Page 25 of 53
PE19.9 | Neonatal Thermal Care — SDL Guide (Part 2)
Diagnosis: Measuring and Grading Neonatal Temperature
Accurate temperature measurement is the foundation of neonatal thermal care. In clinical practice, temperature measurement must be performed at every routine neonatal assessment and repeatedly during any illness — because temperature instability (both hypothermia and hyperthermia) is a non-specific sign of a wide range of neonatal conditions including sepsis, metabolic disorders, and hypoxic-ischaemic encephalopathy, as well as environmental thermal mismanagement.
Method and measurement site:
The axillary temperature (measured with a mercury or digital thermometer in the axilla for 3 minutes, with the arm held close to the body) is the WHO-recommended site for routine neonatal temperature measurement. Rectal temperature is more accurate for core temperature but carries a risk of rectal perforation in neonates and is reserved for clinical necessity. Skin temperature and forehead strip thermometers are unreliable for grading hypothermia.
Grading of hypothermia (WHO classification):
- Normal: 36.5–37.5°C axillary — no intervention beyond maintaining warmth
- Mild hypothermia (cold stress): 36.0–36.4°C — extra clothing, skin-to-skin contact, breastfeeding; monitor closely
- Moderate hypothermia: 32.0–35.9°C — active rewarming (skin-to-skin/KMC for stable neonates; radiant warmer for sick/preterm); blood glucose monitoring; IV dextrose if hypoglycaemic; monitor cardiorespiratory status
- Severe hypothermia: <32.0°C — emergency: radiant warmer + servo control + IV access + blood glucose + blood gases + treatment of complications (IVH, pulmonary haemorrhage, coagulopathy); consider underlying illness
Clinical features that track with grade:
Mild: quiet, reduced activity, poor feeding. Moderate: bradycardia, hypotonia, apnoea, mottled skin, metabolic acidosis, hypoglycaemia. Severe: weak or absent cry, very low muscle tone, bradycardia, cyanosis, sclerema neonatorum.
The key differentials in a neonate with temperature instability include:
- Sepsis: fever or hypothermia + toxic appearance + lethargy + poor perfusion; cannot be distinguished from environmental hypothermia on temperature alone — all hypothermic neonates without a clear thermal explanation require sepsis screen
- Hypoxic-ischaemic encephalopathy (HIE): temperature instability in post-asphyxia period; therapeutic hypothermia (33–34°C) is used therapeutically for moderate-severe HIE — this is a different clinical context
- Endocrine causes (hypopituitarism, hypothyroidism): rare, temperature instability is one of many signs
The rewarming rate for moderate hypothermia should be approximately 0.5°C per hour — avoid rapid rewarming (above 1°C/hour) because overshoot hyperthermia and sudden vasodilation can cause cardiovascular instability. For skin-to-skin rewarming, the rate is naturally gradual and self-regulating.
SELF-CHECK
A 3-day-old term neonate has an axillary temperature of 34.8°C, is hypotonic, and has a blood glucose of 38 mg/dL. The delivery room was cold (18°C) and the neonate was not dried immediately after birth. What is the FIRST action?
A. Administer IV 10% dextrose at 80 mL/kg/day
B. Begin a full sepsis workup (CBC, CRP, blood culture, LP)
C. Place on a radiant warmer, initiate skin-to-skin rewarming, and check blood glucose
D. Administer IM glucagon 0.1 mg/kg for hypoglycaemia
Reveal Answer
Answer: C. Place on a radiant warmer, initiate skin-to-skin rewarming, and check blood glucose
This is moderate hypothermia (34.8°C) with associated hypoglycaemia — the classic thermal cascade. The FIRST action is to provide active rewarming: radiant warmer or skin-to-skin with the mother. Simultaneously check (or recheck) blood glucose and initiate feeds. Blood glucose 38 mg/dL is below the treatment threshold of 45 mg/dL and requires glucose supplementation (oral feed first if able to suck; IV if not). However, warming must accompany glucose correction, because cold stress will continue to consume glucose without rewarming. A sepsis workup is warranted but is not the FIRST action — the thermal context (cold delivery room, not dried) provides a clear explanation. Glucagon is not first-line for neonatal hypoglycaemia.
