Page 18 of 53
PE19.7 | Hemorrhagic Disease of Newborn — SDL Guide
Learning Objectives
- Explain the pathophysiology of Vitamin K Deficiency Bleeding (VKDB) in neonates
- Classify VKDB into early, classic, and late forms with their timing, aetiology, and clinical features
- Describe the laboratory findings in VKDB and differentiate from DIC and thrombocytopenia
- Outline the management of acute VKDB and explain the rationale for universal neonatal Vitamin K prophylaxis
- Identify at-risk groups requiring additional Vitamin K supplementation
INSTRUCTIONS
Haemorrhagic disease of the newborn (HDN), now termed Vitamin K Deficiency Bleeding (VKDB), is a preventable cause of neonatal morbidity and mortality. Late VKDB — occurring in breastfed infants who did not receive prophylaxis — carries a 30–60% risk of intracranial haemorrhage, making this one of the most consequential preventable neonatal conditions. Understanding the four converging reasons why neonates are physiologically Vitamin K-deficient, and the straightforward solution (1 mg IM at birth), is essential knowledge for every clinician involved in neonatal care.
References
- Ghai Essential Pediatrics, 9th ed., Ch 8 — Newborn Infant (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 115 — Blood Disorders in the Newborn (textbook)
- IAP Standard Treatment Guidelines — VKDB Prophylaxis and Management (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 6-week-old exclusively breastfed infant is brought to the emergency with a bulging fontanelle and drowsiness. The parents report no trauma. CT scan reveals a large intracranial haemorrhage. The birth records show: normal delivery, birth weight 3.1 kg, discharged at 48 hours. There is no entry in the discharge summary for Vitamin K injection. This child has late Vitamin K Deficiency Bleeding (VKDB) — now the leading cause of late-onset intracranial haemorrhage in the first 3 months of life in unsupplemented breastfed infants. This scenario, which occurs every week in Indian paediatric hospitals, is almost entirely preventable with a single 1 mg IM injection at birth.
WHY THIS MATTERS
VKDB is one of the clearest examples of a preventable paediatric catastrophe. Global incidence without prophylaxis is estimated at 4–7 per 100,000 live births, but with the prevalence of exclusive breastfeeding in India and variable implementation of prophylaxis at facility deliveries, the true burden is higher. Unlike many neonatal conditions that require complex interventions, VKDB prevention requires a single low-cost injection. Yet, when prophylaxis is missed — as happens in home deliveries, early discharges, or administrative oversights — the consequences range from umbilical stump oozing (mild, treatable) to fatal intracranial haemorrhage (late VKDB). Every future clinician must be able to counsel parents about this prophylaxis, administer it correctly, and recognise VKDB when it presents.
RECALL
From your biochemistry, recall that Vitamin K is a fat-soluble vitamin (along with Vitamins A, D, and E), which means its absorption requires dietary fat and bile salts. Vitamin K1 (phytomenadione) is found in green leafy vegetables and certain plant oils; Vitamin K2 (menaquinone) is synthesised by gut bacteria. Recall from biochemistry that Vitamin K is the essential cofactor for the enzyme that gamma-carboxylates specific glutamic acid residues on clotting factors — a post-translational modification required for calcium binding and therefore coagulant activity. Without this carboxylation, the factors are produced as PIVKA (Proteins Induced by Vitamin K Absence) — structurally present but functionally inactive. From pharmacology, recall that warfarin works by inhibiting Vitamin K epoxide reductase, thus blocking this same carboxylation reaction. This mechanistic link between warfarin and VKDB is clinically important when mothers take anticoagulants.
Clinical Presentation of VKDB: When Neonates Bleed Unexpectedly
Vitamin K Deficiency Bleeding (VKDB) — the modern term preferred over the older 'haemorrhagic disease of the newborn' — presents as spontaneous or excessive bleeding in a neonate, in the absence of trauma, sepsis, or platelet disorder. The recognition of VKDB hinges on two clinical features: the age of the bleeding neonate and the absence of another explanation for the coagulopathy.
Bleeding sites vary by form but commonly include: the umbilical stump (oozing for >48 hours), scalp cephalhaematoma (expanding or failing to resolve), gastrointestinal tract (haematemesis, melaena, or blood-streaked stools), post-circumcision site, intracranial haemorrhage (bulging fontanelle, convulsions, decreased consciousness), and bleeding from venepuncture sites.
