Page 43 of 53
PE19.16 | Newborn Surgical Red Flags — SDL Guide
Learning Objectives
- Identify the five key surgical red-flag presentations in the newborn requiring immediate referral
- Describe the embryological basis and anatomy relevant to tracheo-oesophageal fistula, malrotation, Hirschsprung disease, anorectal malformation, CDH, and abdominal wall defects
- Recognise the clinical presentation of each common neonatal surgical condition at the bedside
- Initiate appropriate immediate stabilisation steps before surgical transfer
- Communicate findings to the surgical team using a structured handover and counsel parents appropriately
INSTRUCTIONS
The newborn period contains some of the most time-sensitive surgical emergencies in all of medicine. A baby vomiting bilious fluid, unable to swallow its own secretions, or with a hollow abdomen needs a surgeon — not watchful waiting. This module equips you to recognise the key surgical red-flag presentations in newborns, understand their anatomical and embryological basis, and initiate the correct stabilisation steps before transfer. The competency is identification and first-response, not operative management; but early recognition determines survival.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 7 (Neonatal Surgery) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 356–368 (Congenital Anomalies) (textbook)
- Puri P. Newborn Surgery, 4th ed. — Standard reference for neonatal surgical emergencies (textbook)
- IAP Guidelines on Management of Common Neonatal Surgical Emergencies (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 3 AM in the postnatal ward. You are called to assess a 12-hour-old male, born at term by normal vaginal delivery. The mother reports he has vomited twice — both times the vomit was bright green in colour. The baby is now restless and the abdomen appears mildly distended. Your registrar says, 'Probably just a feed problem — we'll watch.' You know you have seen something in your paediatric surgery posting about green vomiting in neonates. You also recall that bilious vomiting in a newborn means the obstruction is distal to the ampulla of Vater — and that malrotation with volvulus can infarct the entire midgut in hours. You pick up the phone and call the surgeon.
WHY THIS MATTERS
Neonatal surgical conditions are individually rare but collectively account for a significant proportion of neonatal intensive care admissions and neonatal deaths. Many present as deceptively mild symptoms in the first hours of life — a baby choking on feeds, failing to pass meconium, or vomiting green — symptoms that in an adult might prompt observation but in a newborn demand immediate investigation and surgical referral. The cost of missing a malrotation volvulus, tracheo-oesophageal fistula, or Hirschsprung disease is measured in lives and in permanent disability. As a junior doctor on the postnatal ward, you are the first clinician to examine these babies; your systematic red-flag recognition is the safety net.
RECALL
Recall from embryology that the gut is derived from the primitive gut tube — foregut (oesophagus, stomach, proximal duodenum), midgut (distal duodenum to two-thirds of transverse colon), and hindgut (distal colon to anal canal). The midgut undergoes physiological herniation into the umbilical cord at weeks 6–10, then returns to the abdominal cavity and rotates 270° counter-clockwise around the superior mesenteric artery (SMA) — arrest of this rotation = malrotation. The trachea and oesophagus separate from a common foregut tube by the tracheo-oesophageal septum at weeks 4–5; failure of this septum produces tracheo-oesophageal fistula (TOF). The anorectum develops from the cloaca, divided by the urorectal septum; neural crest cells must migrate craniocaudally to colonise the entire colon; failure of migration produces Hirschsprung aganglionosis. Recall also that meconium (sterile fetal gut contents — mucus, bile, lanugo, amniotic fluid) is normally passed within 24–48 hours of birth in term neonates.
Clinical Indication: When to Suspect a Surgical Emergency in the Newborn
Five cardinal surgical red-flag presentations in the newborn should be committed to memory, because each represents a time-sensitive condition where hours — sometimes minutes — determine outcome. Unlike adults, in whom a single symptom rarely demands immediate surgery, the newborn gut has no physiological reserve — an ischaemic bowel in a 3-kilogram baby progresses to infarction faster than any diagnostic algorithm can be completed. These red flags are pattern-recognition triggers: recognising one should produce a reflex of nil by mouth, IV access, immediate investigation, and surgical referral rather than a period of observation. The threshold for calling the paediatric surgeon must be low, and the paediatrician must be able to communicate the urgency clearly. The five key red flags, their associated diagnoses, and the time windows for action are described below.
