Page 6 of 53
PE19.2 | Neonatal Resuscitation — SDL Guide (Part 2)
Positive Pressure Ventilation (PPV)
Positive pressure ventilation (PPV) is indicated when, after completing the initial steps within the golden minute, the neonate is: (a) not breathing or only gasping, OR (b) breathing but the heart rate is below 100 bpm. PPV is the single most effective intervention in neonatal resuscitation — the majority of neonates who require resuscitation respond to effective PPV alone without requiring chest compressions or medications. Competence in bag-mask ventilation is therefore the core skill of neonatal resuscitation.
Device: The self-inflating bag-and-mask is the standard device in most Indian delivery rooms. It consists of a self-inflating bag (250 mL for term neonates, 500 mL acceptable), a pressure-limiting pop-off valve (set at 30–40 cm H₂O to prevent barotrauma), and an oxygen inlet. In the absence of piped oxygen, room air (21% FiO₂) is the recommended starting gas for term and late preterm neonates ≥35 weeks; evidence shows that starting with 100% O₂ in term neonates increases oxidative stress without improving outcomes. For preterm neonates <35 weeks, starting FiO₂ of 21–30% with titration by pulse oximetry is recommended.
Mask size and seal: Select a mask that covers the nose and chin without covering the eyes. The most common error is an incorrect seal between the mask and face, which allows air to leak and prevents lung inflation. Use the E-C clamp technique: the thumb and index finger form a 'C' around the mask, while the remaining three fingers form an 'E' under the mandible, lifting the jaw into the mask without pressing on the soft tissue of the neck.
Ventilation rate and pressure: The target rate is 40–60 breaths per minute (count aloud: 'breathe — 2 — 3, breathe — 2 — 3'). The initial inflation pressure required to open a fluid-filled newborn lung is typically 20–25 cm H₂O for term neonates; up to 30–40 cm H₂O may be required for the first breath in a slow-to-breathe neonate. Subsequent breaths require less pressure once the lungs are inflated. Watch for chest rise as the primary indicator of effective ventilation — if the chest does not rise, the ventilation is ineffective.
MR SOPA corrective steps (when chest rise is absent — indicating ineffective PPV):
- M — Mask adjustment (reposition the mask for a better seal)
- R — Reposition the airway (neutral sniffing position; add shoulder roll)
