Page 5 of 53
PE19.2 | Neonatal Resuscitation — SDL Guide
Learning Objectives
- Identify the clinical indications and risk factors that anticipate the need for neonatal resuscitation
- Describe the anatomical and physiological principles underlying the neonatal resuscitation algorithm
- Perform the initial stabilisation steps of neonatal resuscitation (warm, position, dry, stimulate) within the golden minute
- Demonstrate correct bag-mask positive pressure ventilation (PPV) technique including rate, pressure, and MR SOPA corrective manoeuvres
- Describe the indications, technique, and compression-to-ventilation ratio for neonatal chest compressions
- State the dose and route of epinephrine in neonatal resuscitation
- Interpret heart rate response to guide decision-making at each step of the algorithm
- Participate in manikin-based simulation of the NRP/HBB algorithm
INSTRUCTIONS
Approximately 10% of newborns require some assistance to begin breathing at birth, and around 1% require extensive resuscitative measures. Given India's annual birth cohort of approximately 25 million, this translates to 250,000 neonates per year who may need active resuscitation — nearly all preventable deaths if resuscitation is performed correctly. The Helping Babies Breathe (HBB) programme, the WHO/AAP-designed adaptation of the Neonatal Resuscitation Program (NRP) for low-resource settings, has become India's primary training tool for skilled birth attendants. As a final-year medical student, you are expected to be able to perform neonatal resuscitation on a manikin (NMC competency PE19.2, skill level SH) and understand the evidence-based algorithm at every decision point. This module follows the PE-skills arc: indication → principles → technique → interpretation → applied practice.
References
- Ghai Essential Pediatrics, 9th ed., Ch 6 — Neonatal Resuscitation (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 122 — Respiratory Distress and Resuscitation of the Newborn (textbook)
- Helping Babies Breathe (HBB) 2nd edition — WHO/AAP, 2016 (guideline)
- ILCOR Neonatal Resuscitation Guidelines 2020 (Perlman et al.) (guideline)
- NNF India — Essential Newborn Care and Resuscitation Guidelines (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the junior resident on call in the labour room at 3 AM. A 28-year-old woman delivers at 38 weeks after a prolonged second stage and thick meconium-stained liquor. The baby is born limp, not crying, and centrally cyanosed. The nurse hands you the baby and says: 'Doctor, do something.' The attending obstetrician is managing a postpartum haemorrhage in the next bay. You have a resuscitation trolley in front of you: a radiant warmer, a self-inflating bag-mask (size 0/1), a stethoscope, and a clock. What do you do in the next 60 seconds — and in the next 10 minutes if the baby doesn't respond?
WHY THIS MATTERS
Birth asphyxia is one of the three leading causes of neonatal mortality in India, accounting for approximately 23% of all neonatal deaths according to the National Neonatal-Perinatal Database. Of all neonates who require active resuscitation, the vast majority respond to the initial steps and bag-mask ventilation alone — only a minority need chest compressions or medications. This means that competence in the first two steps of the algorithm saves more lives than knowing the epinephrine dose. The NMC competency PE19.2 is explicitly a skills competency at SH (skill, high priority) — meaning you will be assessed on your ability to perform this on a manikin, not merely describe it. Every minute of effective resuscitation that is delayed doubles the risk of death or permanent neurodevelopmental impairment. In a country where skilled birth attendance is still being scaled up, a newly-qualified doctor who can perform competent neonatal resuscitation is a literally life-saving asset at any level of the health system.
RECALL
Activate the following prior knowledge before proceeding. From the Normal Newborn Care SDL (pe11-normal-newborn): recall the APGAR score and its five parameters — particularly that heart rate is the single most important parameter for resuscitation decisions; a HR below 100 bpm at 1 minute is the key trigger for intervention. From Physiology (PY): recall the neonatal cardiovascular transition — at birth, pulmonary vascular resistance (PVR) falls and the fetal shunts (foramen ovale, ductus arteriosus) close; failure of this transition causes persistent fetal circulation. From your Anaesthesiology (AS) exposure: recall basic bag-mask ventilation technique for adults — but note that the neonatal technique differs in several critical ways (mask size, airway positioning, inspiratory pressure, and compression:ventilation ratio). Most importantly: the adult BLS compression-to-ventilation ratio is 30:2; the neonatal ratio is 3:1. Do not import the adult ratio into neonatal resuscitation.