Management: The Warm Chain and Rewarming
Management of neonatal thermal care consists of two distinct but overlapping strategies: prevention (the Warm Chain at birth and in the immediate postnatal period) and treatment (rewarming of the hypothermic neonate). Both are guided by the same physiological principles — minimise heat loss and optimise heat production. The practical significance of this framing is that prevention is always preferable to treatment: a hypothermic neonate who arrives at a health facility has already suffered cold stress, metabolic consequences, and potentially life-threatening complications that a simple Warm Chain implementation would have prevented. The clinician who internalises the Warm Chain as physiology rather than as a checklist implements it reliably across all settings.
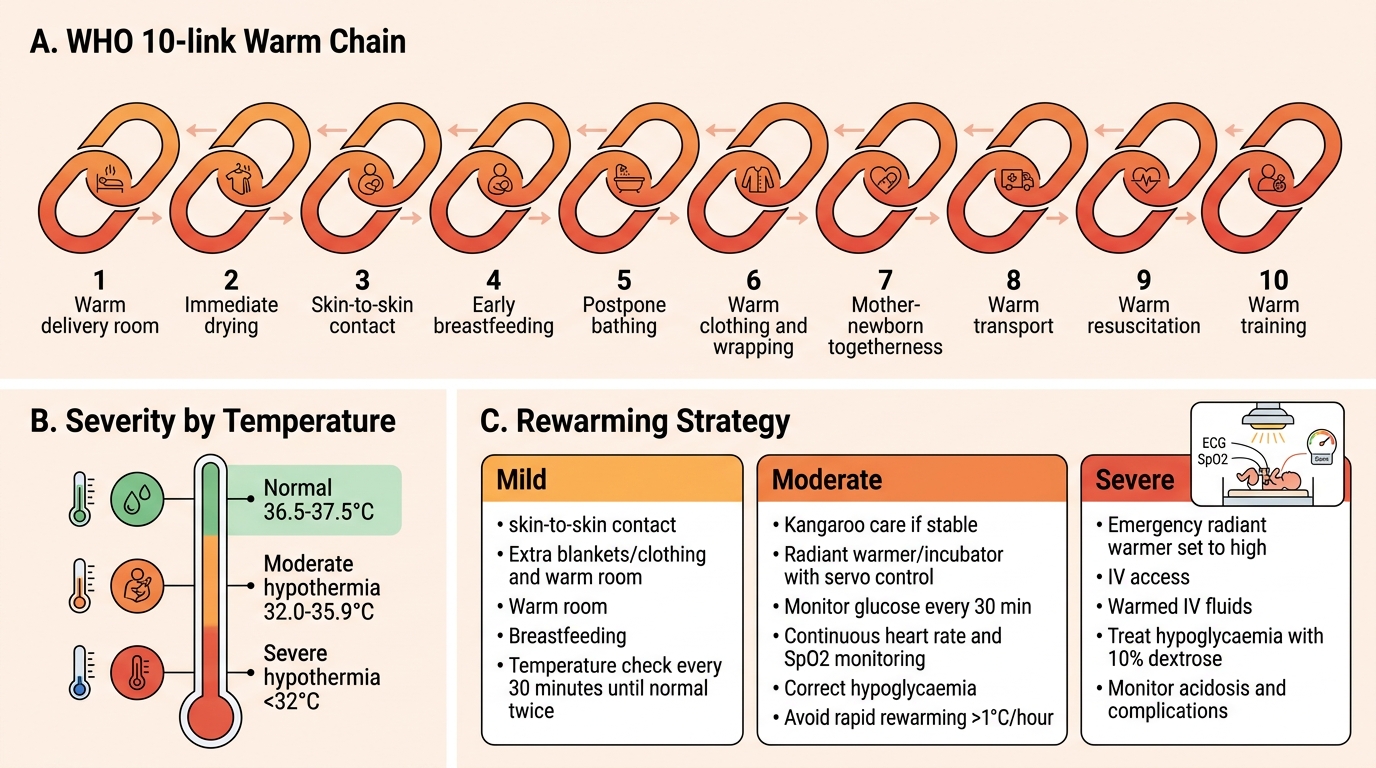
The WHO Warm Chain — 10 links:
The Warm Chain is a set of 10 evidence-based actions at birth and in the first hours designed to prevent hypothermia by eliminating avoidable heat loss. Each 'link' addresses a specific mechanism:
- Warm delivery room (≥25°C): reduces convective and radiant heat loss to the environment
- Immediate drying: removes amniotic fluid — eliminates evaporative heat loss (the largest initial heat loss mechanism)
- Skin-to-skin contact (Kangaroo Care): mother's chest provides a regulated thermal environment; promotes breastfeeding and hormone-mediated attachment
- Breastfeeding: provides fuel (glucose and fat) for thermogenesis; initiates gut function
- Postpone bathing: delay bath by at least 24 hours (or 6 hours minimum per revised guidance); bath removes the remaining vernix (insulating) and is a major cold stress
- Appropriate clothing and wrapping: hat (head is ~20% of total surface area in a neonate — loses heat disproportionately), blankets, socks, wrapped body
- Mother and newborn together (rooming-in): allows continuous monitoring of feeding, thermal status, and early recognition of problems; prevents separation-associated cooling
- Warm transport: during transfer to nursery or another facility, wrap in blankets, use an incubator with heat or skin-to-skin in the transport vehicle