- S — Suction (clear secretions from mouth and nose)
- O — Open the mouth slightly (jaw thrust)
- P — Pressure increase (increase PIP by 5–10 cm H₂O)
- A — Airway alternative (consider LMA or endotracheal intubation)
After 30 seconds of effective PPV (chest rising, rate 40–60/min), reassess the heart rate. If HR ≥100 and spontaneous breathing resumes: gradually wean and stop PPV. If HR 60–100: continue PPV, check effectiveness, recheck technique. If HR <60: begin chest compressions.
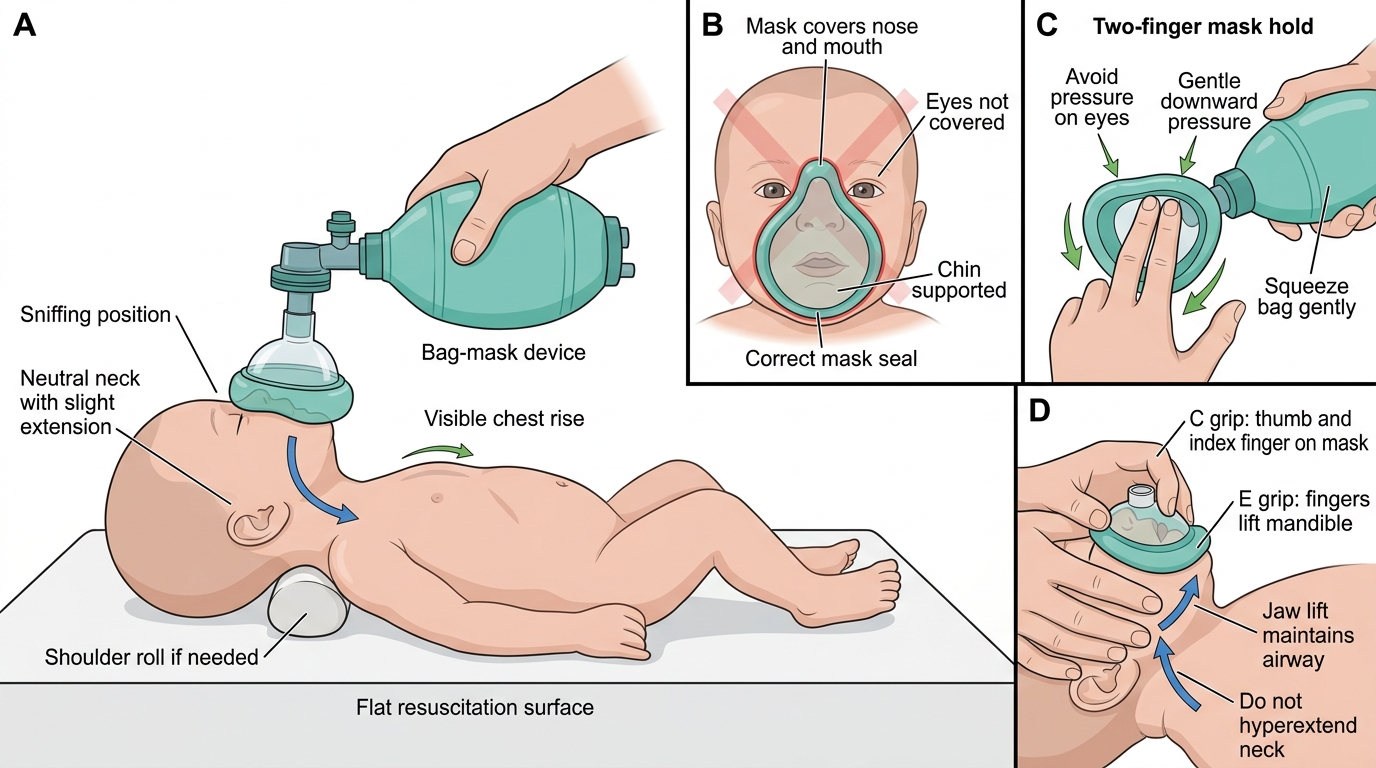
Correct Bag-Mask Ventilation Technique in a Neonate
Chest Compressions and Medications in Neonatal Resuscitation
Chest compressions in neonatal resuscitation are indicated when the heart rate remains below 60 bpm despite 30 seconds of effective positive pressure ventilation (i.e., ventilation with visible chest rise at the correct rate). The emphasis on 'effective' is critical: if PPV is not producing chest rise, compressions on a non-ventilated baby are futile. Always confirm effective ventilation before starting compressions, using MR SOPA corrective steps if necessary.
Technique — two-thumb encircling method (preferred): Two thumbs are placed side by side (or overlapping for very small neonates) on the lower third of the sternum, just below the nipple line. The hands encircle the thorax, with the fingers supporting the back. The sternum is compressed to a depth of one-third of the anterior-posterior (AP) chest diameter and then allowed to fully recoil before the next compression. This two-thumb encircling technique generates higher coronary perfusion pressure than the two-finger technique and is preferred when two rescuers are available.
Compression-to-ventilation ratio — the critical neonatal distinction: In neonates, the ratio is 3:1 — three compressions followed by one ventilation breath, giving a total of 90 compressions and 30 ventilations per minute (120 events/min). This ratio differs fundamentally from adult BLS (30:2) because neonatal cardiac arrest is almost always hypoxic in origin; the primary priority is restoration of oxygenation. A pneumonic for the count is: '1 and 2 and 3 and breathe' (each 'and' represents a brief pause). Once compressions are established, reassess the heart rate every 60 seconds.
Response thresholds during compressions: If HR rises to ≥60 bpm, discontinue compressions and continue PPV until HR reaches ≥100 bpm and spontaneous breathing is established.