When and Why Neonatal Resuscitation Is Needed
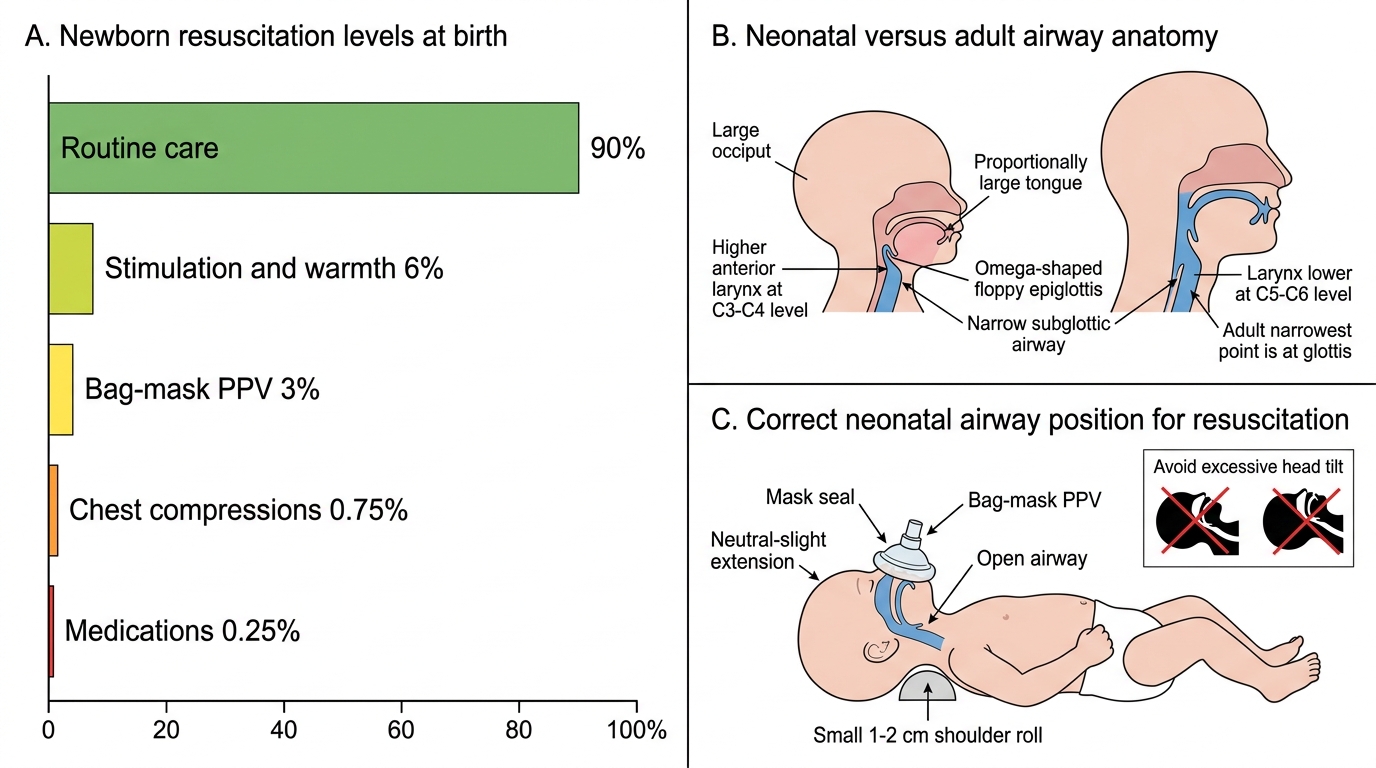
The transition from intrauterine to extrauterine life requires the newborn to achieve three physiological milestones within minutes of birth: clear the airways of fluid, expand the lungs and establish spontaneous breathing, and redirect circulation from placental to pulmonary gas exchange. In approximately 90% of deliveries, this transition occurs spontaneously without any assistance. However, in 10% of deliveries — roughly 2.5 million births per year in India — the neonate requires some level of assistance, ranging from simple stimulation and warming to full cardiopulmonary resuscitation.
Anticipating at-risk deliveries is the first competency in neonatal resuscitation. The decision to have a prepared resuscitation team and equipment at the bedside must be made before the baby is born, not after. The following antenatal, intrapartum, and neonatal risk factors increase the probability that resuscitation will be needed:
Antenatal risk factors: maternal diabetes, pre-eclampsia, chronic hypertension, anaemia, fetal growth restriction (IUGR), multiple gestation, polyhydramnios, oligohydramnios, fetal anomalies, and no antenatal care.
