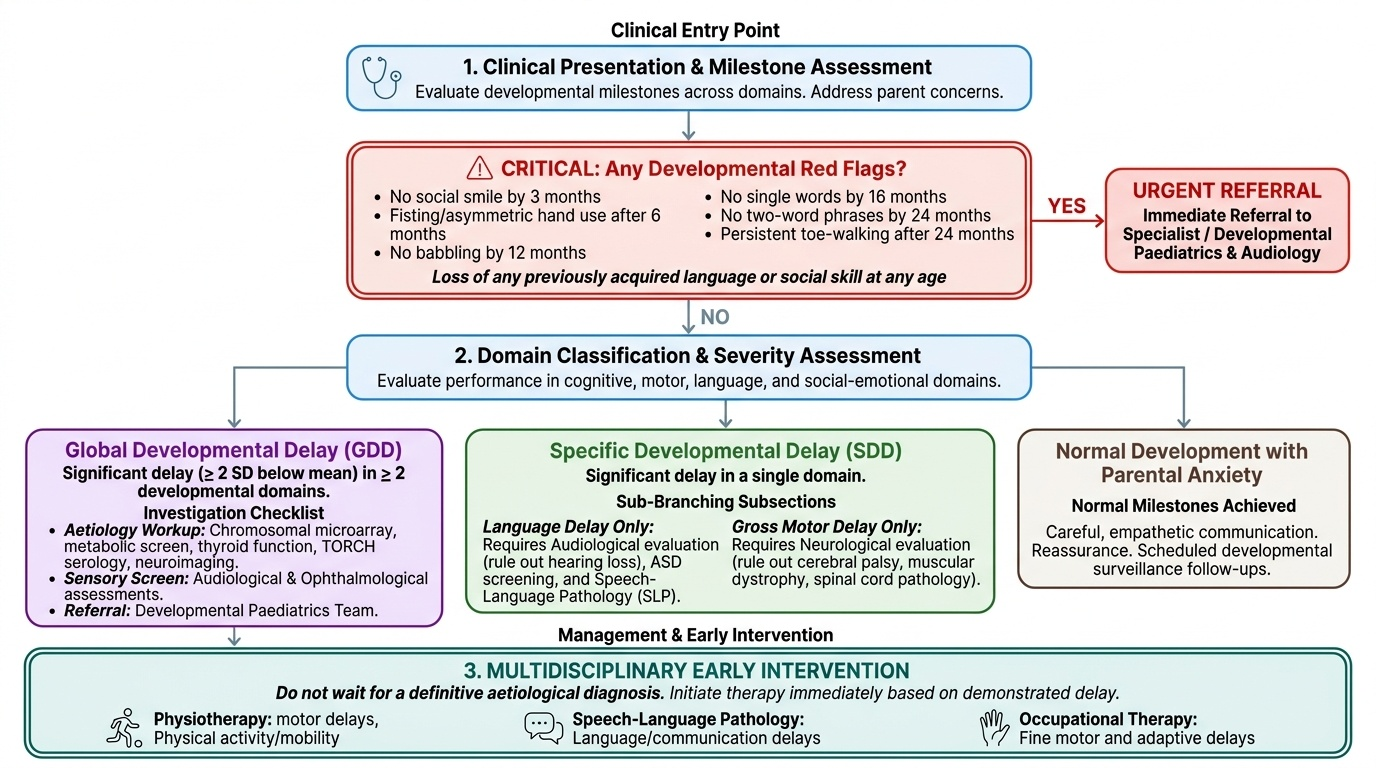
Clinical application of developmental knowledge requires translating milestone knowledge into a classification of a child's developmental status and then into a management decision. The key classifications are global developmental delay, specific developmental delay, developmental regression, and normal development with parental anxiety (which is itself an important clinical encounter requiring careful communication).