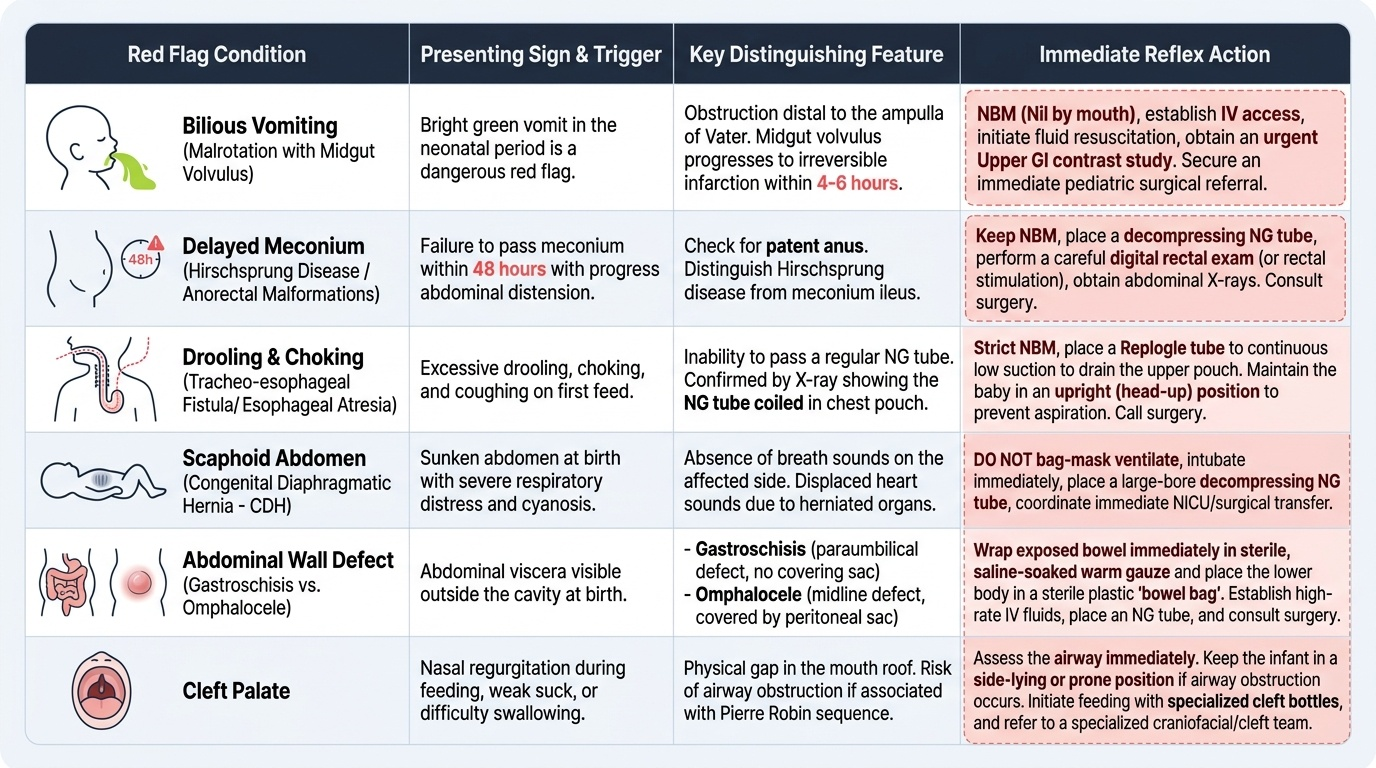
Provided image
- Bilious (green) vomiting at any age in the neonatal period — the most dangerous red flag. The ampulla of Vater (where bile enters the duodenum) is at the level of D2; any vomit that contains bile implies an obstruction distal to the ampulla. The leading emergency diagnosis is malrotation with midgut volvulus (ischaemia of the entire midgut within 4–6 hours), but duodenal atresia, jejunal atresia, and incarcerated hernia are also in the differential.
- Failure to pass meconium by 48 hours in a term neonate, especially with abdominal distension — raises concern for Hirschsprung disease, anorectal malformation (imperforate anus), or meconium ileus (cystic fibrosis). Always check whether the anus is present and patent before attributing this to Hirschsprung.