Intrapartum risk factors: emergency caesarean section, forceps or vacuum delivery, breech or abnormal presentation, prolonged labour, precipitate delivery, thick meconium-stained amniotic fluid (MSAF), abruptio placentae, placenta praevia, cord prolapse, and general anaesthesia.
Neonatal risk factors at delivery: prematurity (<37 weeks), multiple birth, fetal bradycardia, need for instrumented delivery.
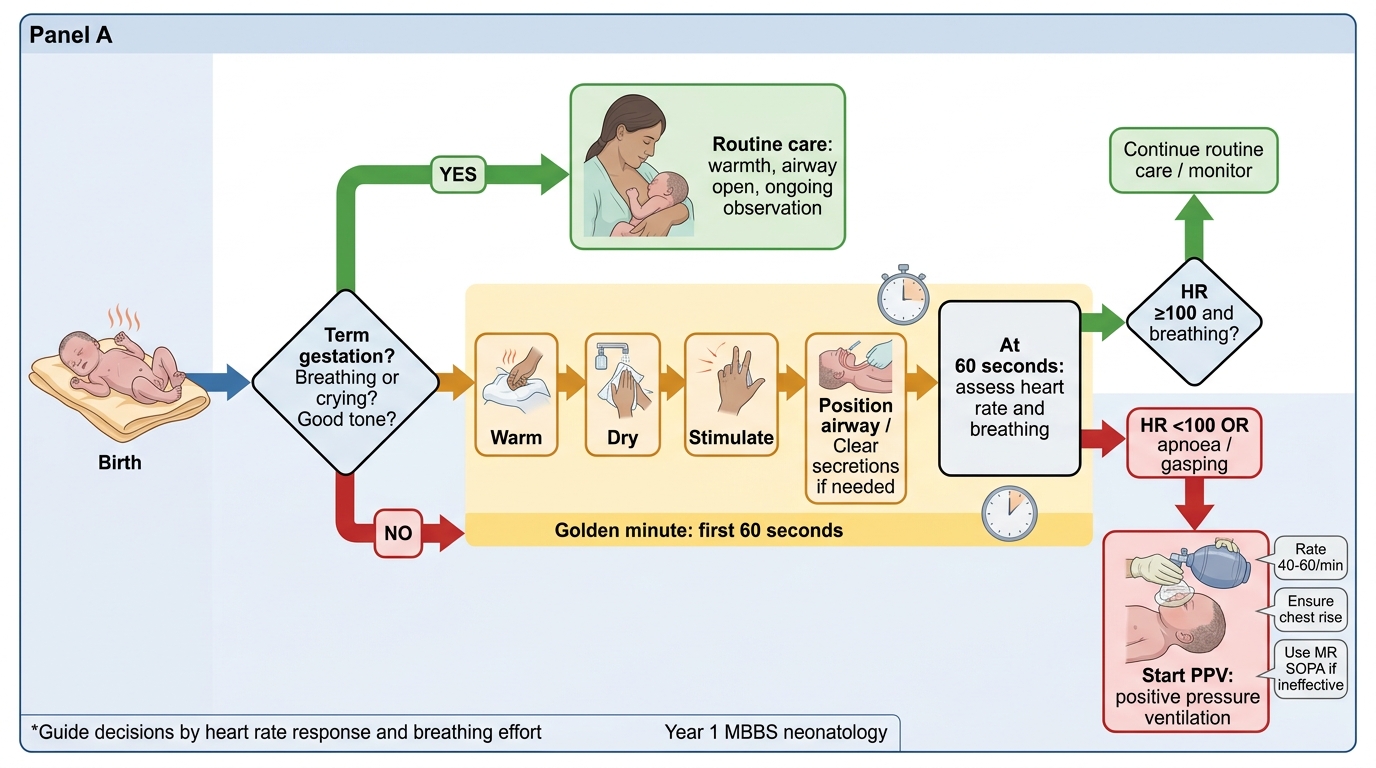
The golden minute concept, introduced by the Helping Babies Breathe (HBB) programme, defines the target window for completing initial stabilisation steps and making the critical decision about whether positive pressure ventilation is needed. Within 60 seconds of birth, the care team should have dried, warmed, and stimulated the baby, cleared the airway if necessary, and assessed whether the baby is breathing and has an adequate heart rate. A team that completes these steps within the golden minute gives the neonate its best chance of an uncomplicated transition.
