Page 20 of 26
PE18.{8,10-12} | Safe Vaccine Administration Workflow — SDL Guide (Part 3)
Biomedical Waste and Sharps Management
Every immunization session generates biomedical waste — used syringes, needles, empty vials, reconstitution diluent containers, cotton swabs, and gloves. Improper disposal is not merely an environmental concern; it is a direct cause of needle-stick injuries, pathogen transmission, and environmental contamination. The Biomedical Waste Management Rules (BMW Rules 2016, amended 2019) under the Environment Protection Act govern disposal at all healthcare facilities in India, including immunization sessions held at subcentres and outreach sites.
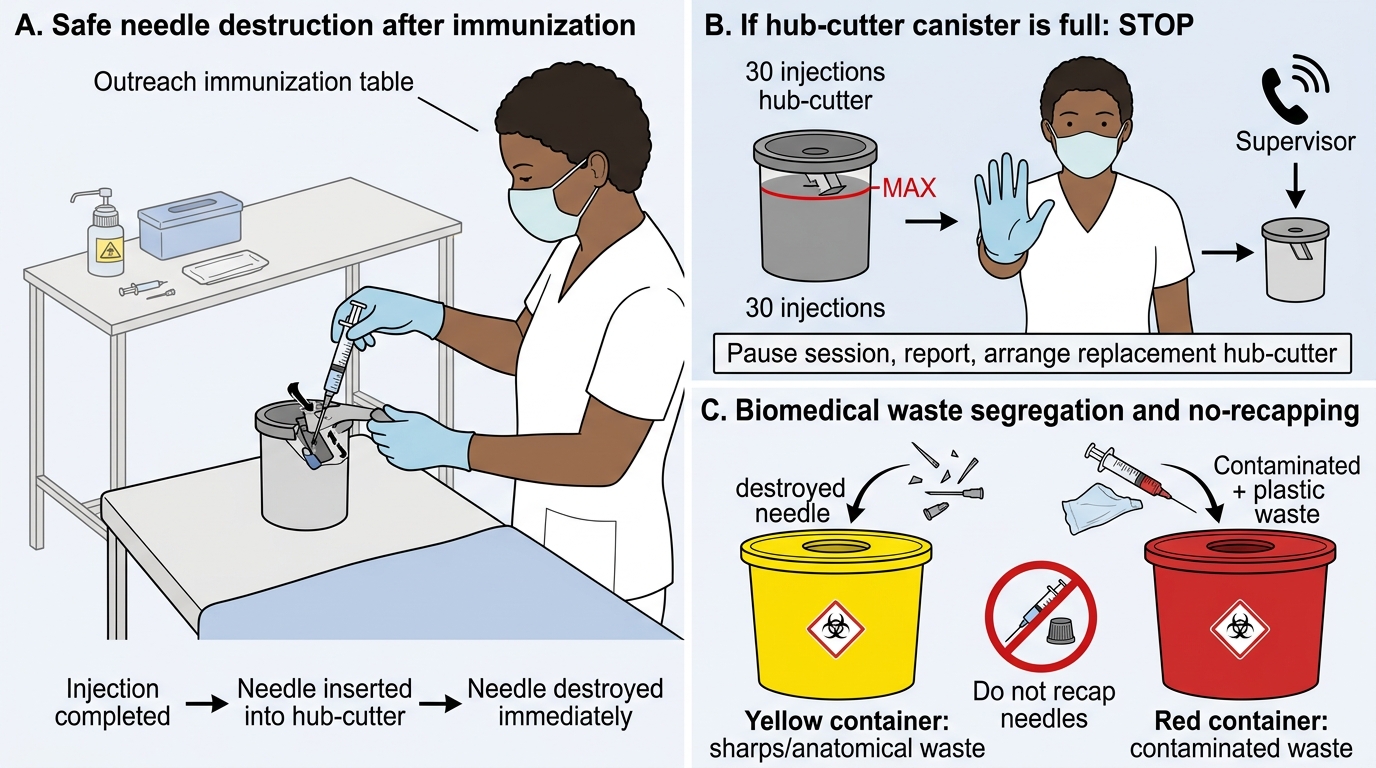
The hub-cutter: the most important single-use sharps safety device in immunization:
The hub-cutter (needle destroyer) is a battery-operated or hand-cranked device that shears the needle from the syringe barrel and collects the destroyed metal in a sealed canister at the point of use, immediately after injection. Its use achieves three goals simultaneously: (1) destroys the needle so it cannot be reused, (2) eliminates the need to recap (which is the most common cause of needle-stick injury), and (3) renders the syringe unusable for re-use. Hub-cutter use is mandatory in the UIP — every immunization session site must have one.