- Drooling, choking, or coughing on first feed + respiratory distress — the hallmark of tracheo-oesophageal fistula (TOF) with oesophageal atresia (OA). The baby cannot swallow secretions; the upper oesophagus ends in a blind pouch. Attempting to pass a nasogastric tube and finding it coiled in the upper chest on X-ray confirms the diagnosis.
- Abdominal wall defect visible at birth — gastroschisis (bowel herniated through a right paraumbilical defect, no covering sac) is a true emergency requiring immediate bowel protection; omphalocele (central defect covered by a peritoneal sac) is urgent but slightly more stable, though associated with major cardiac and chromosomal anomalies.
- Scaphoid (hollow/boat-shaped) abdomen + respiratory distress at birth with mediastinal shift — congenital diaphragmatic hernia (CDH), where abdominal viscera herniate into the thorax through a posterior diaphragmatic defect, compressing the ipsilateral lung and shifting the mediastinum to the contralateral side.
Additionally, cleft lip and/or palate identified at birth creates an acute feeding problem and potential airway risk; while not immediately life-threatening, it requires immediate specialised feeding support and surgical planning.
Anatomy and Embryological Basis of Surgical Conditions
Understanding the embryological basis of each condition clarifies why the presenting symptom is specific and why the anatomy matters for surgical repair.
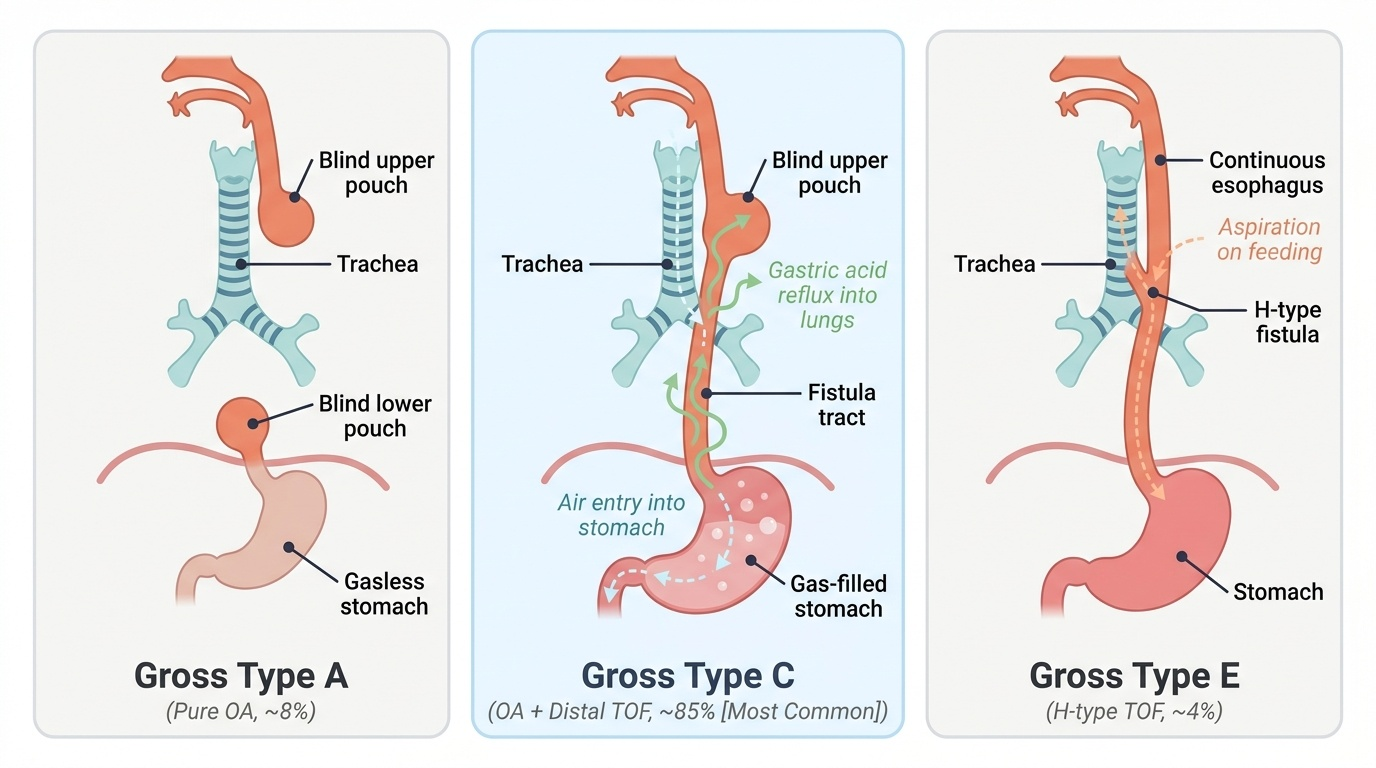
Provided image
Tracheo-oesophageal fistula and oesophageal atresia (TOF/OA): The most common classification is Gross Type C (approximately 85% of cases) — oesophageal atresia with a distal fistula connecting the lower trachea to the stomach, allowing air to enter the stomach (visible on plain X-ray as a gas-filled stomach) and gastric acid to reflux into the lungs through the fistula. Gross Type A (pure OA, ~8%) has no fistula — the stomach is gasless on X-ray. Gross Type E (H-type TOF, ~4%) has a fistula without atresia — these babies present later with recurrent aspiration pneumonia and choking on feeds, not with failure to swallow.
