Page 46 of 53
PE19.17 | Oxygen Toxicity — SDL Guide
Learning Objectives
- Identify the neonates at risk for oxygen toxicity and the clinical contexts in which it occurs
- Explain the pathophysiology of retinopathy of prematurity (ROP) and bronchopulmonary dysplasia (BPD) as the principal manifestations of oxygen toxicity
- Apply the NNF India screening criteria for ROP (gestational age ≤34 weeks or birth weight ≤1800g) and describe the zone and stage classification
- State the target SpO2 range (90–95%) for preterm neonates on supplemental oxygen and the evidence behind it
- Describe the management options for Type 1 ROP (laser photocoagulation and anti-VEGF) and the supportive management of BPD
INSTRUCTIONS
Oxygen — administered every day in neonatal intensive care units — is simultaneously a life-saving intervention and a toxic agent. The premature infant's incompletely developed retinal vasculature and immature antioxidant defences make supplemental oxygen both necessary and dangerous. Retinopathy of prematurity (ROP) and bronchopulmonary dysplasia (BPD) are the two most consequential complications of oxygen therapy in the preterm neonate, and both are preventable with careful monitoring and evidence-based SpO2 targets. As a paediatrician, you will prescribe oxygen, manage the monitoring of preterm neonates, and counsel families about the risk of these complications — this module builds that clinical foundation.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 7 (Neonatology — Retinopathy of Prematurity, BPD) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 109 (Retinopathy of Prematurity), Ch. 115 (Chronic Lung Disease) (textbook)
- NNF India Screening Guidelines for ROP (2021 update) (guideline)
- AAP/American Academy of Ophthalmology: Screening Examination of Premature Infants for Retinopathy of Prematurity (2018) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Baby Priya was born at 28 weeks gestation, weighing 950 grams. She was intubated immediately and has been in the NICU for 5 weeks. Her respiratory status has improved, but she still requires 35% oxygen via CPAP to maintain comfortable saturations. The nurse calls you to say the SpO2 alarm has been alarming frequently — going up to 98% when she is on increased flow and dipping to 85% during feeds. You check the target saturation range prescribed: 91–95%. You recall that too much oxygen causes ROP and lung damage; too little causes hypoxic injury and death. Today, the ophthalmologist visits to do the ROP screening — and you need to understand what you are looking for and what the findings mean.
WHY THIS MATTERS
Retinopathy of prematurity is the leading cause of childhood blindness in India and in many low- and middle-income countries, and its prevalence is rising as neonatal intensive care capacity expands to save smaller and more premature babies. Bronchopulmonary dysplasia similarly affects up to 30–40% of extremely preterm infants, contributing to long-term respiratory morbidity, neurodevelopmental impairment, and repeated hospitalisations. Both conditions are directly linked to uncontrolled oxygen exposure in the premature neonate — and both are preventable with evidence-based SpO2 targets and systematic screening. Understanding the mechanism, screening criteria, and management of oxygen toxicity is a non-negotiable competency for any paediatrician working in a setting where preterm infants are managed.
RECALL
Recall from physiology and biochemistry that molecular oxygen in cells is reduced to water through the electron transport chain, but a small fraction produces reactive oxygen species (ROS) — superoxide (O₂⁻), hydrogen peroxide (H₂O₂), and the highly reactive hydroxyl radical (•OH). In adults, antioxidant defences — superoxide dismutase, catalase, glutathione peroxidase, and vitamins C and E — neutralise these species. The premature infant is born with immature antioxidant systems and is therefore far more susceptible to ROS-mediated lipid peroxidation, DNA damage, and cell death when exposed to supraphysiological oxygen levels. Recall also from anatomy that retinal vascular development proceeds from the optic disc outward, reaching the nasal periphery at approximately 36 weeks gestation and the temporal periphery at term (~40 weeks). A baby born at 26 weeks has only the central retina vascularised — the peripheral retina is entirely avascular and at risk from oxygen-induced VEGF suppression.