Colour-coded container system (BMW Rules 2016):
- Yellow container (puncture-proof, leak-proof): anatomical waste, pathological waste, sharps after hub-cutting (destroyed needle canisters go into this when the hub-cutter canister is full), discarded vaccines/vials. For immunization sessions: empty vaccine vials (except glass — see below) and hub-cutter canisters.
- Red container/bag (puncture-proof): contaminated recyclable waste (used syringes AFTER the needle has been removed by hub-cutter; the plastic barrel without needle is red bag waste).
- Blue/translucent bag: glass vials/ampoules — many vaccine vials are glass and go into the puncture-proof blue container.
- No-recapping rule: the needle MUST NOT be recapped after use. Recapping is the leading cause of accidental needle-stick in immunization workers.
Practical sequence at the session site:
1. Place the hub-cutter within arm's reach before starting the session.
2. After injecting, withdraw needle and immediately pass it through the hub-cutter aperture before setting down the syringe.
3. The decapitated syringe (barrel without needle) is dropped into the red bag.
4. Empty vaccine vials: mark them with a cross or break the glass (to prevent re-use) and place in the yellow container (plastic vials) or blue container (glass).
5. Soiled cotton swabs: yellow bag (non-sharp biological waste).
6. At end of session: seal all containers, label with date and immunization site, and dispatch through the facility's BMW chain to the treatment facility (common bio-medical waste treatment and disposal facility — CBWTF).
Needle-stick injury protocol:
If a health worker sustains a needle-stick injury: (a) allow the wound to bleed freely; (b) wash with soap and water for 10–15 minutes; (c) report to the facility supervisor and the infection-control officer IMMEDIATELY; (d) assess the source child's Hep-B and HIV status; (e) start post-exposure prophylaxis (PEP) for Hep-B (if worker is non-immune: Hep-B Ig + vaccine) and HIV (antiretroviral PEP) within 2–4 hours of exposure.
Biomedical Waste Segregation During Immunization Session
SELF-CHECK
At an outreach immunization session, the health worker uses a hub-cutter after each injection. After 30 injections, the hub-cutter canister is full. She is about to start injection 31 with no replacement hub-cutter available. Which is the MOST appropriate action?
A. Cap the used needle carefully using the one-hand scoop technique and drop it in the yellow container
B. Drop the entire used syringe-with-needle into the yellow container without recapping
C. Stop the session, report to the supervisor, and arrange a replacement hub-cutter before continuing
D. Detach the needle with the other hand and drop it into the yellow container
Reveal Answer
Answer: C. Stop the session, report to the supervisor, and arrange a replacement hub-cutter before continuing
When the hub-cutter is unavailable or full, the session MUST pause. Continuing without a functional needle-destruction mechanism forces health workers to recap (unsafe) or handle loose needles (unsafe). Option A (one-hand scoop) is a last-resort technique accepted ONLY when no other option exists and should be documented and reported. Option B (dropping needle-attached syringe) risks needle-stick injury to waste handlers. Option D (detaching by hand) is a direct needle-stick risk. The correct action is to pause and secure a replacement — this is both the safe and the procedurally correct response under BMW Rules 2016.
Supervised Practice: Observation and Mannequin Demonstration
Observation of live UIP vaccine administration (PE18.11) and mannequin demonstration (PE18.12) are complementary learning experiences that together bridge the gap between declarative knowledge and safe clinical performance. Observation builds familiarity with the real-world flow — patient positioning, vial handling, caregiver interaction, the ambient dynamics of the vaccination room — while mannequin practice develops and reinforces motor accuracy for the injection itself before any needle touches a child. Neither experience alone is sufficient: observation without practice leaves the learner without psychomotor confidence; practice without prior observation means the learner lacks a mental model of the clinical context. As you observe, use the structured checklist below to actively evaluate each dose administered — passive watching develops no competency. As you practise on the mannequin, seek faculty feedback after every complete injection cycle and specifically ask the faculty to confirm whether your BCG injection produced a visible bleb, whether your IM needle angle was correct, and whether you went to the hub-cutter without any attempt to recap. These three checkpoints catch the most common errors at the skill-acquisition stage.