Clinical alert signs that reliably distinguish VKDB from benign minor neonatal bleeding and require immediate investigation include:
- Bleeding persisting beyond 24–48 hours from the same site
- Bleeding from multiple sites simultaneously
- Intracranial signs in any age group: bulging fontanelle, seizures, irritability, or decreased tone in a previously well infant — these point to late VKDB until proven otherwise
- History of no Vitamin K prophylaxis at birth, combined with exclusive breastfeeding
- Maternal drug history (warfarin, anticonvulsants) for early VKDB
The temporal classification of VKDB (early, classic, late) is central to understanding the aetiology and guiding management in each presentation. A well infant who has not received prophylaxis and begins bleeding at 6 weeks has an entirely different cause (late VKDB, often with underlying malabsorption or cholestatic liver disease) compared to the healthy 3-day-old who bleeds from the umbilical stump (classic VKDB).
IMPORTANT DIFFERENTIAL: Haematemesis in the first 24–48 hours may be due to swallowed maternal blood rather than VKDB — the Apt-Downey test distinguishes fetal haemoglobin (resistant to alkali) from maternal haemoglobin (denatures pink → yellow-green with NaOH). A positive Apt test (blood remains pink) suggests fetal origin = VKDB or DIC; maternal blood ingestion is a benign cause.
IMPORTANT DISTINCTION from DIC: In DIC, there is concurrent thrombocytopenia, elevated D-dimers, evidence of a triggering illness (sepsis, asphyxia, shock), and the clinical context is a sick infant. In VKDB, the neonate is typically well — normal activity, no sepsis, no thrombocytopenia — only the coagulation is impaired.
IMPORTANT DISTINCTION from haemophilia A/B: Haemophilia presents in males, PT is normal (haemophilia A = Factor VIII deficiency, haemophilia B = Factor IX deficiency — both intrinsic pathway), and family history may be positive. In VKDB, PT is prolonged with aPTT also prolonged, and both male and female infants are affected.
Why Neonates Are Vitamin K Deficient
Pathophysiology and Aetiology: Why Neonates Are Vitamin K Deficient
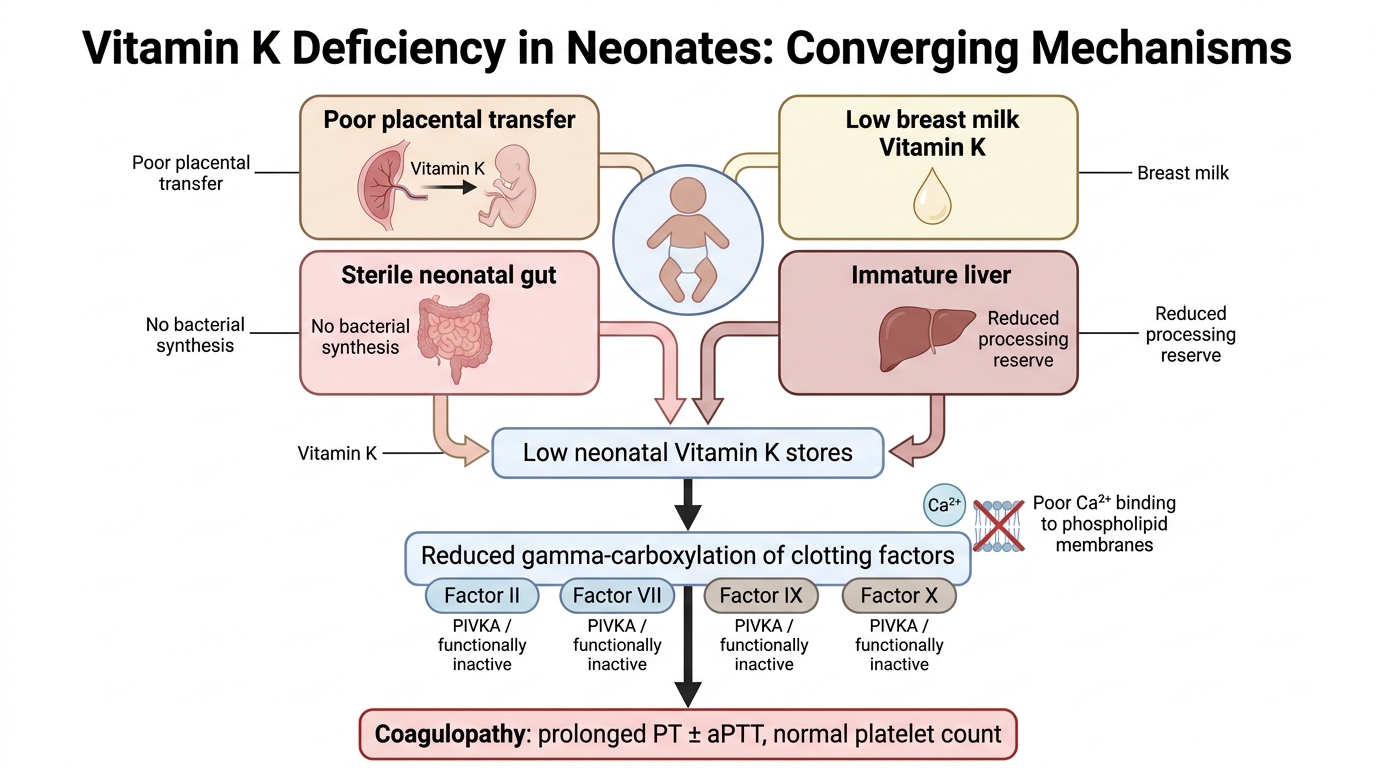