Clinical Presentation: Who Gets Oxygen Toxicity and When
Oxygen toxicity in neonates is not an accident — it is a predictable consequence of immature antioxidant defences and developing organ systems exposed to supplemental oxygen in the context of preterm birth. The clinical presentations of oxygen toxicity range from subclinical retinal changes detectable only on screening to established blindness, chronic lung disease requiring home oxygen, and neurodevelopmental injury. Recognising which neonates are at risk — and ensuring that monitoring is calibrated correctly — is the first step toward prevention. It is also important to understand that oxygen toxicity is not binary: a neonate who receives slightly excessive oxygen for a short period may not develop severe disease, but cumulative exposure and the degree of immaturity determine risk. The following risk factors and clinical contexts should alert the paediatrician to institute careful SpO2 monitoring and timely ROP screening.
Primary risk factors for oxygen toxicity:
• Gestational age ≤34 weeks — the most powerful predictor; the lower the gestational age, the greater the immaturity of retinal vasculature, lung alveoli, and antioxidant defences
• Birth weight ≤1800 grams — used as a screening threshold because LBW neonates, even those born close to term, may have retinal immaturity
• Duration and intensity of supplemental oxygen exposure — total cumulative oxygen exposure, not just peak FiO₂, drives ROP and BPD risk
• Repeated episodes of hyperoxia — SpO₂ >95% in a preterm neonate on oxygen is potentially harmful
• Repeated episodes of hypoxia — paradoxically, hypoxia-hyperoxia cycling (the 'oxygen swings' common in NICU care) may be more damaging to the retina than sustained hyperoxia alone
• Other risk factors: sepsis (increases oxidative stress), blood transfusion (increases free iron available for Fenton reaction generating hydroxyl radicals), intraventricular haemorrhage, necrotising enterocolitis
Clinical contexts where oxygen toxicity is anticipated:
• Extremely and very low birth weight infants (ELBW <1000g, VLBW <1500g) admitted to the NICU
• Preterm infants receiving mechanical ventilation, CPAP, or nasal cannula oxygen
• Infants with respiratory distress syndrome (RDS) requiring surfactant and continued oxygen support
• Infants recovering from RDS who remain on oxygen beyond the first week
The classic presentation of established ROP is detected on screening — not from parental report — because Stage 1–3 ROP is asymptomatic. By the time a parent notices vision impairment, the disease may be Stage 4–5 with retinal detachment. This is why systematic screening is the only way to detect treatable ROP.
BPD manifests as an infant who cannot be weaned from oxygen and/or respiratory support at 36 weeks corrected gestational age. The lungs are chronically inflamed, fibrotic, and hyperinflated; the baby has persistent oxygen dependence, wheezing, recurrent respiratory infections, and poor weight gain.
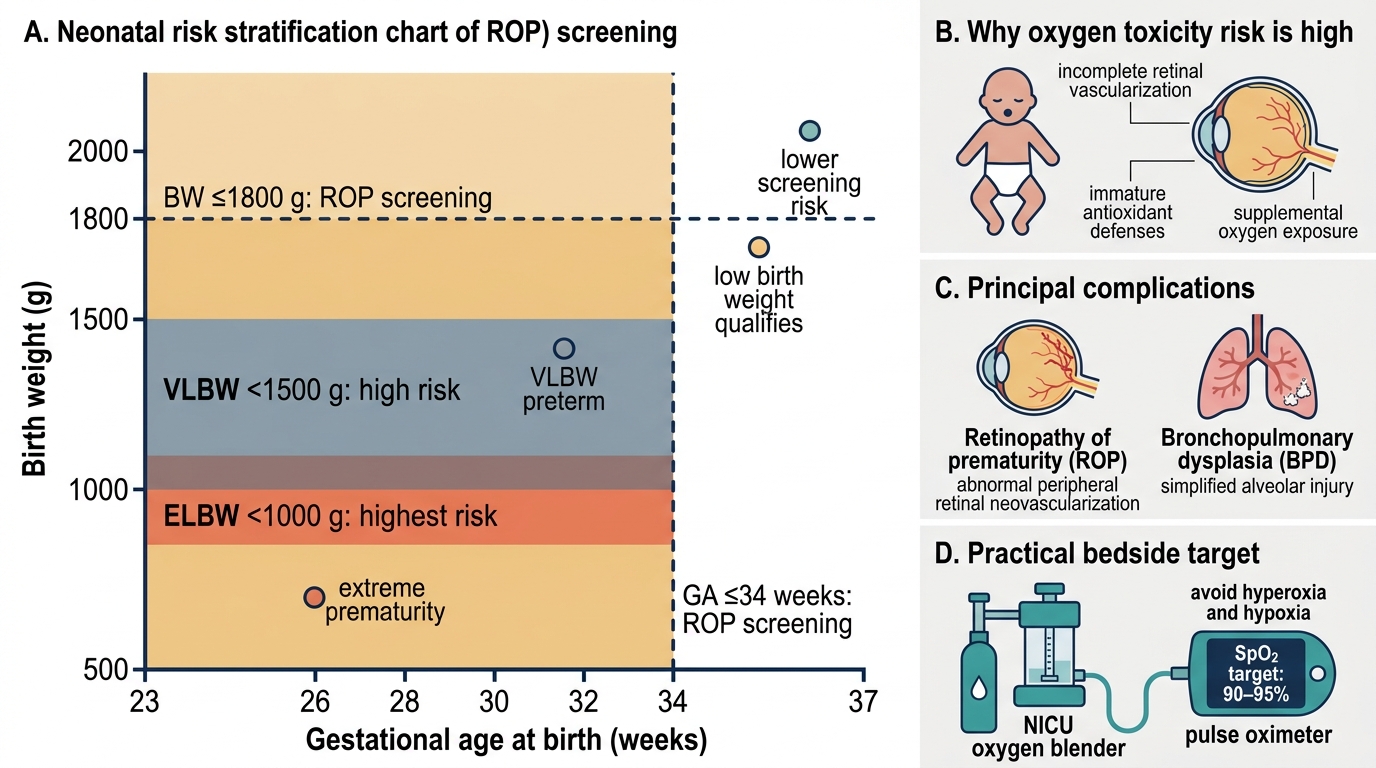
Neonatal Oxygen Toxicity Risk Stratification
Pathophysiology: How Oxygen Injures the Premature Infant
