Page 32 of 53
PE19.11 | Neonatal Hypocalcemia — SDL Guide (Part 2)
Diagnosis: Laboratory and ECG Findings
The diagnosis of neonatal hypocalcemia is confirmed by laboratory measurement. Ionised calcium is the preferred diagnostic test because it measures the biologically active fraction directly and is not confounded by hypoalbuminaemia (common in sick neonates). A blood gas analyser or ion-selective electrode can measure ionised calcium rapidly at the bedside. Total serum calcium is an acceptable surrogate when ionised calcium is unavailable, but requires correction for albumin: for every 1 g/dL fall in serum albumin below 4 g/dL, total calcium is underestimated by approximately 0.8 mg/dL. In the clinical context of a symptomatic neonate, do not wait for a corrected calcium calculation — treat based on the clinical picture and total calcium. The aetiological workup is equally important: simply confirming hypocalcemia is not enough — you must also determine whether it is driven by phosphate overload, magnesium depletion, vitamin D insufficiency, or a structural parathyroid defect, because each demands a different long-term management plan and some (notably DiGeorge syndrome) have life-threatening non-metabolic implications.
Diagnostic thresholds:
- Total serum calcium <7.5 mg/dL (term neonate) or <7.0 mg/dL (preterm) — hypocalcemia
- Ionised calcium <1.0 mmol/L — hypocalcemia (most reliable threshold)
- QTc >0.45 seconds on ECG — highly suggestive of hypocalcemia
Aetiological workup (once hypocalcemia is confirmed):
- Serum phosphate: elevated in late-onset (phosphate overload) or hypoparathyroidism; low/normal in vitamin D deficiency
- Serum magnesium: hypomagnesaemia (<0.6 mmol/L) causes PTH-resistant hypocalcemia — must be corrected first
- PTH level: low/inappropriately normal in hypoparathyroidism; elevated in vitamin D deficiency
- 25-hydroxyvitamin D: low in vitamin D deficiency
- Renal function: phosphate retention worsened by impaired renal excretion
- Chromosomal microarray or FISH for 22q11.2 deletion if DiGeorge syndrome is suspected (cardiac defects, dysmorphia, T-cell immunodeficiency)
ECG monitoring is mandatory before and during IV calcium therapy. A prolonged QTc before treatment confirms the diagnosis; a paradoxical further QTc prolongation or bradycardia during infusion signals too-rapid administration and mandates slowing or stopping the infusion.
SELF-CHECK
A 6-day-old term neonate on cow's milk formula presents with facial twitching. Serum calcium is 6.5 mg/dL and serum phosphate is 9.2 mg/dL. What is the most likely mechanism?
A. Transient neonatal hypoparathyroidism due to prematurity
B. Phosphate overload from high-phosphate cow's milk suppressing ionised calcium
C. DiGeorge syndrome with congenital parathyroid aplasia
D. Hypocalcemia secondary to vitamin D deficiency in the mother
Reveal Answer
Answer: B. Phosphate overload from high-phosphate cow's milk suppressing ionised calcium
The combination of age (day 6, late-onset), cow's milk formula feeding, elevated phosphate (9.2 mg/dL), and low calcium points to phosphate overload — the classic late-onset mechanism. Cow's milk has ~6× the phosphate content of breast milk. The neonatal kidney cannot excrete this load; rising serum phosphate chelates ionised calcium, precipitating hypocalcemia. DiGeorge would present with persistent hypoparathyroidism and normal/low phosphate. Vitamin D deficiency would show low phosphate (not elevated). Prematurity-related hypocalcemia presents in the first 72 hours, not day 6.
Management of Neonatal Hypocalcemia
Management is guided by symptom severity and the underlying aetiology. The primary objectives are to rapidly restore ionised calcium to a safe level in symptomatic cases, provide sustained supplementation during the vulnerable period, and address any contributing factors — particularly hypomagnesaemia, which renders hypocalcemia refractory to calcium treatment alone.
