Page 44 of 53
PE19.16 | Newborn Surgical Red Flags — SDL Guide (Part 2)
Interpretation of Findings and Initial Stabilisation
Once a surgical red flag is identified, the paediatrician's role is immediate stabilisation and safe transfer — not definitive surgery. This distinction is critical: the clinician at the district hospital or general paediatric ward is not expected to perform a Ladd's procedure or repair a diaphragmatic hernia, but is expected to recognise the condition, prevent deterioration, initiate investigations, and transfer the baby safely to a paediatric surgical centre with all clinical information documented. Every minute of delay in stabilisation translates into additional physiological compromise: a volvulus progresses to ischaemia, a CDH baby develops worsening hypoxia from bag-mask distension, and an unstabilised gastroschisis baby loses large volumes of fluid through exposed viscera. The universal and condition-specific stabilisation steps are described below, and each must be initiated concurrently rather than sequentially.
Provided image
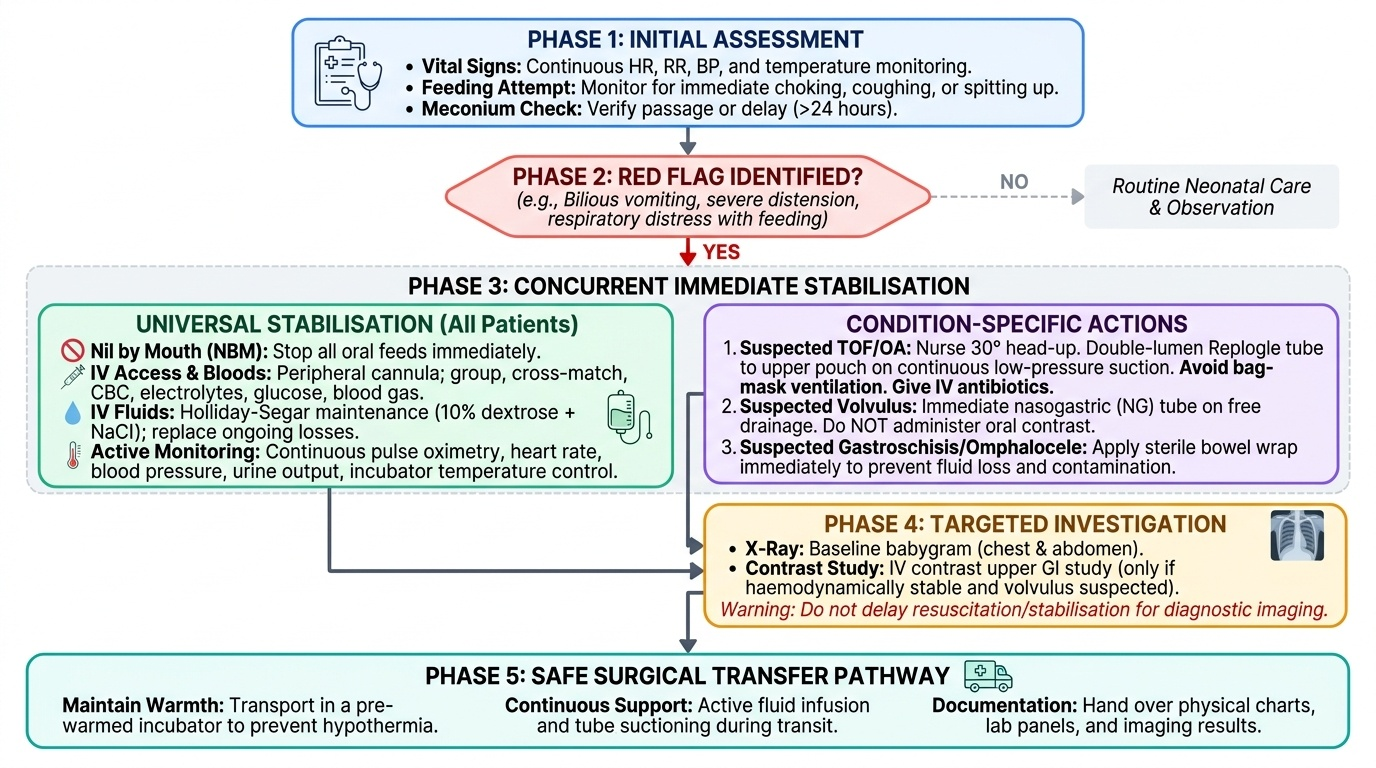
Universal immediate steps for any suspected neonatal surgical emergency:
• Nil by mouth (NBM) — stop all oral feeds immediately
• IV access — peripheral cannula; draw bloods (blood group and cross-match, CBC, electrolytes, glucose, blood gas); send to lab before transfer
• IV fluids — maintenance using Holliday-Segar (100 mL/kg/day for first 10 kg in neonates; typically 10% dextrose with NaCl supplements until electrolytes known); replace ongoing losses (surgical drains, NG aspirate) volume-for-volume
• Monitor — continuous pulse oximetry, heart rate, blood pressure, urine output (catheterise if needed)
• Temperature control — neonates are vulnerable to hypothermia; use a warmer or incubator during transfer
Condition-specific stabilisation:
TOF/OA: Nurse the baby at 30° head-up (reduces gastric acid reflux through the fistula into the lungs). Insert a Replogle tube (double-lumen sump catheter) into the upper oesophageal pouch on continuous low-pressure suction — this prevents overflow aspiration of secretions. Avoid bag-mask ventilation if possible (distends the stomach through the fistula). Give IV antibiotics (aspiration pneumonia prophylaxis).
