Page 19 of 26
PE18.{8,10-12} | Safe Vaccine Administration Workflow — SDL Guide (Part 2)
Step-by-Step Vaccine Administration Technique
The procedural sequence for vaccine administration is not merely a checklist — each step has a physiological or safety rationale that, when understood, makes correct execution more reliable than rote memory. A practitioner who knows WHY each step is performed can adapt correctly when unexpected situations arise, such as a struggling child, a partially used vial, or missing equipment. Vaccine administration can be divided into three sequential phases: pre-injection preparation, the injection itself, and post-injection management. Each phase carries its own risk points, and errors in any one phase can compromise the safety of the entire encounter. The pre-injection phase accounts for the majority of programme-error AEFIs — vial mix-ups, cold-chain breaks, and equipment failures all occur before the needle touches the skin. Mastering this sequence as a cognitive habit, not just a physical skill, is what separates a safe immunizer from an unsafe one.
Pre-injection preparation:
1. Hand hygiene — wash hands with soap and water, or use alcohol-based hand rub; dry thoroughly before touching any equipment.
2. Assemble equipment — auto-disable (AD) syringe of the correct volume, needle of the correct gauge and length, the vaccine vial, and a hub-cutter or puncture-proof sharps container within reach.
3. Check the vial — read the label (name, dose, expiry, batch number); inspect the VVM; check for turbidity, particulates, or colour change in vaccines that should be clear; ensure the reconstituted vaccine was prepared within the permitted time window.
4. Draw up the dose — pierce the rubber septum with a clean needle; invert the vial; withdraw the correct volume without introducing air bubbles; tap and express any air bubble upward.
5. Patient positioning — place the infant supine on the table or in the caregiver's lap. Ensure the limb is fully exposed and relaxed. For older children, seat them on the caregiver's lap with the arm hanging free.
Injection technique (IM, anterolateral thigh, as the most common example):
6. Identify the site — palpate the lateral aspect of the middle third of the thigh. Stretch the skin gently between two fingers (Z-track is not required for routine IM vaccines in children but bunching in infants may aid needle placement).
7. Insert the needle — at 90° to the skin surface, with a quick, confident motion to the hub (for a 16 mm needle in an infant, full insertion reaches the muscle). Slow insertion causes more pain.
8. Do NOT aspirate — IAP/WHO advise that aspiration is unnecessary and should be omitted at recommended anatomical sites.
9. Inject the vaccine — push the plunger steadily over 1–2 seconds. Do not inject rapidly.
10. Withdraw the needle — withdraw smoothly at the same angle as insertion. Apply gentle pressure with a dry cotton ball; do NOT rub (rubbing increases local reactogenicity by dispersing vaccine through tissue planes).
11. Do NOT recap the needle — recapping is the leading cause of needle-stick injuries in immunization workers. Place the used syringe directly into the hub-cutter or puncture-proof container IMMEDIATELY after withdrawal.
For BCG (ID technique):
Insert the 26 G needle, bevel up, nearly parallel to the skin surface (15°), with only 2–3 mm of the needle tip in the dermis. Inject slowly — resistance should be felt, and a tense pale bleb of 5–7 mm should appear. If no bleb forms, the needle tip was subcutaneous; the dose is likely lost and should not be repeated at the same site (consult supervisor). After withdrawal, do not rub.