The injury from supplemental oxygen in a premature neonate operates through two distinct but interrelated mechanisms: first, free-radical-mediated oxidative injury affecting all tissues in the body; and second, a specific two-phase vascular dysregulation in the developing retina that produces retinopathy of prematurity. Understanding both mechanisms is essential because they inform the two principal preventive strategies — careful SpO2 titration (targeting 90–95%) and systematic ROP screening with prompt treatment — and together explain why oxygen must be regarded as a drug with a narrow therapeutic index in neonatal care. The free-radical mechanism is the common substrate; the two-phase retinal model is its most clinically important manifestation.
Free-radical mechanism: When a preterm neonate is exposed to FiO₂ above physiological levels, mitochondrial electron transport chain leak increases ROS production. In the absence of mature antioxidant defences, ROS cause: (1) lipid peroxidation of cell membranes → disruption of cellular integrity; (2) DNA strand breaks → apoptosis of developing neural, retinal, and pulmonary cells; (3) protein oxidation → enzyme inactivation. The lung epithelium, retinal endothelium, and intestinal mucosal cells are particularly susceptible.
ROP pathogenesis — two-phase model:
Phase 1 (hyperoxia, NICU): The premature retina normally develops its vasculature under the relatively hypoxic conditions of intrauterine life. In the NICU, supplemental oxygen suppresses hypoxia-inducible factor 1α (HIF-1α), which drives expression of vascular endothelial growth factor (VEGF). Suppressed VEGF causes regression of newly forming retinal vessels, creating a demarcation zone between the vascularised central retina and the avascular peripheral retina.
Phase 2 (relative hypoxia, as the infant matures): As the metabolically active but avascular peripheral retina continues to grow, it becomes relatively hypoxic compared to the vascularised central retina. HIF-1α is now upregulated, driving a pathological VEGF surge. This VEGF surge stimulates not orderly retinal vascularisation but chaotic, fragile extraretinal fibrovascular proliferation — vessels that grow over the retinal surface and into the vitreous. These abnormal vessels can bleed, contract, and ultimately cause tractional retinal detachment → blindness.
BPD pathogenesis: The premature lung is structurally immature — alveolar development is in the saccular stage at 24–28 weeks. Oxygen toxicity, combined with barotrauma from mechanical ventilation and volutrauma from large tidal volumes, triggers an inflammatory cascade: neutrophil recruitment → cytokine release (IL-1β, IL-8, TNF-α) → alveolar cell necrosis → fibroblast proliferation → interstitial fibrosis. The result is simplified alveolar architecture (fewer, larger alveoli), impaired gas exchange, pulmonary vascular remodelling, and pulmonary hypertension. New BPD (seen with modern surfactant era and gentle ventilation) is characterised more by arrested alveolar development than by fibrotic scarring, but oxygen toxicity remains a key contributor.