Medications — epinephrine (adrenaline): If HR remains <60 bpm despite adequate CPR (effective ventilation + compressions for at least 60 seconds), administer epinephrine. The dose is:
- Intravenous (umbilical venous catheter — preferred route): 0.1–0.3 mL/kg of 1:10,000 solution (= 0.01–0.03 mg/kg)
- Endotracheal tube (only if IV access not yet established): 0.5–1.0 mL/kg of 1:10,000 solution (higher dose due to erratic ETT absorption)
Epinephrine acts by increasing systemic vascular resistance (alpha-adrenergic) and myocardial contractility/rate (beta-adrenergic), restoring coronary perfusion pressure. A dose of 1:1,000 solution at the same volume would be ten times the intended dose — always confirm the concentration (1:10,000) before drawing up.
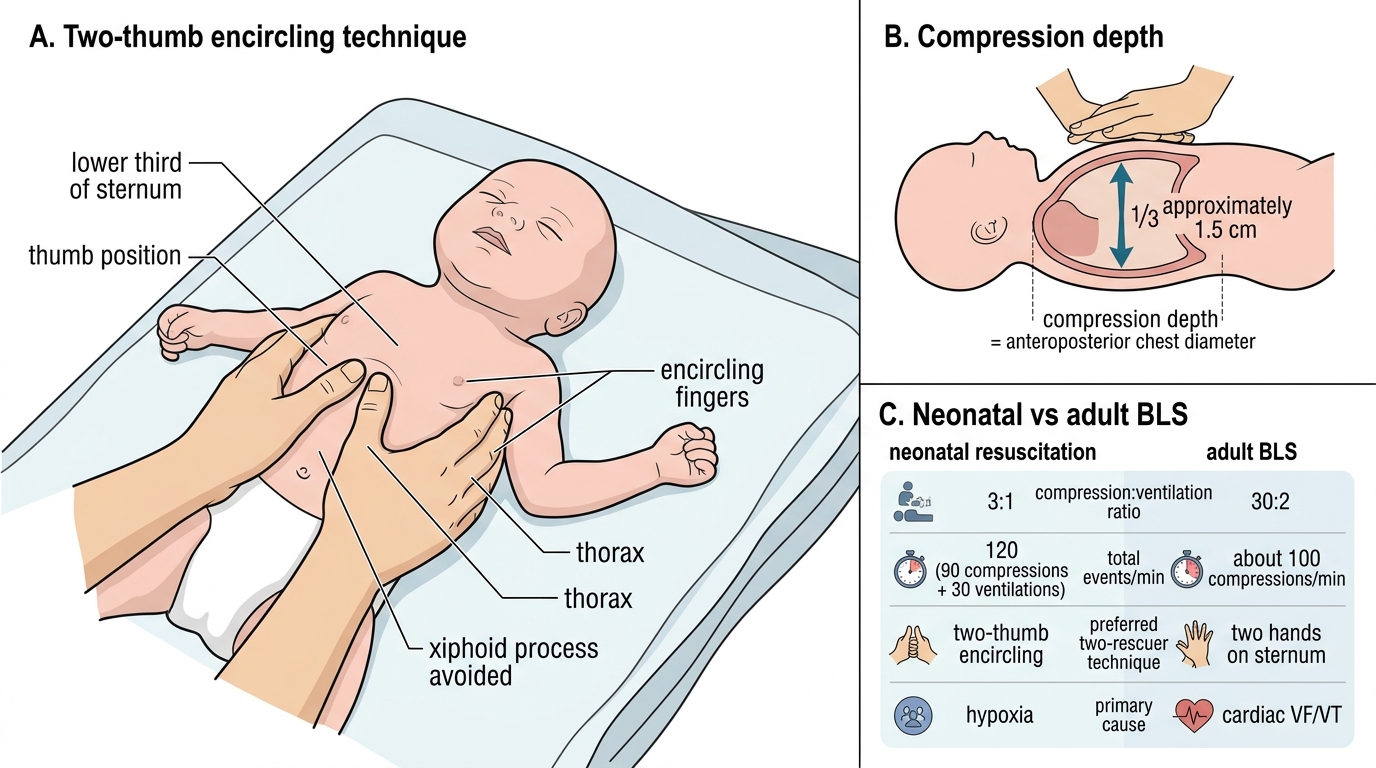
Two-Thumb Encircling Chest Compression in Neonatal Resuscitation
| Parameter | Neonatal resuscitation | Adult BLS |
|---|---|---|
| Compression:ventilation ratio | 3:1 | 30:2 |
| Total events/min | 120 (90 comp + 30 vent) | ~100 |
| Compression depth | 1/3 AP chest diameter (~1.5 cm) | 5–6 cm |
| Preferred 2-rescuer technique | Two-thumb encircling | 2 hands on sternum |
| Primary cause of arrest | Hypoxia | Cardiac (VF/VT) |
SELF-CHECK
After 30 seconds of effective PPV, a neonate's HR is 55 bpm. What is the next correct step?