Malrotation and volvulus: When the midgut fails to complete its 270° rotation, the caecum is abnormally located (often in the mid-abdomen or left side). Ladd's bands — fibrous adhesive bands — form between the caecum and the right posterior abdominal wall, potentially compressing the duodenum. More critically, the mesenteric root is narrow (instead of spanning from the duodenojejunal flexure to the ileocaecal region), making the entire midgut susceptible to twisting around the SMA axis — a volvulus that obstructs both the bowel and its blood supply.
Hirschsprung disease (HD): Failure of neural crest cell migration during embryogenesis results in aganglionosis — absence of both Meissner's submucosal and Auerbach's myenteric ganglia — in the affected segment. The aganglionic bowel (which is always the distal rectum and extends proximally) is tonically contracted and cannot generate peristalsis; the proximal normal bowel becomes progressively dilated. In short-segment HD (rectosigmoid, ~75% of cases), the baby fails to pass meconium and develops increasing abdominal distension; a rectal examination often precipitates a gush of meconium ("squirt sign"), and the aganglionic segment is felt as a contracted, narrow rectum.
Anorectal malformations (ARM): The spectrum ranges from low lesions (fistula to perineum, visible opening, good prognosis for continence) to high lesions (supralevator, no visible opening, associated with sacral agenesis, poor continence prognosis). VACTERL association should be actively sought in every ARM — Vertebral, Anal, Cardiac, Tracheo-Esophageal, Renal, and Limb anomalies cluster together because they share a common embryological window.
Congenital diaphragmatic hernia (CDH): The left-sided Bochdalek hernia (~85%) results from failure of the left pleuroperitoneal membrane to close, allowing stomach, small bowel, spleen, and sometimes liver to herniate into the left thorax. The ipsilateral lung is compressed during critical stages of branching morphogenesis, producing pulmonary hypoplasia (reduced airway and vessel generations on both sides) — this, not just the herniated bowel, determines survival.
