Page 19 of 53
PE19.7 | Hemorrhagic Disease of Newborn — SDL Guide (Part 2)
Diagnosis and Investigation
The diagnosis of VKDB is primarily clinical, supported by targeted coagulation investigations. The diagnostic approach must be efficient — a severely bleeding neonate cannot wait for an extended workup; treatment (Vitamin K1) can be administered empirically while investigations are in progress. The diagnostic strategy serves two goals: confirming VKDB and excluding other haematological conditions whose management differs significantly.
The core investigation set in a bleeding neonate with suspected VKDB includes: prothrombin time (PT/INR), activated partial thromboplastin time (aPTT), platelet count, fibrinogen, and complete blood count. The characteristic laboratory pattern of VKDB is a markedly prolonged PT with a prolonged aPTT, normal platelet count, and normal fibrinogen — reflecting isolated deficiency of the Vitamin K-dependent coagulation factors (II, VII, IX, X) without consumptive coagulopathy or platelet destruction.
Key differentials and their distinguishing features:
- DIC (Disseminated Intravascular Coagulation): prolonged PT + aPTT + elevated D-dimers + thrombocytopenia + reduced fibrinogen + sick infant with a triggering condition (sepsis, perinatal asphyxia, shock). The infant with VKDB is characteristically well.
- Haemophilia A (Factor VIII deficiency): aPTT prolonged, PT NORMAL (Factor VIII is purely in the intrinsic pathway), platelet count normal, affects males predominantly, family history may be present.
- Haemophilia B (Factor IX deficiency): aPTT prolonged, PT normal — same pattern as Haemophilia A, differentiated by specific factor assay.
- Swallowed maternal blood: presents as haematemesis or melaena in first 1–2 days, Apt-Downey test positive (fetal Hb resistant to alkali denaturation → blood remains pink); coagulation studies are normal.
- Thrombocytopenia (immune or alloimmune): normal PT and aPTT, markedly low platelet count, skin petechiae.
PIVKA-II assay: Proteins Induced by Vitamin K Absence (des-gamma-carboxyprothrombin) — the most sensitive specific marker of Vitamin K deficiency, detectable before PT prolongs. Not available in routine laboratories but used in research and specialist centres.
Imaging: CT head (non-contrast) is mandatory in any infant with neurological signs (bulging fontanelle, seizures, decreased consciousness) to identify intracranial haemorrhage and guide neurosurgical decision-making. Urgent creatinine, liver enzymes (ALT, GGT, bilirubin fractions) in late VKDB to screen for cholestatic liver disease.
SELF-CHECK
In Vitamin K Deficiency Bleeding, what is the expected pattern of coagulation tests?
A. Prolonged PT, normal aPTT, low platelet count
B. Normal PT, prolonged aPTT, normal platelet count
C. Prolonged PT, prolonged aPTT, normal platelet count, normal fibrinogen
D. Prolonged PT, prolonged aPTT, low platelet count, reduced fibrinogen
Reveal Answer
Answer: C. Prolonged PT, prolonged aPTT, normal platelet count, normal fibrinogen
VKDB causes deficiency of Vitamin K-dependent factors II, VII, IX, and X — these participate in both the extrinsic (PT) and intrinsic (aPTT) pathways. Both PT and aPTT are prolonged. Platelet count and fibrinogen are NORMAL because VKDB is not a consumptive process. Option A (low platelets) points to DIC or thrombocytopenia. Option B (normal PT) is the Haemophilia A/B pattern (purely intrinsic pathway). Option D (low platelets + low fibrinogen) is the DIC pattern — indicating consumption and fibrin deposition, typically seen in a sick infant.
Management: Acute Treatment and Prevention
Management of VKDB consists of two components: acute treatment of the bleeding episode, and prevention through universal neonatal prophylaxis. The latter is far more important — it is the reason why VKDB is now largely a preventable disease in countries with systematic neonatal care. The acute treatment corrects the immediate haemorrhage; the preventive injection at birth ensures the condition never arises. In clinical practice, both must be understood with precision because the dose, route, and timing of Vitamin K administration vary by the urgency of the situation.
