Page 24 of 53
PE19.9 | Neonatal Thermal Care — SDL Guide
Learning Objectives
- Describe the physiological reasons why neonates are at high risk of hypothermia
- Classify neonatal hypothermia into mild, moderate, and severe grades with their clinical features
- Explain the metabolic cascade triggered by cold stress in a neonate
- Implement the WHO Warm Chain at birth and outline rewarming strategies by hypothermia severity
- Distinguish neonatal hypothermia from hyperthermia and identify when fever requires urgent evaluation
INSTRUCTIONS
Neonatal hypothermia is the silent epidemic of newborn care. In low-resource settings, 30–85% of neonates arrive hypothermic to neonatal units, and hypothermia on admission independently predicts neonatal mortality. The tragedy is that hypothermia is almost entirely preventable with simple, zero-cost interventions — drying the baby at birth, initiating skin-to-skin contact, delaying the first bath, keeping the delivery room warm. The WHO Warm Chain codifies these actions. Understanding the physiology of neonatal heat loss and the metabolic cascade of cold stress transforms these seemingly obvious interventions from rote practice into defensible clinical decisions.
References
- Ghai Essential Pediatrics, 9th ed., Ch 8 — Newborn Infant: Temperature Regulation (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 105 — Thermoregulation in the Newborn (textbook)
- WHO Thermal Protection of the Newborn: A Practical Guide (1997); IAP NNF Guidelines on Thermal Care (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A community health worker calls you from a rural sub-centre. A woman just delivered a 2.8 kg baby at home in the winter. The birth attendant wiped the baby, placed it naked in a basket, and went to attend to the mother. Twenty minutes later, the community health worker arrived and found the baby quiet, not feeding, with bluish extremities and a temperature of 35.2°C by axillary thermometer. She asks: 'What do I do?' This scenario — moderate hypothermia in a term neonate after a delayed thermal response at birth — is preventable with the Warm Chain and is treatable with skin-to-skin rewarming. Your ability to guide this worker through the correct steps will determine whether this baby survives.
WHY THIS MATTERS
Temperature regulation is one of the most basic functions of a healthy neonate, yet it is also one of the most easily disrupted — particularly in the first hours after birth and in low-weight or sick neonates. WHO global data show that hypothermia at birth (temperature <36.5°C) affects 30–85% of neonates in low-income settings and is independently associated with increased mortality and morbidity. In India, where a substantial proportion of deliveries occur in non-facility settings or in facilities without heated neonatal spaces, hypothermia is a genuine public health emergency. The consequences of untreated hypothermia extend beyond thermal discomfort: cold stress triggers hypoglycaemia, metabolic acidosis, pulmonary vasoconstriction, and hypoxia — each of which further impairs the neonate's ability to rewarm. The Warm Chain addresses this problem with interventions that cost essentially nothing.
RECALL
From physiology, recall that the hypothalamus is the thermoregulatory centre — it detects core body temperature via thermoreceptors and activates heat production or heat loss responses to maintain normothermia. In adults, cold exposure triggers: (1) shivering (skeletal muscle contractions generating heat) and (2) non-shivering thermogenesis via brown adipose tissue (BAT). From biochemistry, recall that brown fat (found in the neck, axillae, around the adrenals, and interscapular in neonates) contains UCP1 (uncoupling protein 1/thermogenin) in the inner mitochondrial membrane, which uncouples oxidative phosphorylation from ATP synthesis — energy is released as heat rather than ATP. This is the primary heat production mechanism in neonates because — importantly — neonates cannot shiver effectively (immature skeletal muscle coordination). Finally, recall from your newborn basics that neonatal blood volume is ~80–90 mL/kg, making haemodynamic effects of cold-induced vasoconstriction significant.
Clinical Presentation: Recognising Cold and Hot Neonates
Neonatal hypothermia is clinically insidious — unlike the adult who shivers and complains of cold, the hypothermic neonate presents with non-specific signs that are easily attributed to other causes such as sepsis, hypoglycaemia, or birth asphyxia. The clinical recognition of hypothermia requires systematic temperature measurement at every neonatal assessment, combined with vigilance for its secondary consequences and an understanding of which neonates are highest risk. The importance of measuring temperature at every opportunity cannot be overstated: studies in Indian neonatal units show that more than half of hypothermic neonates had their temperature not measured at admission. A normal temperature does not exclude cold stress — the neonate may be actively compensating, with cool extremities but a maintained core temperature. The combination of clinical signs, risk factors, and sequential temperature measurement provides the complete diagnostic picture.