Vitamin K is the essential cofactor for the enzyme Vitamin K-dependent carboxylase, which gamma-carboxylates glutamic acid residues on clotting factors II (prothrombin), VII, IX, and X — the four factors of the common and extrinsic/intrinsic convergence pathway — as well as the anticoagulant proteins C and S. Gamma-carboxylation creates calcium-binding sites on these factors that allow them to attach to phospholipid membranes and function in the coagulation cascade. Without Vitamin K, these proteins are synthesised by the liver but remain functionally inactive — they are called PIVKA (Proteins Induced by Vitamin K Absence or Antagonism). The result is a selective prolongation of the PT (which tests the extrinsic pathway: factors I, II, V, VII, X) and aPTT (intrinsic: VIII, IX, XI) with normal platelet count.
Four converging reasons explain why neonates — especially breastfed neonates — are physiologically Vitamin K-deficient at birth:
- Poor placental transfer: Vitamin K crosses the placenta very poorly. Cord blood Vitamin K levels are far below maternal levels, and the activity of Vitamin K-dependent clotting factors is physiologically low in all neonates at birth (~20–60% of adult levels for factors II, VII, IX, X).
- Low content in human breast milk: Human breast milk contains only 1–4 mcg/L of Vitamin K — a minute amount compared with formula milk (~55 mcg/L). This means exclusively breastfed infants receive negligible Vitamin K from feeds. Formula-fed infants receive sufficient Vitamin K from fortified formula and rarely develop VKDB.
- Sterile gut in the newborn: Gut bacteria (particularly Bacteroides fragilis and Escherichia coli) synthesise Vitamin K2 (menaquinone) in the colon. The newborn gut is sterile at birth; colonisation takes days to weeks. In the interim, there is no endogenous Vitamin K synthesis from gut flora.
- Immature hepatic synthesis: The neonatal liver has reduced ability to synthesise Vitamin K-dependent clotting factors even when Vitamin K is available — prematurity exacerbates this further.
In early VKDB, maternal drugs that antagonise Vitamin K (warfarin crosses the placenta; anticonvulsants such as phenytoin, phenobarbitone, and carbamazepine; anti-TB drugs rifampicin and isoniazid) add a fifth pathogenic factor — drug-mediated suppression of Vitamin K activity in both mother and fetus.
In late VKDB, a sixth factor comes into play: malabsorption of Vitamin K (fat-soluble) in infants with cholestatic liver disease (e.g., biliary atresia, neonatal hepatitis, Alagille syndrome) or cystic fibrosis. These infants may develop late VKDB even if they received prophylaxis at birth, because fat-soluble vitamin absorption is chronically impaired.