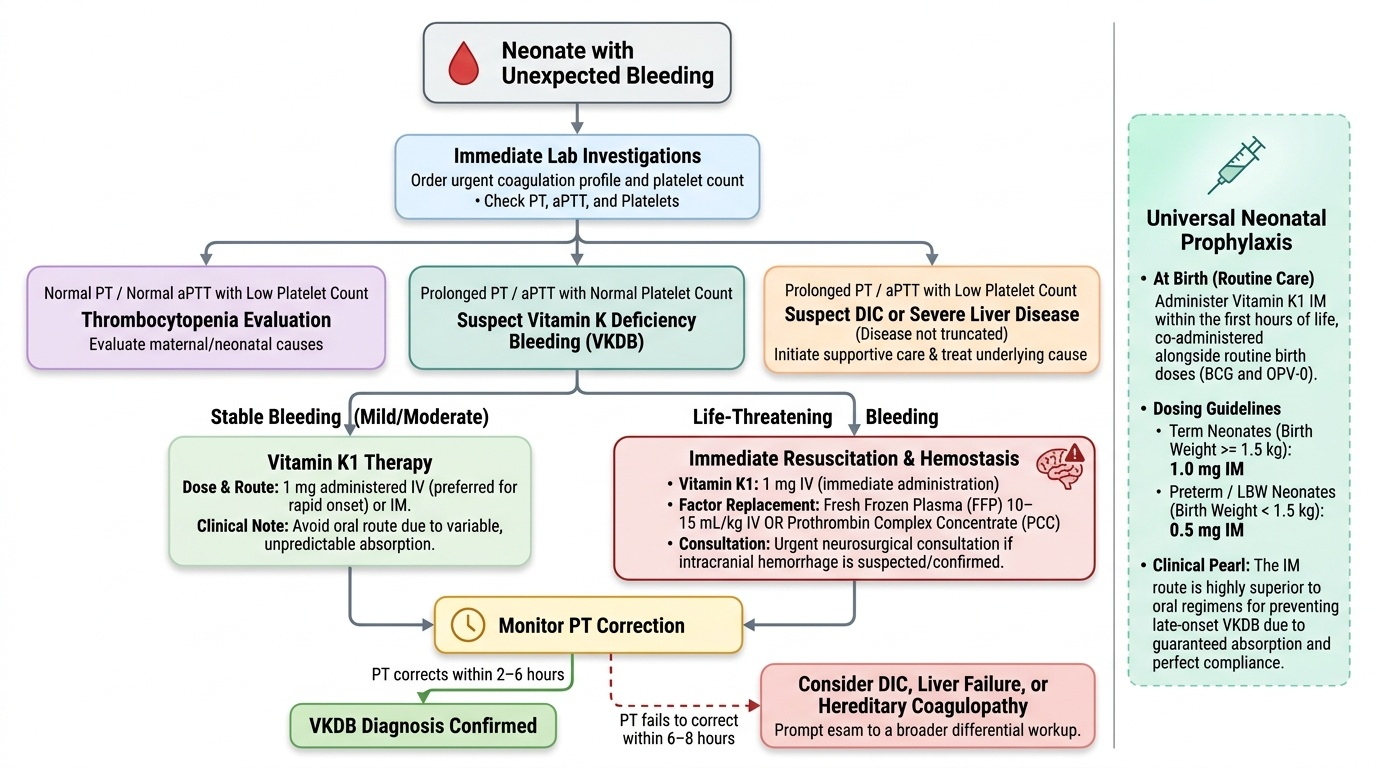
Provided image
Acute treatment of VKDB:
The cornerstone of treatment is Vitamin K1 (phytomenadione) administered intravenously or intramuscularly. The response is not immediate — new functional clotting factors must be synthesised by the liver — so for active haemorrhage, Vitamin K must be combined with immediate factor replacement. Dosing guidelines:
- Dose: 1 mg IV or IM for all term neonates and infants
- Route: IV is preferred in actively bleeding infants for faster onset; IM is acceptable in stable infants
- Response: PT begins to correct within 2–6 hours of IV Vitamin K; if PT does not correct within 6–8 hours, consider DIC or liver failure as the diagnosis rather than VKDB
- ORAL Vitamin K has variable absorption and is NOT appropriate for acute treatment
For life-threatening bleeding (particularly intracranial haemorrhage) where immediate haemostasis is required while Vitamin K is acting:
- Fresh Frozen Plasma (FFP): 10–15 mL/kg IV — provides immediate clotting factors (all of them, not just Vitamin K-dependent)
- Prothrombin Complex Concentrate (PCC): faster, smaller volume, contains concentrated factors II, VII, IX, X — available in some centres
- Neurosurgical consultation for significant intracranial haemorrhage requiring evacuation
Universal neonatal Vitamin K prophylaxis — the prevention:
The Indian National Immunization Schedule (NIS) and IAP recommend Vitamin K1 1 mg intramuscularly for all neonates at birth, administered as part of the routine birth dose along with BCG and OPV-0. For low birth weight neonates, the dose is 0.5 mg IM if birth weight <1.5 kg.
IM Vitamin K is superior to oral regimens for late VKDB prevention because oral administration requires multiple doses (and compliance is imperfect), and fat-soluble vitamin absorption may be impaired in infants with undiagnosed liver disease. A single IM injection provides sustained Vitamin K stores for months.