Provided image
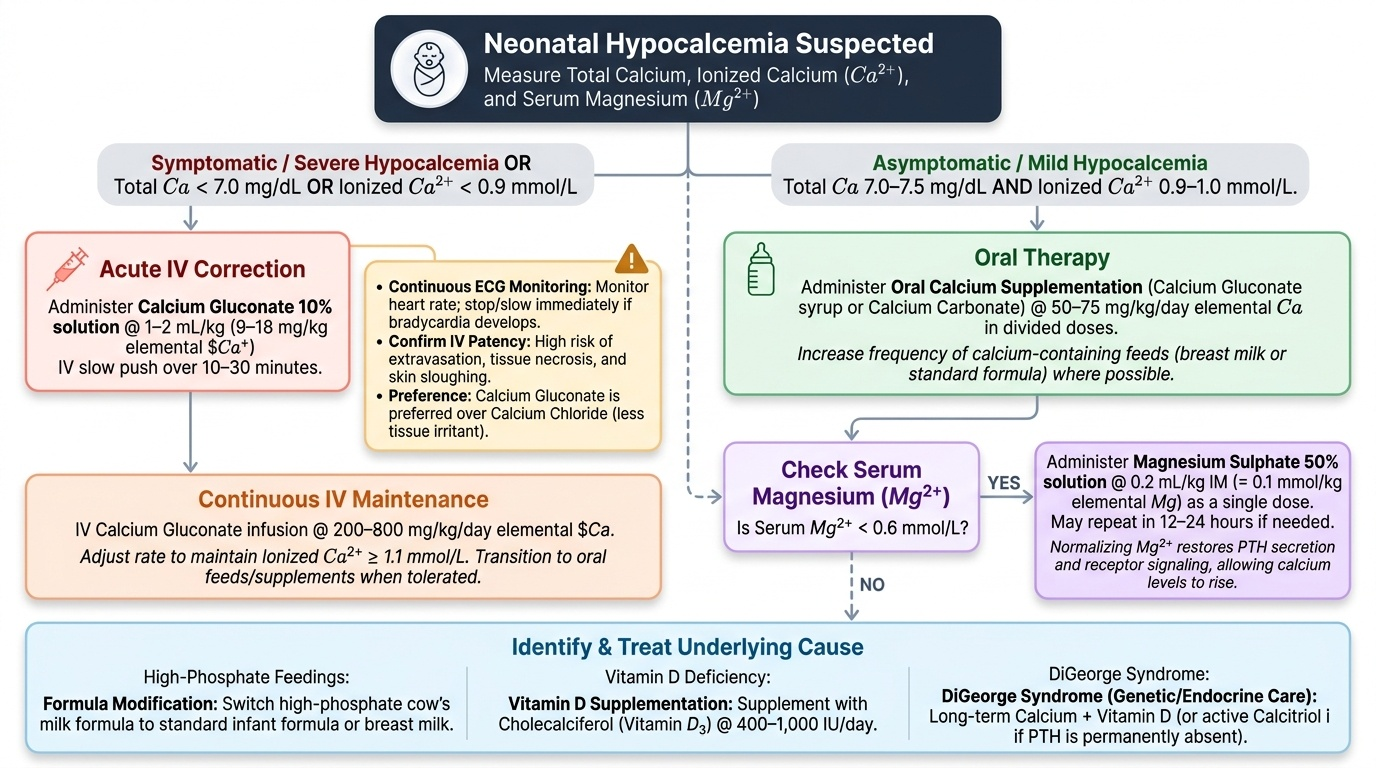
Symptomatic or severe hypocalcemia (total Ca <7.0 mg/dL or ionised Ca <0.9 mmol/L with symptoms):
Administer calcium gluconate 10% solution 1–2 mL/kg IV (providing approximately 9–18 mg/kg elemental calcium) as a slow push over 10–30 minutes with continuous ECG monitoring. The infusion must be through a patent, confirmed IV line — calcium gluconate extravasation causes severe tissue necrosis and skin sloughing. Monitor heart rate continuously; if bradycardia develops, slow or stop the infusion immediately. Calcium gluconate is preferred over calcium chloride in neonates because it is less irritant to veins and tissues. After the acute correction, continue with IV calcium gluconate as a maintenance infusion (200–800 mg/kg/day elemental calcium, adjusted to keep ionised Ca ≥1.1 mmol/L) until the neonate can tolerate oral feeds.
Asymptomatic or mild hypocalcemia (total Ca 7.0–7.5 mg/dL, ionised Ca 0.9–1.0 mmol/L, no symptoms):
Oral calcium supplementation (calcium gluconate syrup or calcium carbonate, providing 50–75 mg/kg/day elemental calcium in divided doses) is appropriate. Increase the frequency of calcium-containing feeds where possible.