Clinical signs of hypothermia (in approximate order of appearance as temperature falls):
- Poor feeding and lethargy: cold stress reduces gut motility and feeding drive; a neonate who was feeding adequately and is now refusing feeds should prompt a temperature check
- Cold peripheries: extremities feel cold before core temperature falls; central warming with cool peripheries = early cold stress
- Skin mottling or pallor: peripheral vasoconstriction redistributes blood flow centrally; skin appears pale or mottled
- Weak cry, hypotonia: neuromuscular function is temperature-dependent; moderate hypothermia causes generalised hypotonia
- Bradycardia and apnoea: cardiac and respiratory function are temperature-dependent; moderate hypothermia slows conduction, severe hypothermia causes life-threatening bradycardia and apnoeic spells
- Hypoglycaemia: cold-stressed neonates have elevated metabolic demands (futile thermogenesis depletes glucose rapidly); blood glucose must always be checked in a hypothermic neonate
- Metabolic acidosis: tissue hypoxia from peripheral vasoconstriction and increased oxygen consumption generates lactic acid
- Sclerema neonatorum (severe hypothermia): skin and subcutaneous tissue become hardened and wooden — a pre-terminal sign in severe hypothermia, especially in preterm or sick neonates
At-risk groups for hypothermia:
- Preterm and LBW neonates: minimal subcutaneous fat, thin skin, immature BAT activity, large surface-area-to-volume ratio — the most vulnerable group
- Birth asphyxia and sick neonates: reduced metabolic capacity, unable to mount thermogenic response
- Neonates in low-resource settings: cold delivery rooms, wet baby not dried immediately, delayed skin-to-skin
- Winter deliveries in India: environmental temperature <25°C compounds heat loss
Neonatal hyperthermia (temperature >37.5°C axillary) is less common but equally important. Causes include:
- Environmental overheating (most common in term healthy neonates): overwarmed incubator or radiant warmer, excess clothing, hot environment — baby is warm-to-touch overall, not irritable, settles with cooling
- True fever (infectious): temperature driven by endogenous pyrogens (IL-1, IL-6, TNF-α, prostaglandins); neonate may appear unwell, irritable, has other signs of sepsis
- Dehydration fever (neonatal): inadequate breastfeeding in the first days → hypernatraemic dehydration → fever; associated with weight loss >10%, sunken fontanelle, dry mucous membranes
Critical clinical point: any temperature elevation in a neonate <28 days should prompt a full sepsis evaluation (CBC, CRP, blood culture, LP) unless environmental overheating is clearly established, because neonates respond to infection with both fever AND hypothermia — temperature instability of any direction is a danger sign.
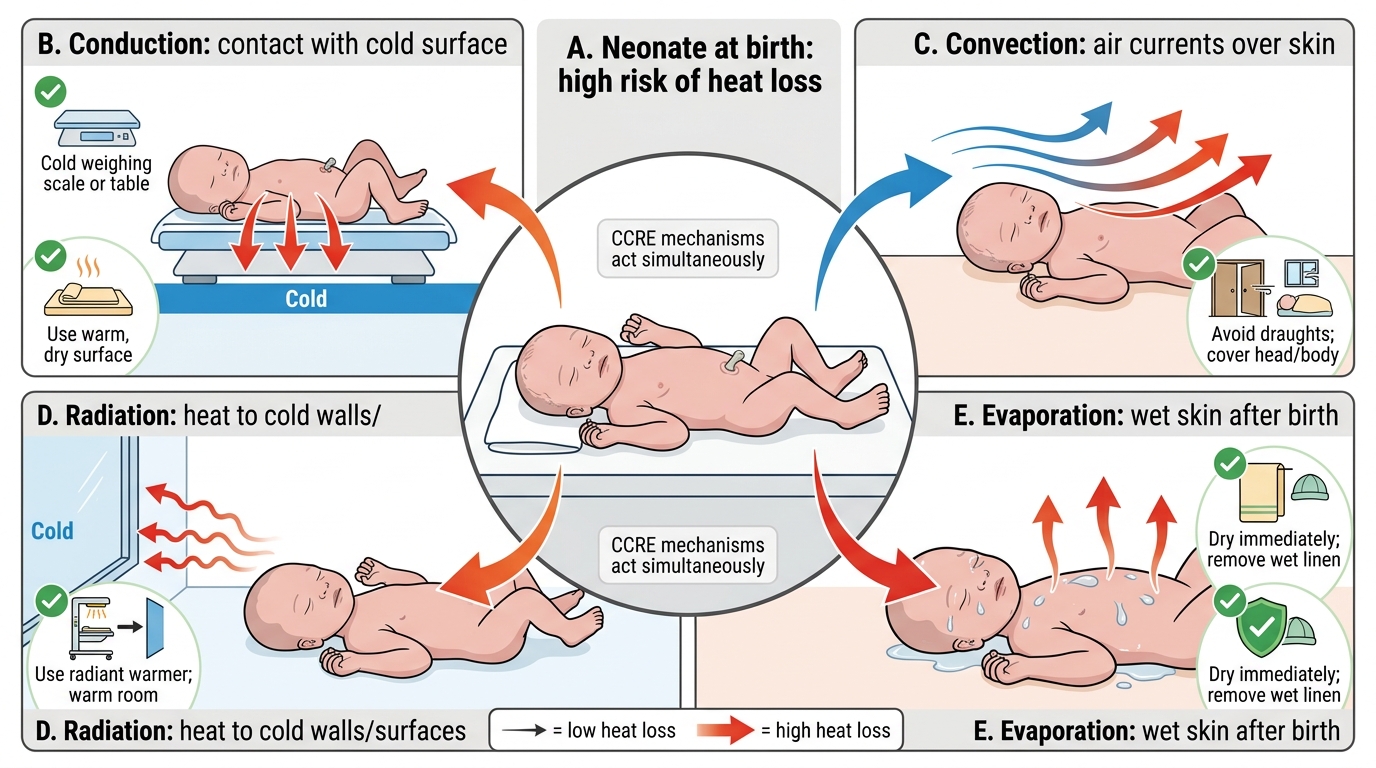
Four Mechanisms of Neonatal Heat Loss
Physiology: Why Neonates Lose Heat So Easily