A. Continue PPV alone for another 30 seconds
B. Administer epinephrine IV immediately
C. Begin chest compressions at a 3:1 compression-to-ventilation ratio
D. Discontinue resuscitation — this HR indicates poor prognosis
Reveal Answer
Answer: C. Begin chest compressions at a 3:1 compression-to-ventilation ratio
HR <60 bpm despite 30 seconds of effective PPV (confirmed by visible chest rise) is the threshold for beginning neonatal chest compressions. The ratio is 3:1 (three compressions followed by one ventilation), giving 90 compressions and 30 ventilations per minute. Epinephrine is reserved for HR <60 despite adequate combined CPR (compressions + ventilation) for at least 60 seconds. Continuing PPV alone is insufficient when HR is below 60. Discontinuation is inappropriate at this early stage.
Interpreting Response to Resuscitation
Heart rate is the primary and most sensitive indicator of the neonate's response to resuscitation. It should be monitored at every decision point in the algorithm, and the response to each intervention determines whether to advance, maintain, or step down. The heart rate is best assessed by cardiac auscultation with a stethoscope; pulse oximetry provides continuous monitoring but may be unreliable in the first minutes due to peripheral vasoconstriction. Counting the heart rate for 6 seconds and multiplying by 10 gives a rapid approximation. The fundamental principle underpinning this interpretation framework is that neonatal cardiac arrest is almost universally hypoxic in aetiology — unlike adult cardiac arrest where arrhythmia predominates. This means that restoring adequate oxygenation and ventilation is the primary therapeutic intervention, and that every HR threshold in the algorithm represents a specific level of cardiorespiratory compromise that corresponds to a specific therapeutic escalation. A team that understands these thresholds mechanistically — rather than as a memorised list — will make correct decisions more reliably under the stress of a real resuscitation, and will also recognise when a baby is improving (HR rising) or deteriorating (HR falling despite intervention) in real time.
Decision tree by HR response:
- HR ≥100 bpm + spontaneous breathing established: Step down. Discontinue PPV, continue observation, initiate skin-to-skin and early breastfeeding. If the 5-minute APGAR is ≥7, proceed to routine postnatal care.
- HR ≥100 bpm but breathing irregular or absent: Continue PPV. Check for any residual airway obstruction. Consider CPAP for a spontaneously breathing preterm neonate who has respiratory distress (pressure 5–8 cm H₂O).
- HR 60–100 bpm: Continue PPV; verify effectiveness (chest rise); apply MR SOPA if not rising; reassess in 30 seconds.
- HR <60 bpm after 30 s effective PPV: Add chest compressions (3:1 ratio).
- HR <60 bpm despite CPR for 60 s: Administer epinephrine; ensure ventilation is truly effective (consider intubation); exclude correctable causes (tension pneumothorax, hypovolaemia, severe metabolic acidosis).
- HR = 0 (asystole) despite full CPR for 10 minutes: In a term neonate with no response to full resuscitation for 10 minutes, consider discontinuation in discussion with family and the senior team. This is a rare and ethically complex scenario.