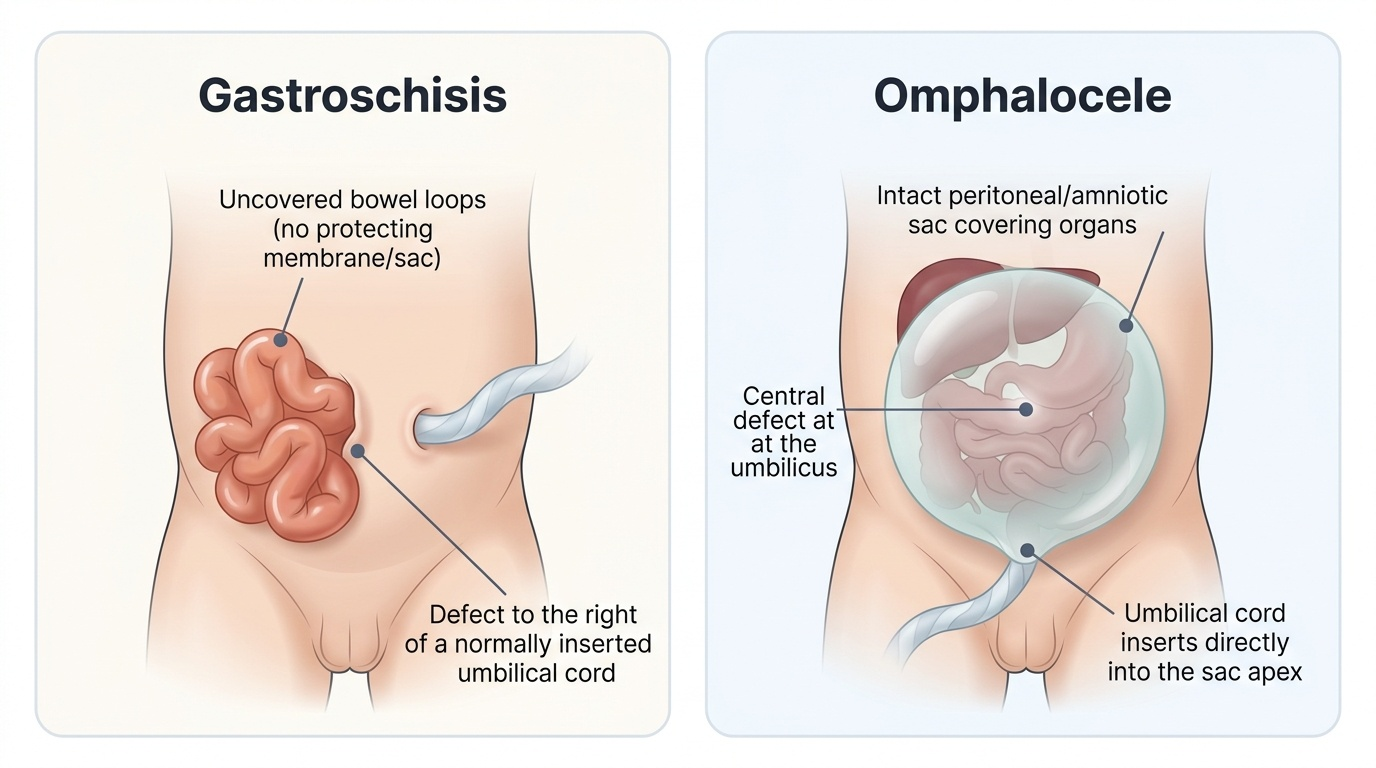
Gastroschisis vs omphalocele: Gastroschisis is a paraumbilical (right-sided) full-thickness abdominal wall defect with no sac — the exposed bowel develops chemical peritonitis (peel) from amniotic fluid exposure and is at risk of evaporative heat and fluid loss, ischaemia, and trauma at delivery. Omphalocele is a central defect at the base of the umbilical cord, covered by a peritoneal/amniotic membrane sac; the sac may contain bowel, liver, and spleen. Omphalocele is associated with chromosomal anomalies (trisomy 13, 18, 21) and Beckwith-Wiedemann syndrome, while gastroschisis is typically isolated.
SELF-CHECK
A 2-hour-old term neonate produces copious oral secretions, chokes on first feed, and has mild respiratory distress. A nasogastric tube is passed and the X-ray shows the tube coiled in the upper chest. The abdomen has gas visible in the stomach and proximal bowel. What is the most likely diagnosis?
A. Oesophageal atresia without fistula (Gross Type A)
B. Oesophageal atresia with distal TOF (Gross Type C)
C. Duodenal atresia
D. Pyloric stenosis
Reveal Answer
Answer: B. Oesophageal atresia with distal TOF (Gross Type C)
Gas in the stomach and bowel on X-ray means air is reaching the GI tract through a fistula connecting the distal trachea to the oesophagus/stomach — this is Gross Type C (OA with distal TOF), the most common variant (~85%). In Gross Type A (pure OA, no fistula), the stomach would be gasless because no air reaches the GI tract. Duodenal atresia causes bilious vomiting with a 'double bubble' on X-ray, not choking on first feeds. Pyloric stenosis presents at 3–6 weeks with non-bilious projectile vomiting, not at 2 hours of age.