Newborn Resuscitation Needs and Neonatal Airway Anatomy
Anatomy of the Neonatal Airway and Physiological Basis of Resuscitation
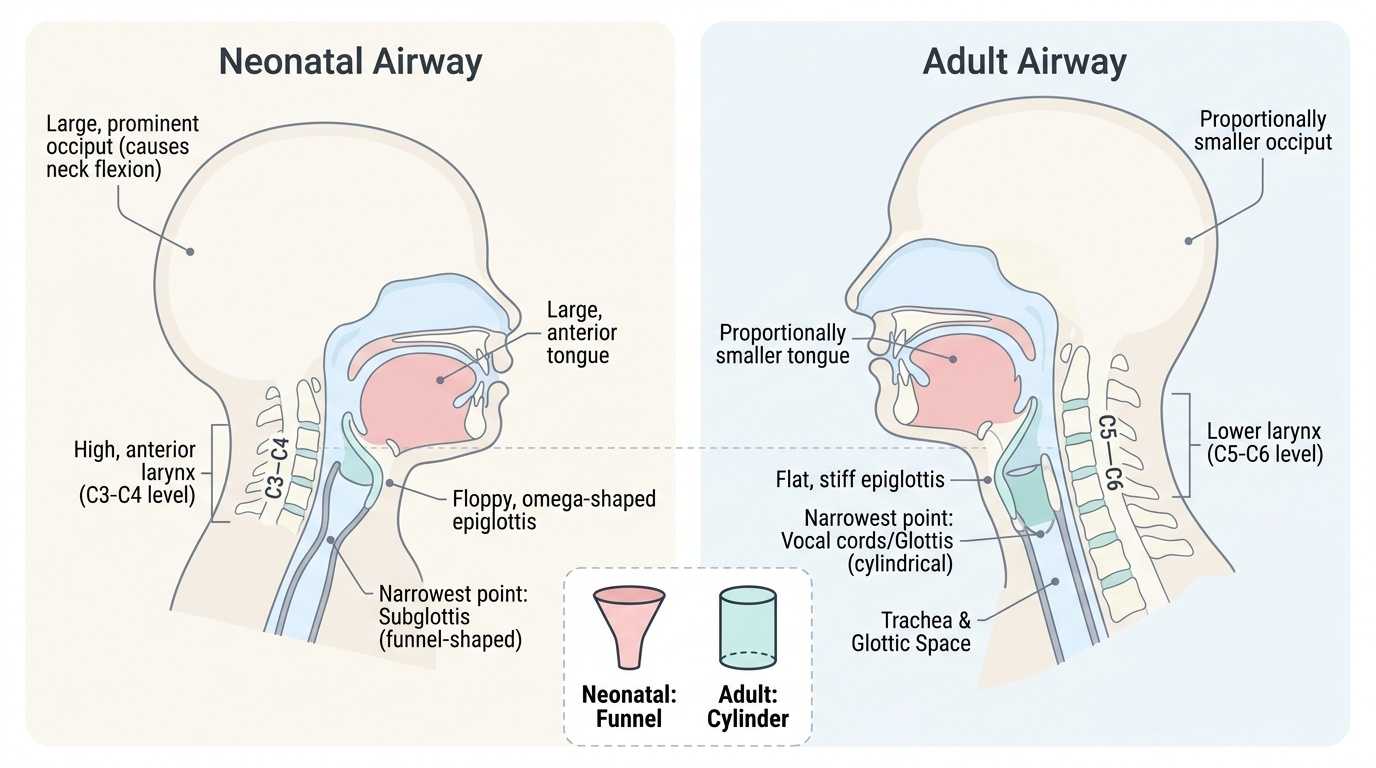
The neonatal airway differs from the adult airway in several anatomically important ways that directly determine resuscitation technique. A thorough understanding of these differences prevents the most common errors in neonatal bag-mask ventilation and intubation. The neonatal head is disproportionately large relative to the body, with a prominent occiput that causes the airway to flex into a sniffing position when the baby is laid flat — paradoxically obstructing the airway if the neck is not slightly extended. This is why correct positioning requires a small shoulder roll (1–2 cm folded cloth), not a large head tilt. The tongue is proportionally large and sits anteriorly, easily obstructing the oral airway. The larynx is positioned higher and more anteriorly (at C3–C4 in neonates vs C5–C6 in adults), and the epiglottis is omega-shaped and floppy. The subglottic space is the narrowest point of the neonatal airway (unlike adults, where the glottis is narrowest) — this is why uncuffed endotracheal tubes are used in neonates and why even minor subglottic oedema can critically reduce airway diameter.