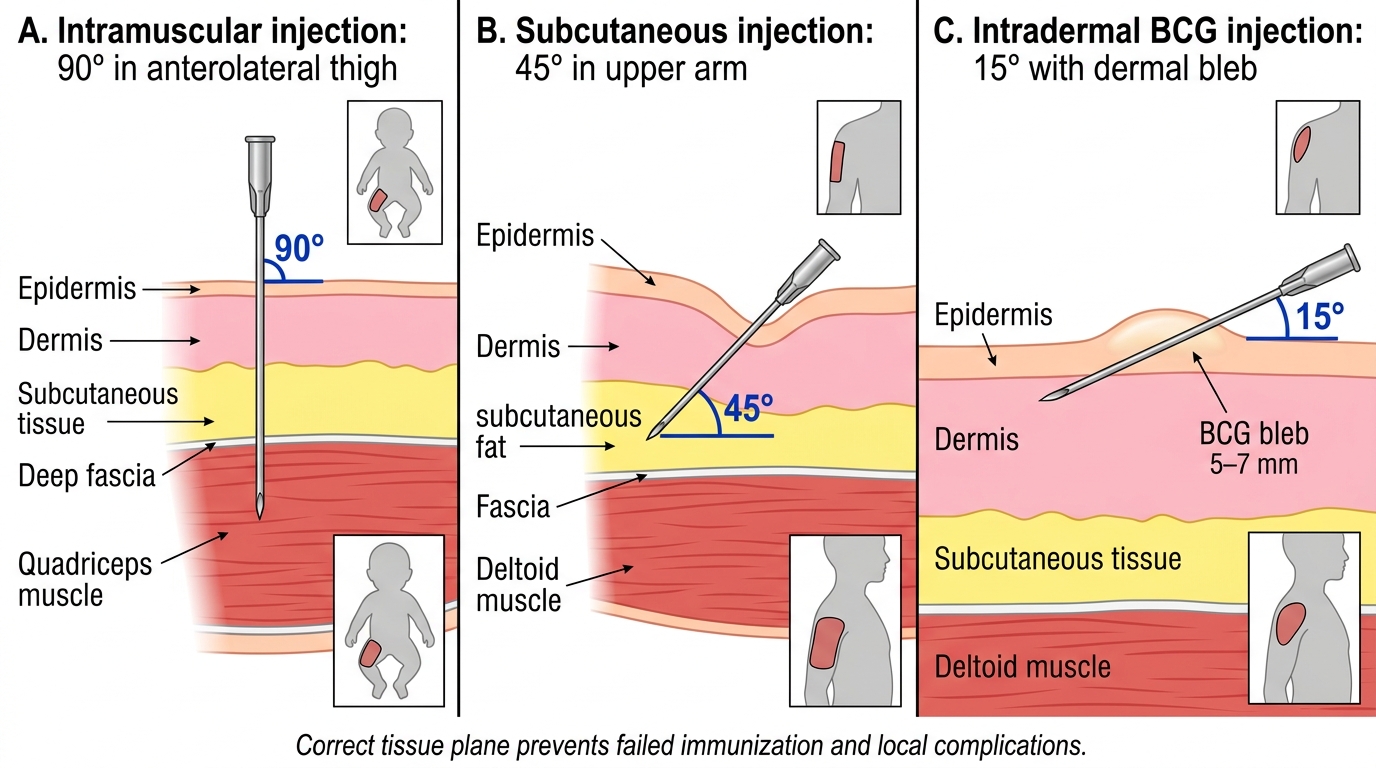
Correct Needle Angles and Tissue Planes for Immunization
Post-injection care:
Keep the child and caregiver at the immunization site for 30 minutes for observation (minimum 15 minutes per some field guidelines, but 30 minutes is the standard for detecting early anaphylaxis). Instruct caregivers on expected minor reactions (low-grade fever, redness, mild swelling at site within 24–48 hours) and when to seek immediate care (high fever, persistent crying >3 hours, collapse, difficulty breathing within the monitoring period or within 24–48 hours).
Patient/caregiver counselling: Before leaving, provide verbal and where available written guidance on:
- Expected normal reactions and their timeline
- Fever management (paracetamol syrup — weight-based, 10–15 mg/kg per dose, 4–6 hourly PRN; NOT aspirin or ibuprofen in infants < 3 months)
- The date and vaccine due at the next visit
- When to return urgently
CLINICAL PEARL
The BCG bleb is your injection quality-control marker. A correct intradermal BCG injection produces a pale, tense bleb of 5–7 mm diameter that disappears within 30 minutes as the fluid disperses through the dermal lymphatics. No bleb = the injection landed subcutaneously, meaning the dose is in the wrong tissue plane and immune priming will be suboptimal. The scar at 4–6 weeks (a small ulcer that heals to a round scar ≤10 mm) is the downstream quality marker of correct technique. Conversely, a large ulcerated or keloidal BCG scar suggests either too deep an injection or hypersensitivity — important to note in the record.