Special risk groups requiring additional attention:
- Infants born to mothers on anticonvulsants, warfarin, anti-TB drugs: antenatal maternal Vitamin K supplementation (10 mg oral/day in last 4 weeks) + ensure neonatal prophylaxis is administered promptly
- Infants with persistent jaundice beyond 2 weeks: screen for cholestatic liver disease; if cholestatic jaundice is present, repeat Vitamin K1 IM monthly (or as per specialist guidance) because fat malabsorption will deplete stores
- Home deliveries without medical supervision: confirm with the family at first postnatal visit whether Vitamin K was given; if not, administer immediately
IMPORTANT CLINICAL NOTE: The (now debunked) concern that IM Vitamin K at birth increases childhood cancer risk was based on a single 1992 study by Golding et al. — it has been extensively studied and refuted by multiple large cohort studies. Parents who ask about this concern should be clearly reassured.
SELF-CHECK
Which statement about Vitamin K prophylaxis in newborns is CORRECT per the Indian National Immunization Schedule?
A. Oral Vitamin K 2 mg is the preferred route for all neonates in India
B. Vitamin K prophylaxis is only recommended for premature infants weighing <1.5 kg
C. Vitamin K1 1 mg IM is recommended for all neonates at birth; 0.5 mg IM if birth weight <1.5 kg
D. Vitamin K prophylaxis is only required for infants born to mothers with anticoagulant therapy
Reveal Answer
Answer: C. Vitamin K1 1 mg IM is recommended for all neonates at birth; 0.5 mg IM if birth weight <1.5 kg
Per IAP guidelines and the National Immunization Schedule, ALL neonates receive Vitamin K1 1 mg IM at birth (universal prophylaxis, not just for high-risk groups). The dose is adjusted to 0.5 mg IM for very low birth weight infants (<1.5 kg). IM is the preferred route over oral for prophylaxis because it provides reliable absorption and sustained effect regardless of feeding or intestinal absorption status. Oral regimens require multiple doses and are less reliable for preventing late VKDB.
Self-Assessment: VKDB Scenarios
Apply your understanding of VKDB to the following clinical scenarios. Work through each case independently before reading the reasoning. Each scenario is designed to test a different aspect of the VKDB framework: recognition of the classic form, management of the most dangerous late form with intracranial haemorrhage, and prevention counselling for a high-risk mother. The ability to approach these scenarios systematically — using timing, feeding history, prophylaxis status, and coagulation results — will serve you in clinical practice far better than memorising facts in isolation.
Case 1 — Classic VKDB: A 5-day-old exclusively breastfed infant is brought in because the umbilical stump has been oozing since day 3. The mother says the baby has been feeding well and has not seemed unwell. On examination, the baby is active, fontanelle is flat, and there is a small haematoma at the venepuncture site from the heel prick test. Birth records show the baby was delivered at home by a traditional birth attendant. No Vitamin K was recorded as given.
- Diagnosis: Classic VKDB (day 5, breastfed, no prophylaxis, well infant, multiple bleeding sites)
- Investigations: PT/aPTT (expect both prolonged), platelet count (expect normal), FBC
- Management: Vitamin K1 1 mg IM immediately; expect resolution of bleeding within 12–24 hours; counsel on prophylaxis for future pregnancies
Case 2 — Late VKDB: A 7-week-old breastfed infant presents with seizures and a tense, bulging fontanelle. Parents report the baby was well until yesterday. There is a history of persistent jaundice with pale stools noticed since 3 weeks. Emergency CT shows subdural haematoma. PT is markedly prolonged, aPTT prolonged, platelets normal.
- Diagnosis: Late VKDB with intracranial haemorrhage, likely secondary to cholestatic liver disease (biliary atresia — pale stools + jaundice)
- Immediate management: Vitamin K1 1 mg IV stat + FFP 10–15 mL/kg + neurosurgery consultation + NICU admission
- Further workup: liver function tests, direct bilirubin (conjugated fraction), abdominal USG + HIDA scan for biliary atresia
- Key point: this infant needs Kasai portoenterostomy for biliary atresia and ongoing Vitamin K supplementation
Case 3 — Early VKDB prevention: A G2P1 woman at 36 weeks gestation is seen in antenatal clinic. She has epilepsy and has been on phenytoin throughout the pregnancy. She asks about risks to her newborn.
- Key counselling: phenytoin crosses the placenta and interferes with Vitamin K metabolism in the fetus — early VKDB (within 24 hours of birth) risk is elevated
- Antenatal management: advise Vitamin K1 10 mg orally daily in the last 4 weeks of pregnancy
- Postnatal management: Vitamin K1 1 mg IM immediately at birth (do not wait for the routine schedule); monitor for bleeding in the first 24 hours