The remarkable thermal vulnerability of the neonate results from the intersection of physical characteristics (thin skin, large surface-area-to-body-volume ratio, minimal subcutaneous insulation) and physiological immaturity (immature hypothalamic thermoregulation, limited thermogenic capacity). Understanding these mechanisms converts the Warm Chain from a list of rules into a set of physiology-driven decisions. Unlike older children and adults who can compensate through shivering, sweating, and behavioural adaptations, the neonate has no behavioural option, limited thermogenic reserve, and a surface area that geometrically amplifies heat exchange with the environment. Each of the four heat loss mechanisms operates simultaneously and additively at birth — a wet, naked neonate in a cold draughty room is losing heat through all four channels at once, and the cumulative rate can exceed the neonate's maximum thermogenic capacity within minutes. This physiological reality is why the delivery room and the first hour after birth are the highest-risk period for neonatal hypothermia.
Four mechanisms of heat loss — mnemonic CCRE:
1. Conduction: heat transfers from the warm neonate to a cooler surface in direct contact (cold metal weighing scale, cold examination table, cold mattress). Prevention: place neonate on a warm pre-heated surface or a blanket.
2. Convection: moving air currents carry heat away from the skin surface. The neonate's large surface area amplifies this loss. Prevention: close windows, eliminate drafts in the delivery room, cover the neonate.
3. Radiation: the neonate radiates heat to any cool surface in the environment (cold walls, cold incubator walls) without direct contact — this is often overlooked. Prevention: warm the environment to ≥25°C; incubator walls should not be cold.
4. Evaporation: evaporation of amniotic fluid from wet skin at birth is the largest single mechanism of heat loss in the immediate post-delivery period. A wet neonate on a cold surface can lose body heat alarmingly fast. Prevention: immediate drying with a warm towel is the single most important Warm Chain action.
Why neonates are particularly vulnerable compared to adults:
- Surface area:volume ratio: a neonate has approximately 3× the surface area per kilogram of body weight compared to an adult. This geometrically amplifies convective and radiant losses.
- Thin skin: minimal subcutaneous fat, especially in preterm neonates — provides negligible insulation.
- Immature hypothalamic thermoregulation: the hypothalamic temperature set-point and effector responses are not fully mature at birth; the neonate is slow to detect and respond to thermal challenges.
- Cannot shiver: neonates lack effective shivering — their main thermogenic defence is non-shivering thermogenesis (NST) via brown adipose tissue (BAT). BAT is present in the neck, interscapular region, axillae, mediastinum, and perinephric areas. Catecholamines released in response to cold stimulate beta-3 adrenergic receptors on brown adipocytes → activate hormone-sensitive lipase → free fatty acids → mitochondrial oxidation → heat generated via UCP1 (thermogenin) uncoupling. However, BAT stores are limited (especially in preterm neonates), and NST rapidly depletes glucose and oxygen — explaining why hypoglycaemia and oxygen desaturation follow cold stress.