Provided image
Global developmental delay (GDD) is defined as significant delay (>2 SD below the mean, or failure to achieve expected milestones) in two or more developmental domains. It is the under-5 equivalent of intellectual disability (a term used when developmental delay persists and is assessable after age 5). GDD requires comprehensive evaluation: aetiology workup (chromosomal microarray, metabolic screen, thyroid function, TORCH serology, neuroimaging), audiological assessment, ophthalmological assessment, and referral to a developmental paediatrics team.
Specific developmental delay involves delay in a single domain—most commonly language. Isolated language delay in an otherwise normally developing child requires audiological evaluation (hearing loss is the most common remediable cause), but may also reflect autism spectrum disorder (where social communication is disproportionately affected) or speech-motor disorders (articulation, dysfluency). Isolated gross motor delay requires neurological evaluation for cerebral palsy, muscular dystrophy, or spinal cord pathology.
Red flags that mandate immediate referral regardless of how the parent frames the concern:
- No social smile by 3 months
- No babbling by 12 months
- No single words by 16 months
- No two-word phrases by 24 months
- Loss of any previously acquired language or social skill at any age
- Persistent toe-walking after 24 months
- Fisting or asymmetric hand use after 6 months (asymmetric motor development suggesting hemiplegia)
Early intervention principles: the earlier intervention begins, the greater the neuroplasticity benefit. Even without a definitive aetiological diagnosis, a child with demonstrated developmental delay should be referred to early intervention services (physiotherapy for motor delay, speech-language pathology for language delay, occupational therapy for fine motor and adaptive delay) concurrently with the diagnostic workup—not after.
SELF-CHECK
An 18-month-old child has no meaningful words, does not point to objects, does not make eye contact consistently, and does not respond to his name. The most important initial investigation is:
A. MRI brain
B. Chromosomal karyotype
C. Formal audiological assessment (hearing test)
D. Thyroid function tests
Reveal Answer
Answer: C. Formal audiological assessment (hearing test)
The clinical picture—absent language, lack of pointing, poor eye contact, not responding to name—raises concern for autism spectrum disorder or hearing impairment. Formal audiological assessment is the single most important initial investigation because hearing loss is the most common, most easily treatable cause of language delay, and must be excluded before any other diagnosis is pursued or before referring for autism assessment. MRI, karyotype, and thyroid tests are indicated based on specific clinical findings (e.g. dysmorphic features, regression, growth abnormality) but are not the first priority when hearing has not been excluded.
Self-Assessment: Developmental Milestones and Assessment
Work through these scenarios to test your milestone knowledge before your next paediatrics posting.
Scenario 1: A mother brings her 9-month-old daughter. She says the baby does not wave bye-bye and does not look when her name is called. She does, however, sit without support and picks up objects with a raking grasp. Which domains are concerning, and what is the most important single question you would ask?
(Language and personal-social domains are concerning: waving bye-bye and name responsiveness are expected by 9 months. The most important question: does the baby turn when her name is called from out of sight (i.e. when visual cues are absent)? This specifically tests auditory responsiveness and distinguishes hearing impairment from social inattention. Refer for audiological assessment.)
Scenario 2: How old is a child who: walks alone without support, uses 3 meaningful words, uses a spoon messily, and builds a tower of 2 cubes?
(This profile corresponds to approximately 15 months: walking alone is expected by 12–15 months; 3 words by 15 months; spoon use and 2-cube tower by 15 months. Social smile at 6–8 weeks and neck control at 3 months are long passed.)
Scenario 3: A 24-month-old boy is brought because 'he doesn't talk.' The mother says he had 8–10 words at 18 months but now seems to have fewer words and has become socially withdrawn. How does this change your assessment compared to a child who simply never had many words?
(The history describes developmental regression—loss of previously acquired language and social skills. This is always pathological and cannot be explained as 'late development.' Key differentials include autism spectrum disorder (where a regression plateau is common around 18–24 months), epileptic encephalopathy (e.g. Landau-Kleffner syndrome causing acquired epileptic aphasia), and metabolic/neurodegenerative conditions. This child needs urgent referral, not watchful waiting.)