AEFI: Recognition, Classification, and Reporting
An adverse event following immunization (AEFI) is any untoward medical occurrence that follows immunization and does not necessarily have a causal relationship with the vaccine. This broad definition is intentional — it triggers investigation without prejudging causation. The WHO (2012) classification organises AEFIs into four aetiological categories based on investigation findings, which guides both management and programme response. Understanding the classification is not merely an academic exercise: it determines whether an event is reported as a signal of programme failure (error-related), as an expected biological reaction (vaccine-induced), or as a coincidence requiring no programme action. Misclassifying a programme error as a vaccine-induced reaction protects a faulty workflow from scrutiny and allows the error to recur; misclassifying a coincidental event as vaccine-induced erodes public confidence unnecessarily. For the clinician managing the child, the classification also informs the urgency of the reporting pathway and whether a cluster investigation should be triggered. The four categories are mutually exclusive after investigation, though the initial clinical presentation may be ambiguous — the classification is assigned after a structured AEFI investigation, not at the bedside.
Provided image
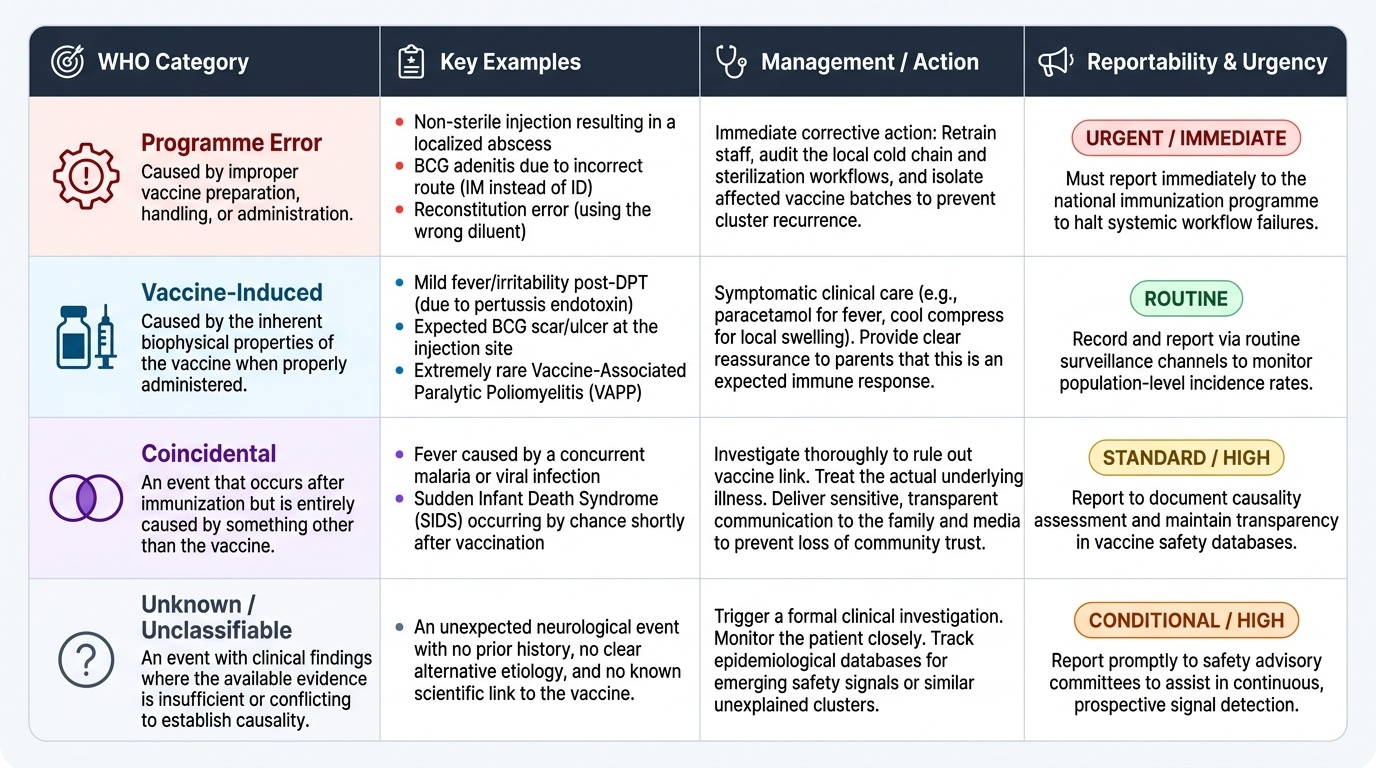
WHO 4-category AEFI classification:
1. Vaccine-induced reaction (vaccine product–related): caused by the inherent properties of the vaccine when properly given. Examples: mild fever post-DPT (endotoxin from pertussis component), BCG ulcer, oral poliovirus vaccine-associated paralytic poliomyelitis (VAPP — rare). These are expected, immunologically mediated, and their frequency is known from pre-licensure trials.
2. Immunization error–related reaction (programme error): caused by a vaccine that has been improperly prepared, handled, or administered — NOT an intrinsic property of the vaccine. Examples: abscess from non-sterile injection technique, BCG adenitis from IM instead of ID injection, transmission of blood-borne pathogens from needle reuse, anaphylaxis from over-concentrated reconstituted vaccine. These are PREVENTABLE and indicate a failure in the safe-administration workflow.