Suspected volvulus: Immediate NBM + nasogastric tube on free drainage. Do NOT give oral contrast — use IV contrast upper GI study or take directly to theatre if haemodynamically unstable. Time-to-surgery is the most important variable.
Gastroschisis: The exposed bowel must be protected immediately. Wrap bowel in sterile warm saline-soaked gauze and cover with cling film (or use a bowel bag); this reduces evaporation, heat loss, and infection. Place a nasogastric tube to decompress the stomach. Nurse the baby on the side so the bowel is not kinked. Volume resuscitation is essential — gastroschisis babies lose large amounts of fluid from the exposed viscera.
CDH: Avoid bag-mask ventilation (insufflates bowel, worsens herniation). Intubate and ventilate if respiratory distress is severe. Insert a nasogastric tube to decompress herniated stomach/bowel. High-frequency oscillatory ventilation or inhaled nitric oxide may be required for pulmonary hypertension in specialist units.
Investigations before transfer:
• Plain X-ray (chest + abdomen, 'babygram') — single film captures coiled NG tube, double bubble, mediastinal shift, bowel in thorax
• Echocardiography — CDH (pulmonary hypertension), omphalocele/OA (VACTERL cardiac anomalies)
• Renal ultrasound — anorectal malformations, OA/VACTERL
• Blood gas — severity of respiratory compromise in CDH; acidosis in volvulus (late sign)
SELF-CHECK
A term newborn female has no visible anal opening on examination at birth. Urine appears slightly yellow-stained (meconium-coloured). Which of the following is the MOST appropriate next step?
A. Rectal examination to check for Hirschsprung disease
B. Perform a barium enema immediately
C. Assess for VACTERL anomalies and refer urgently to a paediatric surgeon
D. Observe for 48 hours to see if meconium passes spontaneously
Reveal Answer
Answer: C. Assess for VACTERL anomalies and refer urgently to a paediatric surgeon
Absent anal opening with meconium-stained urine suggests a high anorectal malformation (ARM) with a recto-urinary fistula — urine is draining through a fistula from the rectum. This is not a wait-and-see situation. The priority is immediate surgical referral and systematic assessment for VACTERL-associated anomalies (Vertebral, Anal, Cardiac, Tracheo-Esophageal, Renal, Limb). A spine X-ray, echocardiogram, and renal ultrasound are needed before surgical planning. Rectal examination cannot identify aganglionosis in ARM. Barium enema is not the first step and must be preceded by clinical assessment.
Applied and Supervised Practice: Handover and Communication
Effective communication in the context of a neonatal surgical emergency is a clinical skill that must be practised consciously, because the consequences of a poorly structured handover are as serious as a delayed diagnosis. The paediatric clinician who identifies a surgical red flag must translate that recognition into two simultaneous communication tasks: a precise, structured handover to the paediatric surgeon and an accurate, compassionate explanation to the parents — each requiring a different register, different content, and different emotional tone. The surgeon needs a concise SBAR summary with the clinical decision already stated; the parents need honest acknowledgement of what was found, what is being done, and what will happen next — without premature diagnostic certainty and without minimising their fear. Practise both, because the ability to manage clinical urgency and family distress simultaneously is the mark of a competent junior doctor.
SBAR handover to the paediatric surgeon (practise this structure):
• Situation: 'I have a 6-hour-old term male with bilious vomiting — two episodes of green vomit — who is now tachycardic and has a mildly distended abdomen. I am concerned about malrotation with volvulus.'
• Background: 'Born at 39+2 weeks by SVD, Apgar 9/10. Birth weight 3.2 kg. No antenatal anomaly detected. Vomiting started at 4 hours of life.'
• Assessment: 'He is currently haemodynamically borderline — HR 168, BP 52/34, SpO₂ 97% on air. Abdomen not rigid. No blood per rectum yet. I've placed an IV line, stopped feeds, placed an NG tube, and sent bloods.'
• Request: 'I need you to see him urgently — can you come now or should I arrange transfer to your centre? I'll organise an upper GI contrast study in parallel.'