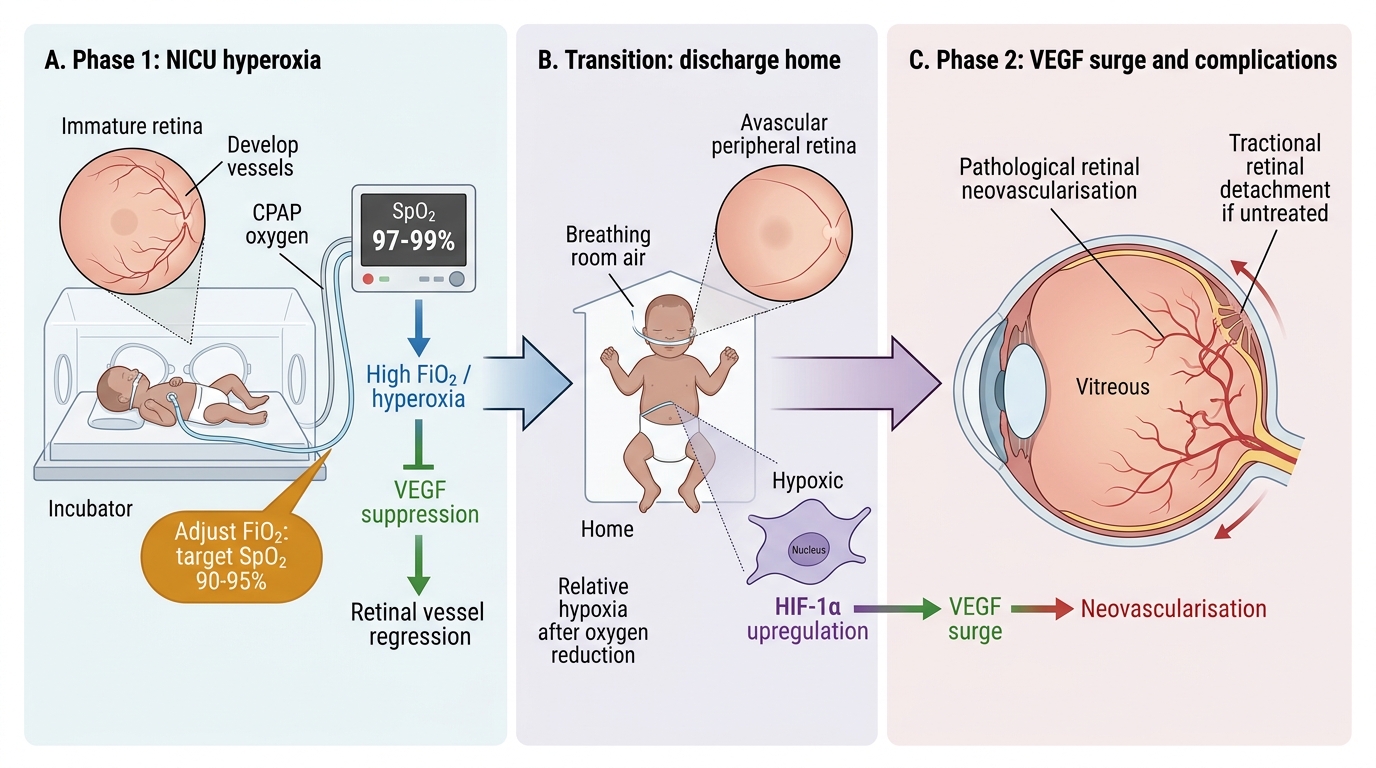
Two-Phase Pathogenesis of Retinopathy of Prematurity
SELF-CHECK
A 30-week preterm infant in the NICU has been receiving 40% oxygen via CPAP. SpO2 is consistently 97–99%. What is the most appropriate action?