Provided image
Physiology of perinatal asphyxia: When a neonate fails to establish adequate ventilation at birth, the sequence of physiological events follows a predictable pattern. Initially, primary apnoea occurs — the neonate stops breathing but has an adequate heart rate (>100 bpm) and responds to stimulation (drying, rubbing the back or soles). If hypoxia continues without intervention, the neonate enters gasping respirations followed by secondary apnoea — a state where the neonate will not respond to stimulation and heart rate falls progressively. Secondary apnoea requires positive pressure ventilation; stimulation alone is ineffective. Since it is clinically impossible to distinguish primary from secondary apnoea with certainty at the bedside, the NRP/HBB guideline states that any apnoeic neonate who does not respond to 30 seconds of stimulation should be treated as secondary apnoea and ventilation begun immediately.
Initial Stabilisation Steps — The Golden Minute
The initial stabilisation steps of neonatal resuscitation are performed in a specific sequence designed to maximise the chance of spontaneous transition while simultaneously preparing for intervention if needed. These steps are summarised by the mnemonic WIPE (Warm, position and clear airway, stimulate, evaluate) or equivalently by the HBB sequence: Warm → Dry → Stimulate → Position → Clear airway → Evaluate. Every step has a specific rationale grounded in neonatal physiology, and omitting any step increases the risk of harm.
Step 1 — Warm: Place the baby under a preheated radiant warmer immediately after birth. Evaporative cooling begins the instant the wet baby is exposed to room air, and even a brief period of hypothermia increases metabolic demand, oxygen consumption, and glucose utilisation. For preterm neonates <32 weeks, a polyethylene plastic wrap or bag is placed over the body (not the face) before drying to reduce evaporative and conductive heat loss. Target axillary temperature: 36.5–37.5°C.
Step 2 — Position and clear airway: Place the baby supine (or slightly tilted to one side) with the neck in a neutral or slightly extended 'sniffing' position — this aligns the oral, pharyngeal, and tracheal axes for optimal airflow. A 1–2 cm shoulder roll can help. Do NOT hyperextend the neck (narrows airway) and do NOT hyperlflex (obstructs). Clear the airway by suction only if the airway is visibly obstructed with secretions or meconium. Routine suctioning of the vigorous neonate is NOT recommended. For meconium-stained amniotic fluid (MSAF): if the baby is vigorous (crying, good tone, HR >100), do NOT intubate to suction — simply clear the mouth and nose with a bulb syringe if visibly obstructed, then proceed with initial steps. Routine intubation and tracheal suctioning in vigorous MSAF babies is no longer recommended (ILCOR 2015 onward) as it does not improve outcomes and risks harm.
Step 3 — Dry and stimulate: Vigorously dry the baby with a warm towel; this simultaneously provides stimulation and removes cooling moisture. If the baby does not breathe after drying, additional stimulation by rubbing the back or flicking the soles of the feet for 5–10 seconds is appropriate. Do not shake, slap, or forcibly stimulate the baby.
Evaluation at 60 seconds: After the initial steps, simultaneously assess two parameters: (1) Breathing — is the baby breathing adequately (regular respirations, not gasping)? (2) Heart rate — is the HR ≥100 bpm? These two assessments are made simultaneously by auscultating the chest with a stethoscope (most reliable) or feeling the umbilical cord. If the baby is breathing and HR ≥100, proceed to routine care (ongoing assessment, warmth, breastfeeding). If the baby is apnoeic OR HR <100, begin PPV.
NRP/HBB Neonatal Resuscitation Algorithm
SELF-CHECK
A neonate born at 38 weeks with thick meconium-stained liquor is crying vigorously and has good muscle tone. HR is 130 bpm. What is the correct immediate management?
A. Intubate immediately and suction the trachea
B. Perform routine initial steps; no tracheal suctioning required
C. Begin bag-mask ventilation at 40 breaths/min
D. Administer supplemental oxygen by face mask
Reveal Answer
Answer: B. Perform routine initial steps; no tracheal suctioning required
Per ILCOR 2015 and current NRP guidelines, routine intubation and tracheal suctioning is NOT recommended for vigorous meconium-stained neonates (crying, good tone, HR >100 bpm). It does not improve outcomes and may cause harm (bradycardia, airway injury). The correct approach is routine initial steps: warm, dry, stimulate, position — and clear the mouth and nose with a bulb syringe only if visibly obstructed. Bag-mask ventilation is not needed in a vigorous, breathing neonate.