Hypomagnesaemia correction is essential before or alongside calcium therapy. When serum magnesium is <0.6 mmol/L, PTH secretion and receptor signalling are impaired; hypocalcemia will not resolve until magnesium is normalised. Administer magnesium sulphate 50% solution 0.2 mL/kg IM (= 0.1 mmol/kg elemental Mg) as a single dose; repeat if needed at 12–24 hours. Once magnesium is corrected, PTH function is restored and calcium typically responds.
Treat the underlying cause: Switch high-phosphate cow's milk formula to standard infant formula or breast milk. For vitamin D deficiency: supplement with cholecalciferol (vitamin D₃) 400–1,000 IU/day. For DiGeorge syndrome: long-term calcium and vitamin D (or active calcitriol if PTH is permanently absent).
CLINICAL PEARL
Slow IV calcium gluconate — or bradycardia and cardiac arrest. The most dangerous error in managing symptomatic neonatal hypocalcemia is giving IV calcium gluconate as a rapid bolus. Calcium is a potent cardiac electrolyte: an acute rise in serum calcium shortens phase 2 of the cardiac action potential and can trigger severe bradycardia, heart block, or ventricular fibrillation. Always give calcium gluconate 10% at 1–2 mL/kg over a minimum of 10–30 minutes with the ECG trace running. A second critical point: never mix calcium gluconate with sodium bicarbonate in the same IV line — calcium carbonate precipitates immediately, blocking the cannula and delivering a clot rather than calcium. Flush thoroughly between drugs.
Self-Assessment
Work through these consolidation questions carefully. The answers require integration of pathophysiology, thresholds, and drug safety principles.
Q1. A 2-day-old preterm neonate (32 weeks) has ionised calcium of 0.88 mmol/L and is jittery. What is the diagnosis, the most likely mechanism, and the correct immediate treatment?
Answer: Early-onset neonatal hypocalcemia (onset <72 h, preterm). Mechanism: immature parathyroid gland + depleted calcium stores (third-trimester accretion incomplete) + elevated calcitonin. Treatment: calcium gluconate 10% 1–2 mL/kg IV over 10–30 minutes with ECG monitoring. Check serum magnesium simultaneously — correct hypomagnesaemia if present.
Q2. Why will hypocalcemia not respond to calcium therapy alone if serum magnesium is low?
Answer: Magnesium is an obligate cofactor for PTH secretion and for PTH receptor-signalling at target organs (bone, kidney). Hypomagnesaemia (<0.6 mmol/L) causes PTH-resistant hypocalcemia — the calcium given is not retained because the PTH axis needed to mobilise bone calcium and increase renal calcium reabsorption cannot function. Magnesium sulphate 0.2 mL/kg IM must be given first or concurrently.
Q3. A term neonate with DiGeorge syndrome has persistent hypocalcemia at 3 weeks of age. PTH is undetectable. What long-term management is needed?
Answer: DiGeorge syndrome with parathyroid aplasia causes permanent hypoparathyroidism. Management requires lifelong active vitamin D (calcitriol, to bypass the PTH-dependent 1α-hydroxylation step) plus oral calcium supplementation, with regular monitoring of serum calcium to avoid hypercalcaemia. Magnesium supplementation may also be needed.
Q4. What ECG change is the most useful non-invasive indicator of neonatal hypocalcemia, and what QTc cut-off is used?
Answer: Prolonged corrected QT interval (QTc); the cut-off is QTc >0.45 seconds. This reflects delayed ventricular repolarisation due to reduced calcium's effect on phase 2 of the action potential. QTc monitoring is also used to detect excessive calcium administration (shortening of QTc below 0.30 seconds signals hypercalcaemia).
SELF-CHECK
A neonate is being treated for symptomatic hypocalcemia. During IV calcium gluconate infusion, the heart rate drops from 140 to 85 beats/min. What is the correct immediate action?
A. Increase the infusion rate to rapidly normalise calcium
B. Stop or significantly slow the infusion immediately and reassess
C. Administer atropine and continue the infusion
D. Switch to calcium chloride at the same rate
Reveal Answer
Answer: B. Stop or significantly slow the infusion immediately and reassess
Bradycardia during IV calcium gluconate infusion indicates the rate is too fast — an acute rise in serum calcium shortens cardiac action potential phase 2 and can trigger bradycardia, heart block, or ventricular fibrillation. The correct action is to immediately slow or stop the infusion and monitor until heart rate recovers. ECG monitoring is mandatory throughout. Atropine does not address the cause. Increasing the rate would worsen the bradycardia. Calcium chloride is more concentrated and more cardiotoxic — not the solution here.