Provided image
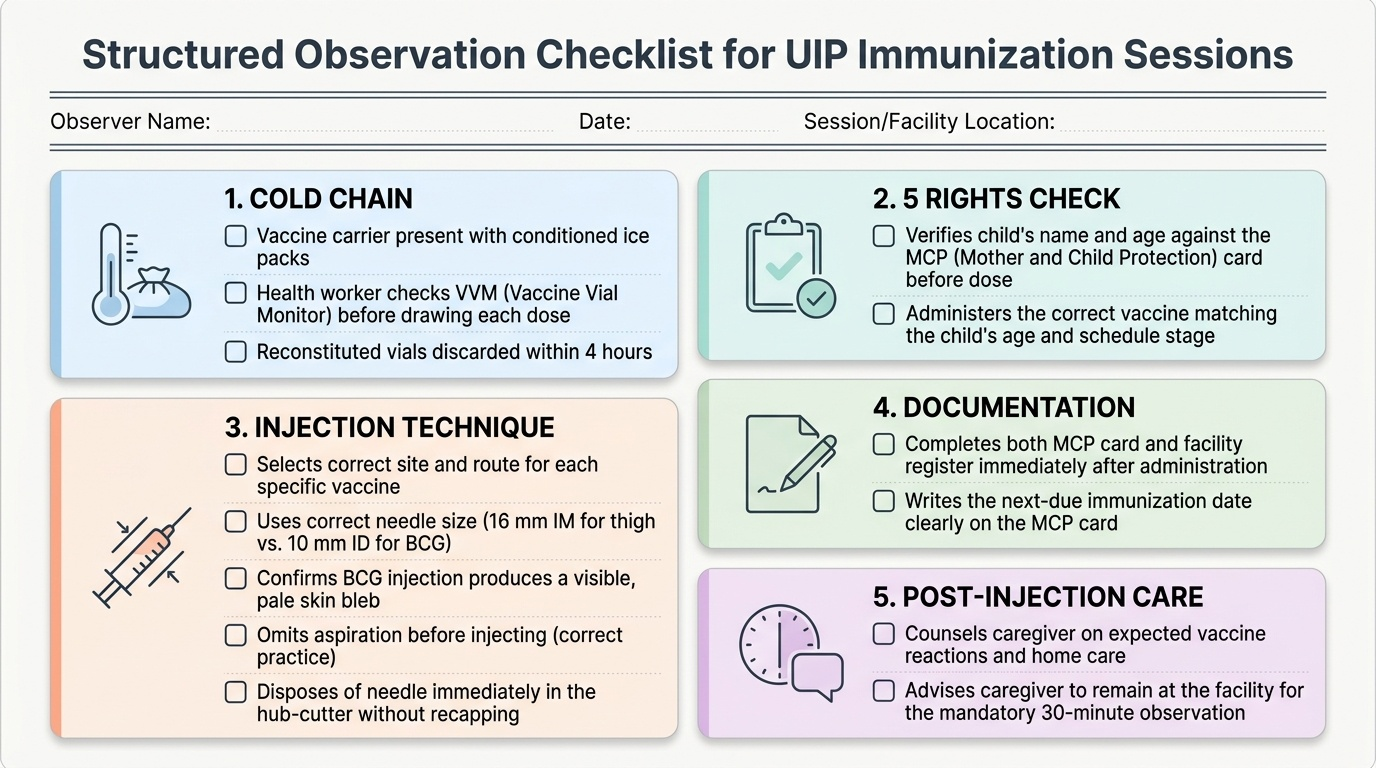
What to observe during a UIP immunization session (PE18.11 checklist):
As an observer, systematically watch for and mentally note the following at EACH dose administered:
Cold chain:
• Is the vaccine carrier present with ice packs?