3. Immunization anxiety–related reaction: caused by anxiety about the injection rather than by the vaccine itself. Examples: vasovagal syncope (especially in adolescents), hyperventilation, psychogenic pain. Managed with calm reassurance; patient must be kept supine and observed.
4. Coincidental event: temporal association only; would have occurred regardless of vaccination (e.g. fever from an upper respiratory infection that began the day of vaccination). Investigation reveals no evidence of any of the first three categories.
Clinical recognition of major AEFI:
Minor local reactions (days 1–3): redness (erythema), swelling, tenderness at injection site — expected, self-limiting, require only reassurance and paracetamol if the child is distressed.
Minor systemic reactions (hours to days 1–2): low-grade fever (≤38.5°C), irritability, malaise — common post-DPT/pentavalent, expected, managed at home.
Serious AEFI (require urgent assessment):
- Anaphylaxis: onset usually within 15–30 minutes; urticaria, angioedema, bronchospasm, hypotension, collapse. Treatment: adrenaline 0.01 mL/kg of 1:1000 solution IM into the lateral thigh (maximum single dose 0.5 mL in children); call for emergency help; oxygen; IV access.
- High-pitched/inconsolable crying >3 hours (screaming episode): associated with pertussis-containing vaccines; generally self-limiting but must be reported.
- Hypotonic-hyporesponsive episode (HHE): pallor, limpness, unresponsiveness within 48 hours of pertussis-containing vaccine; mechanism uncertain; generally self-limiting, no sequel, but extremely alarming and must be reported.
- Febrile seizure: temperature-related, generally benign in a neurologically normal child, but must be assessed and reported.
- Encephalopathy/encephalitis: very rare; onset within 72 hours; requires urgent investigation and reporting.
AEFI reporting workflow (India):
All serious AEFI must be reported within 24 hours through the district AEFI committee → state AEFI committee → national PvPI (Pharmacovigilance Programme of India) and IPC-AEFI systems. The reporting form (AEFI Case Investigation Form) captures: child's demographics, vaccine details (name/batch/manufacturer/expiry/site), cold-chain details, clinical description, and outcome. Minor expected reactions need not be formally reported but should be recorded in the facility register.