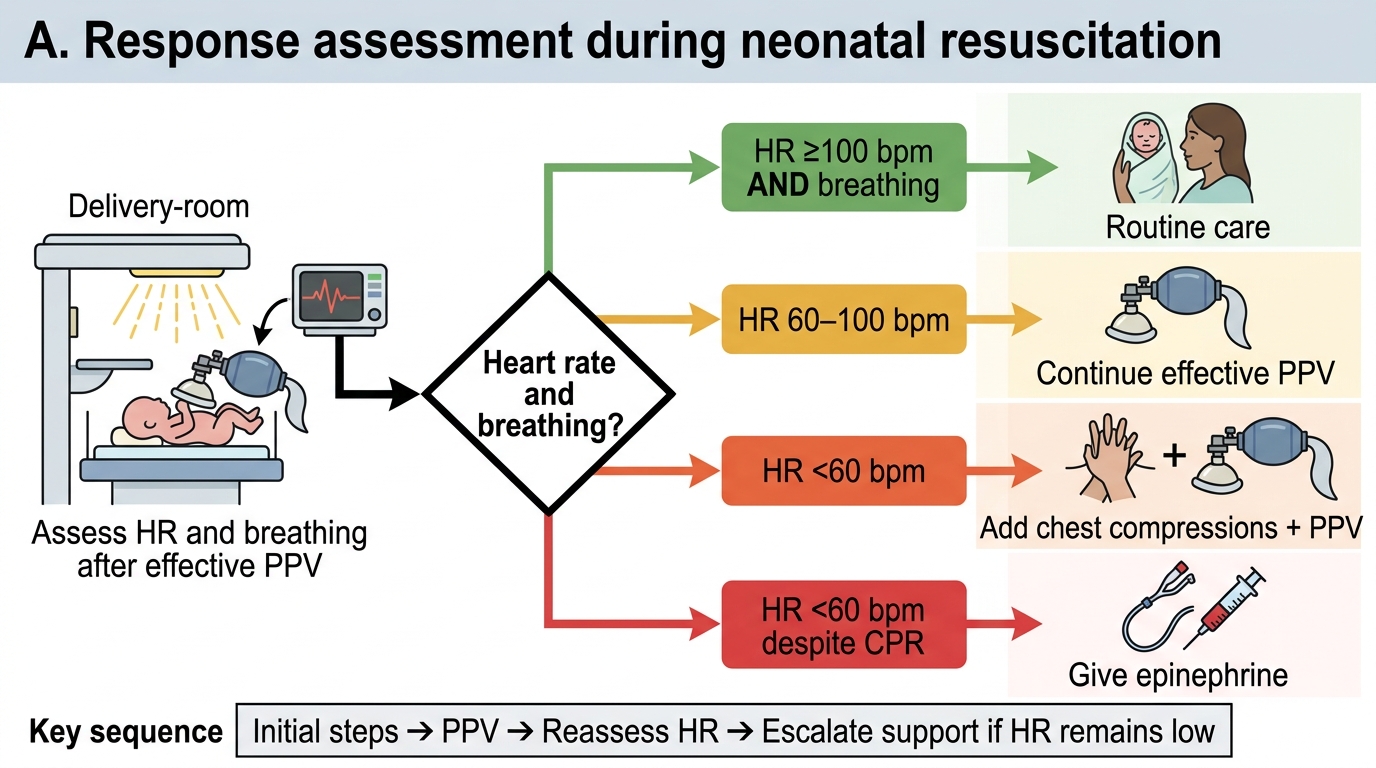
Neonatal Resuscitation Response Assessment Decision Tree
CLINICAL PEARL
The single most common reason neonatal PPV fails to raise the heart rate is an inadequate mask seal causing air leak — not an intrinsically non-resuscitable baby. Before escalating to chest compressions or intubation, always apply MR SOPA corrective steps. In one study of newborn resuscitation, corrective ventilation steps resolved the problem and avoided intubation in over 60% of cases where initial PPV appeared ineffective. The corollary: never start chest compressions on an apnoeic neonate without first confirming that the chest is rising with each breath. Compressions on an unventilated neonate circulate deoxygenated blood — a physiologically futile intervention. The mantra: 'Ventilate first, compress only on a ventilated neonate.'