• Does the health worker check the VVM before drawing up each dose?
• Are reconstituted vials discarded within 4 hours?
5 Rights check:
• Does the worker verify the child's name and age against the MCP card before each dose?
• Is the correct vaccine given for the child's age and schedule stage?
Technique:
• Which site and route is used for each vaccine?
• Is the needle size appropriate (16 mm IM for thigh vs 10 mm ID for BCG)?
• Is the BCG injection producing a visible bleb?
• Is aspiration omitted (correct) or performed (incorrect)?
• Is the needle immediately hub-cut after withdrawal, without recapping?
Documentation:
• Are both the MCP card and the facility register completed immediately?
• Is the next-due date written on the MCP card?
Post-injection:
• Is the caregiver counselled on expected reactions and the 30-minute observation rule?
• Is the child kept under observation before leaving?
Mannequin practice (PE18.12) — critical checkpoints:
Practice in this order, seeking faculty feedback after each complete cycle:
- Intradermal BCG technique — insert the 26 G needle almost parallel (15°) to the skin surface, bevel up; inject 0.05–0.1 mL to produce a tense bleb. Common errors: needle too deep (no bleb), needle too steep an angle (IM deposition), leakage of fluid around needle (poor seal).
- IM pentavalent at anterolateral thigh — palpate the correct site, stretch skin, insert 23–25 G 16 mm needle at 90°, inject without aspiration, withdraw, apply pressure. Common errors: gluteal site (never correct), failure to stretch skin, recapping after withdrawal.
- SC MR at right upper arm — pinch the subcutaneous tissue at the right upper arm, insert 25 G needle at 45°, inject, withdraw. Common errors: inserting at 90° (IM route), incorrect site (deltoid instead of upper arm).
Self-correction habit: after each practice injection, pause and ask yourself: Did I verify the site anatomically? Did the needle feel right? Did I go straight to the hub-cutter? Good injection practice is a psychomotor skill that deepens with deliberate self-reflection after each repetition.
Self-Assessment: Safe Vaccine Practice
Integrating the full safe-vaccination workflow into autonomous clinical practice requires not just factual recall but the ability to apply principles under time pressure, with imperfect equipment, and in the face of caregiver anxiety. This self-assessment section tests your command of the key decision points covered in this module before you encounter them in a real immunization session. Work through each scenario below without referring back to earlier sections; then check your reasoning against the explanations. The goal is not to memorise answers but to identify any gaps in your understanding that require a second reading or a question for your clinical supervisor. The scenarios are calibrated to the level of a final-year MBBS student who has observed at least one immunization session and completed the mannequin demonstration.
Scenario 1 — Site identification: You are administering pentavalent-1 to a 6-week-old infant. State the injection site, needle gauge, length, and angle you would use, and explain why the anterolateral thigh is preferred over the deltoid at this age.
Expected reasoning: Anterolateral thigh (vastus lateralis, middle third, lateral aspect); 23–25 G, 16 mm needle at 90°. The infant deltoid lacks sufficient muscle mass at 6 weeks for IM injection. The gluteal site is never acceptable due to sciatic nerve risk.
Scenario 2 — AEFI classification: Three children from the same immunization session develop fever and local swelling at 24 hours; one has a fluctuant abscess. The health worker used a single multi-dose vial across all three without changing gloves between children. Classify this AEFI and state your next action.
Expected reasoning: Immunization error–related (programme error) AEFI — the failure to change gloves and the shared vial handling represents a contamination pathway. Report to the district AEFI committee within 24 hours; ensure affected children receive clinical assessment; document and retrain the health worker on NTAT and the multi-dose vial policy.
Scenario 3 — Documentation: A caregiver presents a 9-month-old child for MR vaccine. The MCP card is torn — BCG and pentavalent-1 are confirmed; all subsequent entries are illegible. What is your approach?
Expected reasoning: Unknown vaccination status = treat as unvaccinated for the unreadable doses. Administer MR today (due at 9 months regardless). For the pentavalent series, if only dose 1 is confirmed, schedule doses 2 and 3 with minimum 4-week intervals. Issue a new MCP card and document today's administration with full details (vaccine, batch, site, VVM, next-due date). Do not fabricate or assume doses were given.