Clinical Presentation and Recognition at the Bedside
Each neonatal surgical condition has a constellation of clinical features that, when recognised early, allows immediate action. The following condition-by-condition guide prioritises the bedside signs that distinguish each diagnosis and the do-not-miss hallmarks.
Provided image
Malrotation with midgut volvulus: Bilious vomiting is the cardinal sign — typically early, forceful, and not preceded by a feed problem. Abdominal distension may be absent initially (high obstruction); haemodynamic instability and blood in stool are late signs indicating ischaemia. On X-ray, the duodenal-jejunal flexure (DJ flexure) may be abnormally located to the right of the spine (normally left of midline). Upper GI contrast study (gold standard) shows the DJ flexure in an abnormal position and possibly a 'corkscrew' sign of volvulus. Surgical referral is IMMEDIATE — do not wait for the contrast study if the baby is haemodynamically deteriorating.
Duodenal atresia: "Double bubble" sign on abdominal X-ray (dilated stomach + dilated proximal duodenum, no gas distally) is pathognomonic. Associated with Down syndrome (trisomy 21) in ~30% of cases. May be detected antenatally with polyhydramnios. Presentation is bilious vomiting but the baby is typically more stable than volvulus.
Hirschsprung disease: Term neonate with failure to pass meconium in 48 hours + progressive abdominal distension. Rectal examination reveals a tight, narrow rectum; withdrawal of the finger is followed by a gush of meconium and flatus (the "squirt sign"). Contrast enema may show the narrow aganglionic segment transitioning to dilated proximal bowel, but definitive diagnosis requires suction rectal biopsy (absence of ganglion cells on histopathology, with increased acetylcholinesterase staining).
Anorectal malformation (imperforate anus): Visible on newborn examination — the anus is absent or abnormally located. A fistula may open onto the perineum (low ARM) or into the vestibule/vagina in females or the urethra in males (high ARM). Always check for associated VACTERL components (spine, cardiac, renal anomalies) with X-ray, echo, and renal ultrasound.
TOF/OA: Excessive oral secretions and bubbling from birth, choking on first feed, cyanosis. Nasogastric tube cannot be advanced more than ~10–12 cm — it coils in the upper oesophageal pouch. Babygram (chest + abdomen X-ray): tube coiled in upper chest; gas in the stomach if distal fistula (Type C), gasless abdomen if Type A. Associated anomalies in ~50% (VACTERL).
CDH: Respiratory distress immediately after birth (or within hours), shifted heart sounds (mediastinal shift AWAY from the side of the hernia), absent breath sounds on the ipsilateral side, and a scaphoid (hollow) abdomen (because abdominal contents are in the chest). CXR shows bowel loops in the thorax and mediastinal shift.
Gastroschisis vs omphalocele:
| Feature | Gastroschisis | Omphalocele |
|---|---|---|
| Location | Right of umbilicus | At umbilicus |
| Covering sac | None — bowel directly exposed | Peritoneal/amniotic sac present |
| Bowel appearance | Matted, thickened (chemical peel) | Normal |
| Associated anomalies | Rare; typically isolated | Common (trisomy 13/18/21, BWS) |
| Urgency | Extreme — bowel protection immediately | Urgent, slightly more stable |
CLINICAL PEARL
Bilious vomiting in a newborn is a surgical emergency until proven otherwise. The word 'bilious' means green or yellow — bile-stained. The ampulla of Vater opens into the second part of the duodenum; any vomit containing bile means the obstruction is distal to this point and the midgut is at risk. Malrotation with volvulus is the most time-critical diagnosis — the entire midgut (from mid-duodenum to transverse colon) can infarct and become irretrievably lost within 4–6 hours of volvulus onset. A baby who loses the midgut is committed to a lifetime of short-bowel syndrome and parenteral nutrition. 'Watch and see if the next feed is also green' is not an acceptable plan. Call the surgeon immediately, establish IV access, make the baby nil by mouth, and arrange urgent upper GI contrast study or take directly to theatre.