Medicolegal implications:
An AEFI may lead to a medicolegal complaint if the caregiver believes it was caused by negligence. The practitioner's protection is (a) documented correct administration technique, (b) documented pre-vaccination counselling (informed consent), (c) timely and complete AEFI reporting, and (d) evidence that the vaccine was from an unbroken cold chain. Indian courts have addressed vaccine injury liability under the Consumer Protection Act 2019 (medical negligence) — the key test is deviation from standard of care.
SELF-CHECK
A 6-week-old infant develops a 3 cm fluctuant abscess at the site of pentavalent vaccine given 10 days ago. Injection records show the vaccine was reconstituted 6 hours before use and the same needle was used to draw up doses for two children. How should this AEFI be classified?
A. Vaccine-induced (vaccine product–related) reaction — local abscess is a known complication of pentavalent vaccine
B. Immunization error–related reaction — the abscess was caused by programmatic failure (prolonged reconstitution and possible needle reuse), not vaccine properties
C. Coincidental event — the infant probably had a pre-existing skin infection
D. Immunization anxiety–related reaction — needle-site reactions are triggered by stress
Reveal Answer
Answer: B. Immunization error–related reaction — the abscess was caused by programmatic failure (prolonged reconstitution and possible needle reuse), not vaccine properties
Pentavalent vaccine is NOT a reconstituted vaccine (it is a liquid formulation) — but even if reconstituted vaccines were involved, using a dose 6 hours after preparation violates the 4-hour rule. More critically, reusing a needle between patients introduces contamination and cross-infection risk, violating basic safe-injection practice. This is an IMMUNIZATION ERROR–RELATED AEFI. The WHO AEFI classification assigns this to 'programme error' — preventable failures in preparation, handling, or administration technique.
Documentation: The Immunization Record
Accurate immunization documentation is the bridge between a single vaccine administration and the child's lifelong immune history, the epidemiological surveillance of vaccine coverage, and the medicolegal record of standard-of-care delivery. Incomplete or inaccurate records are a direct patient-safety hazard: a child with a falsely recorded dose may be treated as immune when they are not (under-vaccination risk) or given an additional unnecessary dose (over-vaccination with risk of local reactions and wasted resources).