SELF-CHECK
A 5-day-old exclusively breastfed infant has oozing from the umbilical stump for 2 days and blood-streaked stools. PT is markedly prolonged, aPTT is prolonged, platelet count is 220,000. The baby is active and feeding well. What is the most likely diagnosis and what is the immediate treatment?
A. Disseminated intravascular coagulation (DIC) — treat underlying sepsis
B. Classic VKDB — administer Vitamin K1 1 mg IM/IV
C. Haemophilia A — fresh frozen plasma transfusion
D. Thrombocytopenic purpura — IV immunoglobulin
Reveal Answer
Answer: B. Classic VKDB — administer Vitamin K1 1 mg IM/IV
This is classic VKDB: 5-day-old breastfed infant with bleeding from umbilical stump and GI tract; prolonged PT and aPTT but NORMAL platelet count (platelet count is normal in VKDB — differentiating from DIC where thrombocytopenia occurs); the infant is well (against DIC). Treatment is Vitamin K1 1 mg IM or IV. DIC requires a sick trigger (sepsis, asphyxia), has thrombocytopenia, and elevated D-dimers. Haemophilia A has normal PT (Factor VIII = intrinsic path only → aPTT prolonged, PT normal). Thrombocytopenic purpura is excluded by the normal platelet count.
Classification of VKDB: Early, Classic, and Late Forms
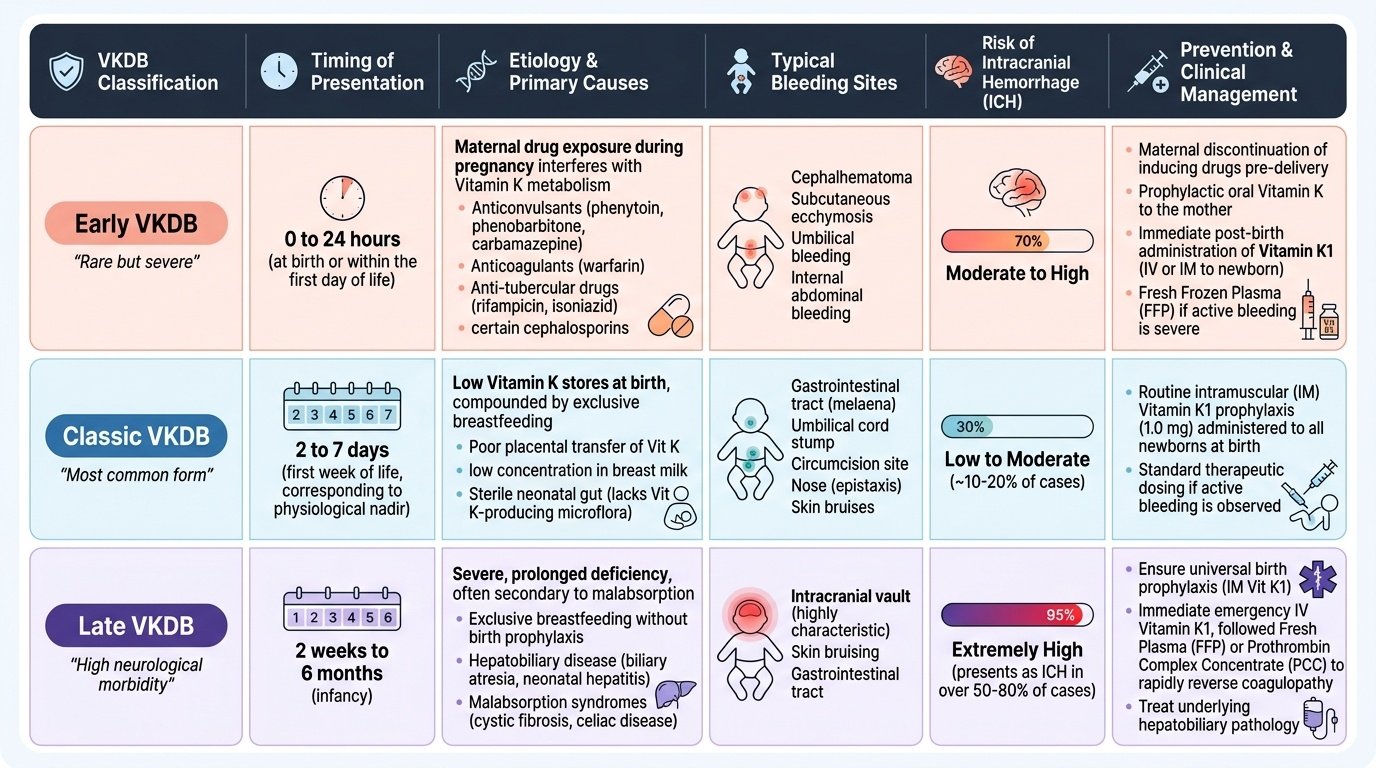
VKDB is classified into three forms based on the timing of presentation, each with distinct aetiology, clinical features, bleeding sites, and risk of serious complications. This classification is not merely academic — it directly determines the management strategy and identifies the at-risk groups who require targeted intervention. Understanding the temporal pattern of VKDB is essential for any clinician examining a bleeding neonate or young infant, because the same condition — Vitamin K-dependent clotting factor deficiency — presents in entirely different clinical contexts depending on when in postnatal life the Vitamin K store is depleted. Early VKDB is caused by maternal drug exposure, classic VKDB by the physiological nadir in unsupplemented breastfed infants, and late VKDB by ongoing dietary deficiency or malabsorption. The following comparison illustrates the key distinguishing features of all three forms:
Provided image
Early VKDB (within 24 hours of birth) is the most dramatic but least common form. It is almost always caused by maternal drug use during pregnancy — specifically drugs that antagonise Vitamin K or induce hepatic Vitamin K catabolism: warfarin (oral anticoagulant, crosses placenta), antiepileptic drugs (phenytoin, phenobarbitone, carbamazepine), anti-tubercular drugs (rifampicin, isoniazid), and some cephalosporins. The infant is born already deficient because the maternal drug depleted Vitamin K in the fetal compartment. Bleeding