Thermoneutral zone: the environmental temperature range in which the neonate maintains normal body temperature with minimal metabolic energy expenditure. For a term neonate: approximately 32–34°C in an open incubator; for a preterm neonate: higher (35–37°C). Managing the thermal environment within the thermoneutral zone minimises the metabolic cost of thermoregulation.
SELF-CHECK
A healthy term neonate is placed unwrapped on a cool metal examination table immediately after birth. Which mechanism of heat loss is MOST responsible for the rapid initial temperature drop in this scenario?
A. Radiation — heat radiated from skin to cool walls in the room
B. Evaporation — amniotic fluid on wet skin evaporating rapidly
C. Conduction — direct heat transfer from the warm neonate to the cool metal surface
D. Convection — air currents removing heat from the skin surface
Reveal Answer
Answer: B. Evaporation — amniotic fluid on wet skin evaporating rapidly
Evaporation of amniotic fluid from the wet skin surface at birth is the LARGEST single mechanism of heat loss in the immediate post-delivery period. A wet neonate loses heat through evaporation far faster than through other mechanisms in the first minutes. This is why IMMEDIATE DRYING is the first and most important Warm Chain step. While conduction from a cold metal table is also significant and should be prevented (pre-warm the surface), evaporation on a wet neonate is the quantitatively dominant initial mechanism.
Pathophysiology of Hypothermia: The Metabolic Cascade
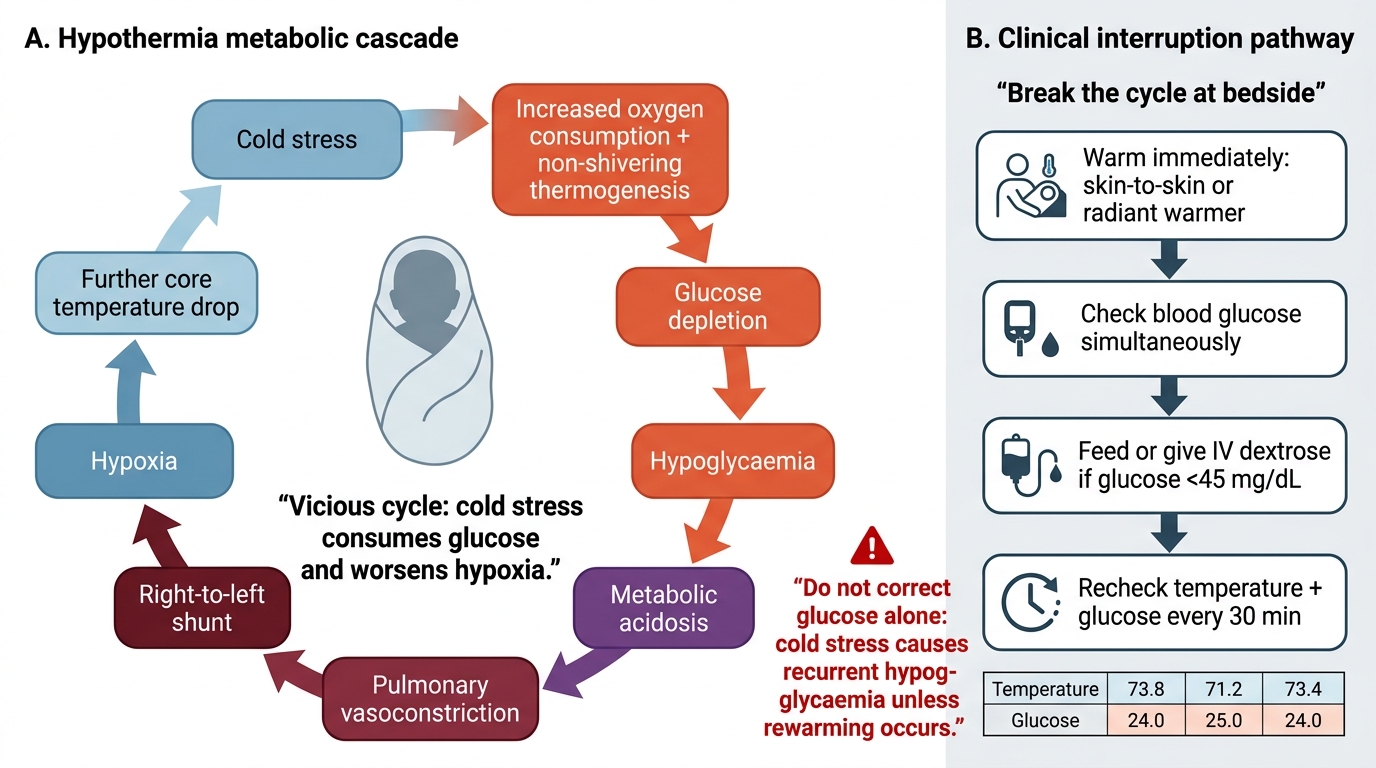
Once a neonate's temperature begins to fall, a self-reinforcing metabolic cascade is initiated that can rapidly progress from mild hypothermia to a life-threatening spiral if not interrupted. Understanding each step of this cascade explains why hypothermia is dangerous beyond the temperature itself, and why rewarming alone — without monitoring and correcting the metabolic consequences — is insufficient management. The cascade should be understood as a sequence of physiological adaptations that initially protect the neonate (vasoconstriction preserving core temperature, BAT activation attempting to generate heat) but rapidly become pathological as metabolic reserves are exhausted. Each severity grade of hypothermia corresponds not just to a temperature number but to a predictable metabolic state — mild hypothermia is compensated adaptation, moderate is decompensating with active metabolic consequences, and severe is a systemic emergency involving failure of multiple organ systems.
The cascade begins with cold stress (temperature <36.5°C or even anticipatory exposure to a cold environment before temperature falls). The hypothalamus activates thermogenic responses:
- Increased metabolic rate and oxygen consumption: non-shivering thermogenesis (BAT activation) dramatically increases whole-body oxygen consumption. In a preterm neonate, oxygen consumption may increase 2–3 times baseline during cold stress — rapidly exceeding the capacity of the immature cardiorespiratory system.
- Glucose depletion → hypoglycaemia: BAT thermogenesis is fuelled primarily by free fatty acids and glucose. In neonates with limited glycogen stores (especially SGA/IUGR and preterm), cold stress rapidly depletes blood glucose. Hypoglycaemia (blood glucose <45 mg/dL) is a direct metabolic consequence of hypothermia — always check blood glucose in any hypothermic neonate.
- Metabolic acidosis: increased oxygen consumption with inadequate oxygen delivery (due to peripheral vasoconstriction and immature cardiac output) → anaerobic glycolysis → lactic acid accumulation → metabolic acidosis. Acidosis further impairs cardiac function and cellular metabolism.
- Pulmonary vasoconstriction: hypoxia and acidosis are potent stimuli for pulmonary vasoconstriction. In a neonate, pulmonary hypertension can cause persistent fetal circulation (right-to-left shunting through the ductus arteriosus and foramen ovale) → further hypoxia → worsening vasoconstriction → a vicious cycle.
- Peripheral vasoconstriction → reduced heat exchange: as the neonate attempts to conserve core temperature, peripheral blood vessels constrict, reducing blood flow to the extremities. The extremities lose heat rapidly (appearing cold and mottled) while core temperature is maintained initially — this is the 'cold peripheries with warm trunk' pattern of early hypothermia, which then progresses to central cooling as thermogenic reserves are exhausted.
- Capillary leak and coagulopathy (severe hypothermia): endothelial damage from prolonged hypoxia and acidosis leads to capillary leak and consumptive coagulopathy, particularly in preterm neonates with already fragile endothelium — contributing to IVH and pulmonary haemorrhage.
The clinical take-away: hypothermia is not a single problem — it is a trigger for a cascade of metabolic crises. Treating the temperature alone without monitoring blood glucose, oxygen saturation, and acid-base status is incomplete management.
Neonatal Hypothermia Metabolic Cascade
CLINICAL PEARL
The most commonly missed connection in neonatal thermal care is that hypothermia causes hypoglycaemia — not the other way around. A hypothermic neonate with hypoglycaemia requires BOTH rewarming AND glucose correction; correcting the blood glucose alone without addressing the thermal state will result in recurrent hypoglycaemia because cold stress continues to consume glucose. The bedside sequence should be: (1) warm immediately (skin-to-skin or radiant warmer); (2) check blood glucose simultaneously; (3) initiate feeds (or IV dextrose if glucose <45 mg/dL); (4) recheck both temperature and glucose every 30 minutes during rewarming. Documenting temperature-glucose pairs is a reliable way to track recovery in a hypothermic neonate.