Provided image
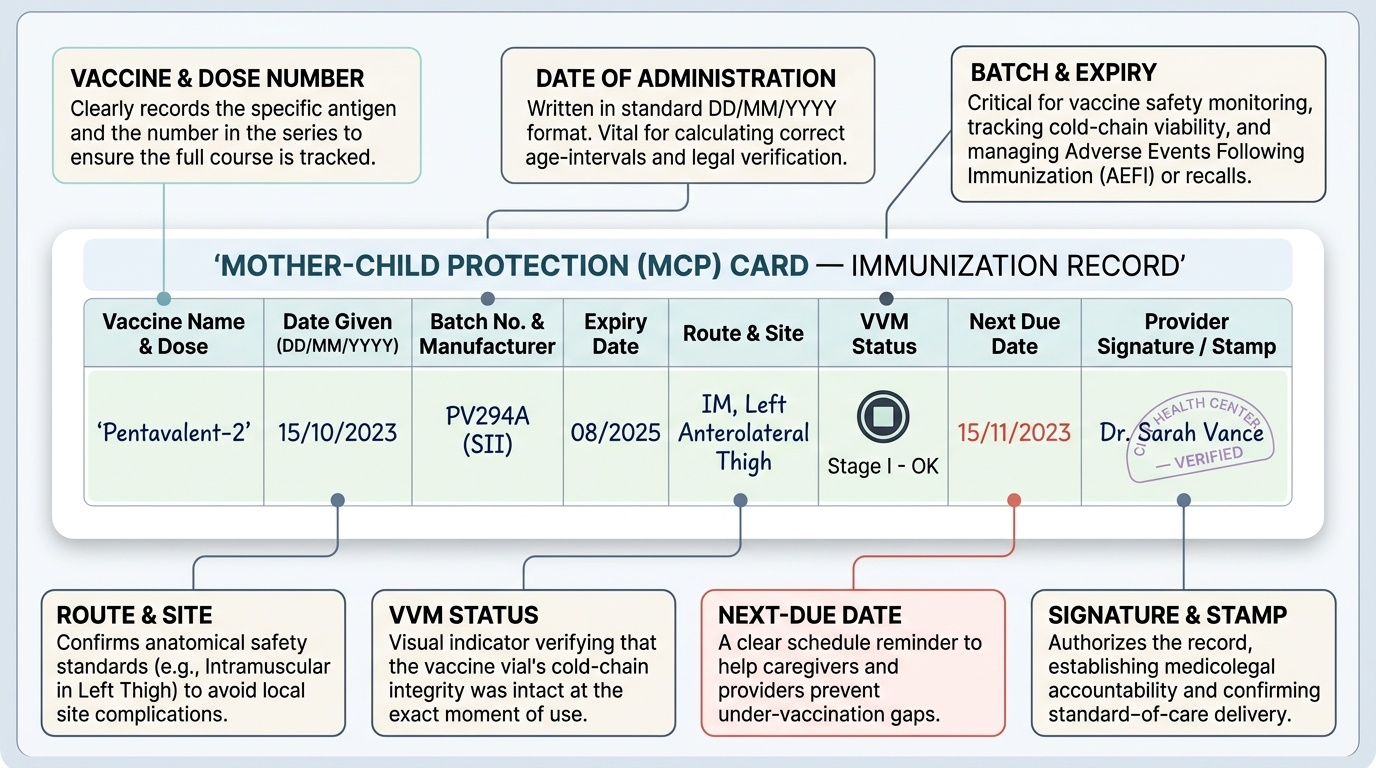
What must be recorded for each dose:
Every dose administered should be documented in TWO places: (a) the Mother-Child Protection (MCP) Card / immunization card (the child's portable record, kept with the caregiver) and (b) the facility immunization register (the provider's copy, used for coverage monitoring and AEFI investigation).
For each entry, record:
- Date of administration (DD/MM/YYYY — the medicolegal and epidemiological standard)
- Vaccine name (full name, e.g. 'Pentavalent-2', 'BCG', 'MR-1')
- Dose number in the series (e.g. 'DPT Booster 1')
- Batch number and manufacturer — essential for AEFI investigation and vaccine lot recall
- Expiry date of the vial
- Route and site of administration
- VVM status at time of use
- Name and signature/stamp of the administering health worker
- Date due for next vaccine — written clearly on the MCP card and verbally communicated to the caregiver
- Any adverse reaction observed during the 30-minute observation period
Interpreting a partially vaccinated child's record:
When a child presents with an incomplete or damaged MCP card, the practitioner must:
1. Determine the minimum age at which the child could have received each dose (cross-check with the NIS age windows).
2. Apply the principle: unknown vaccination status = unvaccinated — do not assume doses were given without documentation.
3. Restart the series from the appropriate point, respecting minimum intervals (≥4 weeks between primary-series injectable doses).
4. Catch-up vaccines are guided by the IAP catch-up schedule — a child who missed the 9-month MR dose can receive it at any subsequent contact.
Electronic immunization tracking:
Many states now use eVIN (Electronic Vaccine Intelligence Network) for cold-chain monitoring and U-WIN for individual immunization records. The paper MCP card remains the ground-truth document in field settings, and U-WIN entries supplement (not replace) it.
Medicolegal significance:
The immunization record is a medical document. Falsification (recording a dose that was not given) constitutes medical fraud and is actionable under the NMC Act 2020 (professional misconduct) and potentially under the Indian Penal Code if harm results. Practitioners must resist caregiver pressure to backdate or fabricate entries.