- Warm resuscitation: resuscitation under a pre-warmed radiant warmer; dry and cover even during resuscitation to prevent conductive/evaporative losses
- Training: all birth attendants and nurses must receive standardised training in recognising and preventing hypothermia
WHO Warm Chain and Neonatal Hypothermia Rewarming
Rewarming strategies by severity:
Mild hypothermia (36.0–36.4°C): non-invasive methods are sufficient — skin-to-skin contact with mother (most effective, natural), extra clothing and blankets, ensure room is warm, encourage breastfeeding. Monitor temperature every 30 minutes until normal for 2 consecutive readings.
Moderate hypothermia (32–35.9°C): active rewarming required:
- Kangaroo/skin-to-skin care (preferred for stable neonates) — rewarms at the physiological rate of ~0.5°C/hour
- Radiant warmer or incubator with servo control (set to achieve 36.5°C skin temperature) — for sick or preterm neonates who cannot be held
- Mandatory concurrent monitoring: blood glucose every 30 minutes, heart rate and SpO2 continuous, blood gas if acidosis suspected
- IV/oral glucose correction for hypoglycaemia
- Avoid rapid rewarming (>1°C/hour) — causes vasodilation and cardiovascular instability
Severe hypothermia (<32°C): emergency management:
- Radiant warmer on high + IV access immediately
- Warm IV fluids (pre-warmed to 37°C if possible) to prevent IV-mediated cooling
- Treat complications: hypoglycaemia (IV 10% dextrose bolus 2 mL/kg + infusion), acidosis (NaHCO3 only if pH <7.1 and documented respiratory adequacy), coagulopathy (FFP, Vitamin K if not given)
- NICU admission; neonatologist involvement
- Full sepsis screen (severe hypothermia requires exclusion of sepsis regardless of clear thermal explanation)
Prevention of hyperthermia:
Neonates under radiant warmers or in incubators must have temperature monitored continuously — servo-controlled mode (automatically adjusts heater output to maintain target skin temperature) is safer than manual mode. A neonate at 38.5°C under a radiant warmer in manual mode is at risk of brain injury from hyperthermia.
SELF-CHECK
Which of the following is the MOST important single action to prevent hypothermia in the immediate post-delivery period?