typically occurs at multiple sites — cephalhaematoma, subcutaneous ecchymosis, intracranial haemorrhage, gastrointestinal, or surgical wound sites. This form carries the highest risk of intracranial haemorrhage among early forms. Prevention requires antenatal supplementation: pregnant women on these drugs should receive Vitamin K1 10 mg orally daily in the last month of pregnancy (or IM in the last week), and the neonate should receive prophylaxis immediately at birth.
Classic VKDB (days 2–7 of life) is the most common form. It occurs in exclusively breastfed infants who did not receive Vitamin K prophylaxis at birth — the physiological nadir of Vitamin K-dependent factor activity. Bleeding is typically from the umbilical stump, circumcision site, venepuncture sites, or gastrointestinal tract. The infant is otherwise well; platelet count and fibrinogen are normal. The risk of intracranial haemorrhage is lower than in early or late VKDB. Response to Vitamin K administration is rapid and reliable.
Late VKDB (2 weeks to 6 months of age) is the most clinically serious form. It occurs in exclusively breastfed infants who did not receive prophylaxis at birth, or in infants with conditions causing fat-soluble vitamin malabsorption: biliary atresia (the most important associated condition), neonatal hepatitis, Alagille syndrome, cystic fibrosis, alpha-1 antitrypsin deficiency, or prolonged antibiotic use that suppresses gut flora. Up to 30–60% of late VKDB cases present with intracranial haemorrhage — this is the defining danger. Other sites include subcutaneous and mucosal bleeding. A clinically important point: the infant with biliary atresia who received prophylaxis at birth may still develop late VKDB because ongoing malabsorption depletes Vitamin K; these infants need repeated supplementation (Vitamin K1 1 mg IM weekly or 2 mg oral alternate day, under specialist guidance).
CLINICAL PEARL
The single most important clinical pearl in VKDB is that the late form presents in a previously well infant who has not appeared jaundiced — the classic cholestatic liver disease connection. Every young infant presenting with unexpected intracranial haemorrhage must be screened for VKDB. Check: (1) Was Vitamin K given at birth? (Record, parental recall, or birth centre confirmation.) (2) Is there any cholestatic jaundice (persistent jaundice >2 weeks, pale/acholic stools, dark urine)? Biliary atresia and other cholestatic conditions must be excluded in all infants with late VKDB, because they require ongoing supplementation and specific treatment. A quick bedside observation: look at the stool colour — pale/white acholic stools in a 4-week-old with VKDB should prompt urgent hepatology referral.