Counselling the parents: Parents of a baby with a suspected surgical condition are frightened and need honest, compassionate communication without premature diagnostic certainty. The key principles are: (1) acknowledge what you have seen and why it concerns you ('Your baby's vomit is green — that tells us there may be a problem with the bowel that needs the surgeon's assessment'); (2) do not assign a final diagnosis before investigations are done; (3) explain what is being done ('We are stopping feeds, placing a drip, and calling a specialist right now'); (4) do not minimise ('It could be nothing' is dangerous and dishonest) and do not catastrophise ('Your baby is about to die' is premature); (5) tell them where their baby is going and when they will hear news.
For anorectal malformation, cleft lip/palate, and abdominal wall defects — conditions that are visible — the parents have already seen the abnormality. Acknowledge their shock, provide basic information, and ensure they have a named person to contact. Avoid speculating about prognosis before specialist review.
Documentation: Write a clear, timed note. Record the clinical findings, investigations ordered, who was contacted (name + time), and the plan. In time-sensitive emergencies, documentation can be done after immediate stabilisation but must not be omitted.
SELF-CHECK
A term neonate delivered at a district hospital is found to have loops of bowel protruding through a defect to the right of the umbilicus, with no covering membrane. The nearest paediatric surgical unit is 2 hours away. What is the MOST appropriate immediate management?
A. Cover the bowel with dry gauze and transfer immediately
B. Wrap exposed bowel in sterile warm saline-soaked gauze, cover with cling film, establish IV access, and arrange immediate transfer
C. Attempt primary reduction and closure at the district hospital
D. Place a nasogastric tube only and wait for the surgical team to arrive
Reveal Answer
Answer: B. Wrap exposed bowel in sterile warm saline-soaked gauze, cover with cling film, establish IV access, and arrange immediate transfer
This is gastroschisis — an abdominal wall defect to the right of the umbilicus with exposed uncovered bowel. The priority is bowel protection: wrap in sterile warm saline-soaked gauze and cover with cling film or a sterile bowel bag to prevent evaporative losses, heat loss, and infection. IV access and IV fluids are essential — fluid loss from exposed viscera is massive. Nil by mouth. Then arrange immediate transfer. Dry gauze (option A) causes desiccation and tissue injury. Primary repair at a district hospital without a paediatric surgeon is not appropriate. A nasogastric tube alone (option D) addresses only one element of stabilisation.
Self-Assessment: Newborn Surgical Red Flags
This section consolidates your recognition and response framework for neonatal surgical emergencies, integrating the anatomy, clinical presentation, and stabilisation steps you have covered in this module. Before reviewing the micro-quiz answers, work through the following diagnostic framework independently for each scenario: (1) Which red flag pattern does this presentation match — bilious vomiting, failure to pass meconium, drooling/choking, abdominal wall defect, or scaphoid abdomen? (2) What is the most dangerous diagnosis on the differential, and what is the time window before irreversible injury occurs? (3) What are the immediate stabilisation steps you initiate before the surgeon arrives? (4) What single investigation would most rapidly confirm or refute the leading diagnosis, and what finding would you look for?
The table below summarises the key distinguishing features of the major neonatal surgical conditions covered in this module. Use it as a self-check against your reading of the clinical vignettes in the micro-quiz sections above.
| Condition | Red flag | Key imaging finding | Most dangerous complication | Immediate action |
|---|---|---|---|---|
| Malrotation + volvulus | Bilious vomiting | Upper GI: DJ flexure right of midline / corkscrew | Midgut infarction | NBM + IV + call surgeon STAT |
| Duodenal atresia | Bilious vomiting | 'Double bubble' CXR/AXR | Aspiration | NBM + NG + IV |
| Hirschsprung disease | No meconium >48h + distension | Contrast enema: transition zone; biopsy: no ganglion cells | Enterocolitis | NBM + NG + surgical referral |
| TOF/OA (Type C) | Drooling + choking + gas in stomach | NG tube coiled in chest; gas in abdomen | Aspiration pneumonia | Replogle tube + head-up + IV ABx |
| CDH | Respiratory distress + scaphoid abdomen | Bowel loops in thorax on CXR | Pulmonary hypoplasia + PPHN | Intubate + NG + no bag-mask |
| Gastroschisis | Exposed bowel, right paraumbilical | Clinical diagnosis | Bowel ischaemia + hypothermia | Bowel wrap + IV fluids STAT |
| Omphalocele | Bowel/liver in sac at umbilicus | Clinical; echo + renal USS for anomalies | Chromosomal/cardiac co-morbidity | Sac protection + IV + referral |
| Imperforate anus | No anal opening | Invertogram / MRI pelvis | Recto-urinary fistula + sepsis | VACTERL screen + surgical referral |
Reflect on the VACTERL association — every case of TOF/OA, anorectal malformation, or vertebral anomaly should prompt a systematic search for the other components, because missing a cardiac defect or renal agenesis in the same baby compounds morbidity.