A. Administering IV glucose prophylactically to all neonates
B. Placing the neonate in an incubator set to 35°C
C. Immediate thorough drying with a warm towel after birth
D. Applying a hat and mittens before cutting the umbilical cord
Reveal Answer
Answer: C. Immediate thorough drying with a warm towel after birth
Immediate drying is the single most important first action in the Warm Chain because evaporation of amniotic fluid is the dominant mechanism of heat loss immediately after birth. A wet neonate loses body heat alarmingly fast through evaporation — the wet surface dramatically accelerates heat loss by all other mechanisms simultaneously. Drying must be vigorous and immediate. Once dried, skin-to-skin contact is the next priority. Incubator care is not required for stable term neonates. IV glucose prophylaxis is not indicated for normoglycaemic neonates. Hats are important but secondary to drying.
Self-Assessment: Thermal Care Scenarios
Apply the thermal care framework to the following scenarios. For each, identify the thermal status, the likely mechanism of heat loss or gain, and the appropriate management. These scenarios are designed to build confidence in making rapid thermal assessments at the bedside. Each tests a different domain: recognition and grading, implementation of prevention at a facility delivery, and the critical diagnostic distinction between environmental hyperthermia and true fever. Work through each independently before reading the structured responses — the process of reasoning under simulated time pressure is the most effective way to consolidate clinical decision-making frameworks.
Scenario 1 — Moderate hypothermia recognition and rewarming:
A 12-hour-old term neonate (born at home, December, Rajasthan) is brought to the PHC. Temperature 34.2°C axillary. The baby is quiet, hypotonic, and not feeding. Blood glucose is 34 mg/dL. There is no history of maternal fever or prolonged rupture of membranes.
- Thermal grade: moderate hypothermia (34.2°C, 32–35.9 range)
- Mechanisms: the baby was not dried at birth, not kept warm (cold December home environment), delayed postnatal care = evaporation + convection + radiation from birth
- Management sequence: (a) Immediate skin-to-skin with mother on a warm surface; wrap both in blankets; (b) Simultaneously give early feed (expressed breast milk or formula, 5–10 mL) OR IV 10% dextrose 2 mL/kg bolus given blood glucose 34 mg/dL is <45 mg/dL; (c) Monitor temperature and blood glucose every 30 minutes; (d) Expect temperature to rise at ~0.5°C/hour with skin-to-skin; (e) Sepsis screen if temperature does not normalise within 2 hours or if clinical deterioration
Scenario 2 — Warm Chain implementation at a facility delivery:
You are the house officer in a district hospital labour ward. A baby is about to be delivered by normal vaginal delivery in November. List five Warm Chain actions you will implement in the first 5 minutes.
- Pre-warm the radiant warmer and lay a pre-warmed towel on it (warm delivery surface + pre-warmed wrap)
- Ensure delivery room windows are closed and room temperature ≥25°C
- At birth: immediately place on radiant warmer and DRY VIGOROUSLY with the warm towel — discard the wet towel
- Assess breathing and APGAR; if baby is well — initiate skin-to-skin contact with mother and cover both with a blanket (do not separate for routine care)
- Attach a hat; defer the first bath by at least 24 hours
Scenario 3 — Hyperthermia vs fever in a neonate:
A 4-day-old term breastfed neonate has a temperature of 38.2°C. The mother reports that the baby has been wrapped in 4 layers of blankets. The neonate is active, feeding well, and the anterior fontanelle is flat.
- Initial assessment: this is consistent with environmental overheating (excess clothing + high ambient temperature). The neonate is otherwise well.
- Initial action: remove excess clothing; measure temperature in 30 minutes
- If temperature normalises to <37.5°C with cooling: environmental hyperthermia confirmed; counsel mother on appropriate clothing
- If temperature persists or neonate appears unwell: full sepsis evaluation — a neonate with fever must be investigated for infection (CBC, CRP, blood culture, LP) because neonatal sepsis can be rapidly fatal and cannot be excluded clinically
- KEY RULE: Never attribute neonatal fever to 'wrapping' without first ensuring the baby is well and then confirming resolution with environmental correction