A. Increase oxygen to 50% to provide a safety margin
B. Reduce FiO2 to target SpO2 90–95% as per NNF guidelines
C. Maintain current oxygen level as SpO2 >95% prevents hypoxic injury
D. Switch to room air immediately to prevent ROP
Reveal Answer
Answer: B. Reduce FiO2 to target SpO2 90–95% as per NNF guidelines
The target SpO2 for preterm neonates on supplemental oxygen is 90–95% (NNF India, AAP). Persistently elevated SpO2 of 97–99% indicates excessive oxygen delivery. Hyperoxia suppresses VEGF in the immature retina, increasing ROP risk, and generates reactive oxygen species causing lung injury (BPD). The correct action is to gradually reduce FiO2 until SpO2 is consistently within the 90–95% range. Switching abruptly to room air risks hypoxia. Increasing oxygen would worsen toxicity risk.
Diagnosis and Investigation: ROP Screening and BPD Assessment
Diagnosis of oxygen toxicity complications requires systematic, protocol-driven screening because neither ROP nor BPD announces itself with dramatic symptoms in the critical early stages — by the time a parent notices that their child cannot track light, the retina may already be detaching. BPD similarly evolves insidiously: the infant who remains oxygen-dependent at 36 weeks corrected age has been developing progressive alveolar injury for weeks. This means that the screening schedule, the serial ophthalmological examination of the preterm retina, and the monitoring of oxygen dependence at 36 weeks corrected age are the primary diagnostic tools — not symptoms reported by parents or nurses. The following section details the NNF India screening criteria, the ROP zone and stage classification, the treatment thresholds, and the BPD diagnostic criteria that allow timely intervention before irreversible injury occurs.
ROP screening — NNF India criteria (screen ALL of the following):
• Gestational age ≤34 weeks at birth, OR
• Birth weight ≤1800 grams
• Any infant >34 weeks or >1800 grams who had an unstable clinical course (prolonged oxygen requirement, sepsis, blood transfusion) — at the discretion of the treating neonatologist
Timing of first screen (NNF India): At 31 weeks corrected gestational age OR 4 weeks after birth, whichever comes later. Subsequent screens are scheduled by the ophthalmologist based on findings.
ROP Classification:
Location is described by zone (how far from the optic disc): Zone I = most posterior (centred on optic disc, radius = twice optic disc-to-fovea distance — the highest-risk zone); Zone II = extends from Zone I to nasal ora serrata; Zone III = residual temporal crescent (lowest risk).
Severity is described by stage: Stage 1 = demarcation line (flat white line separating vascular from avascular retina); Stage 2 = ridge (elevated demarcation line with height and width); Stage 3 = ridge with extraretinal fibrovascular proliferation (new vessels growing on the retinal surface or into vitreous); Stage 4a = partial retinal detachment, extrafoveal (vision may be preserved); Stage 4b = partial detachment involving the fovea (significant vision loss); Stage 5 = total retinal detachment (blindness).
Plus disease = dilatation and tortuosity of posterior pole retinal vessels (at least 2 quadrants) — indicates active, aggressive disease and upgrades severity at any zone/stage.
Aggressive Posterior ROP (AP-ROP): Formerly 'Rush disease' — rapidly progressive, Zone I or posterior Zone II, extensive plus disease without the sequential stage progression; requires urgent treatment.
Type 1 ROP (treatment threshold): Any of the following: (a) Zone I any stage with plus disease; (b) Zone I Stage 3 without plus; (c) Zone II Stage 2 or 3 with plus disease → treat with laser or anti-VEGF.
Type 2 ROP (watch and wait): Zone I Stage 1 or 2 without plus; Zone II Stage 3 without plus → close follow-up, treat if progresses to Type 1.
BPD diagnosis (Jobe and Bancalari criteria): Requirement for supplemental oxygen or respiratory support at 28 days of postnatal age (for infants <32 weeks) or at 36 weeks corrected gestational age (primary clinical benchmark). Severity graded as: mild (FiO2 <30% at 36 weeks CGA), moderate (FiO2 ≥30% or CPAP at 36 weeks), severe (positive pressure ventilation or high-flow nasal cannula at 36 weeks CGA).
Investigation in BPD: Chest X-ray shows hyperinflation, interstitial changes, and cystic lucencies. Echocardiography is essential to detect pulmonary arterial hypertension (PAH), a major complication that worsens prognosis. Blood gas shows hypercapnia and hypoxia in established disease.
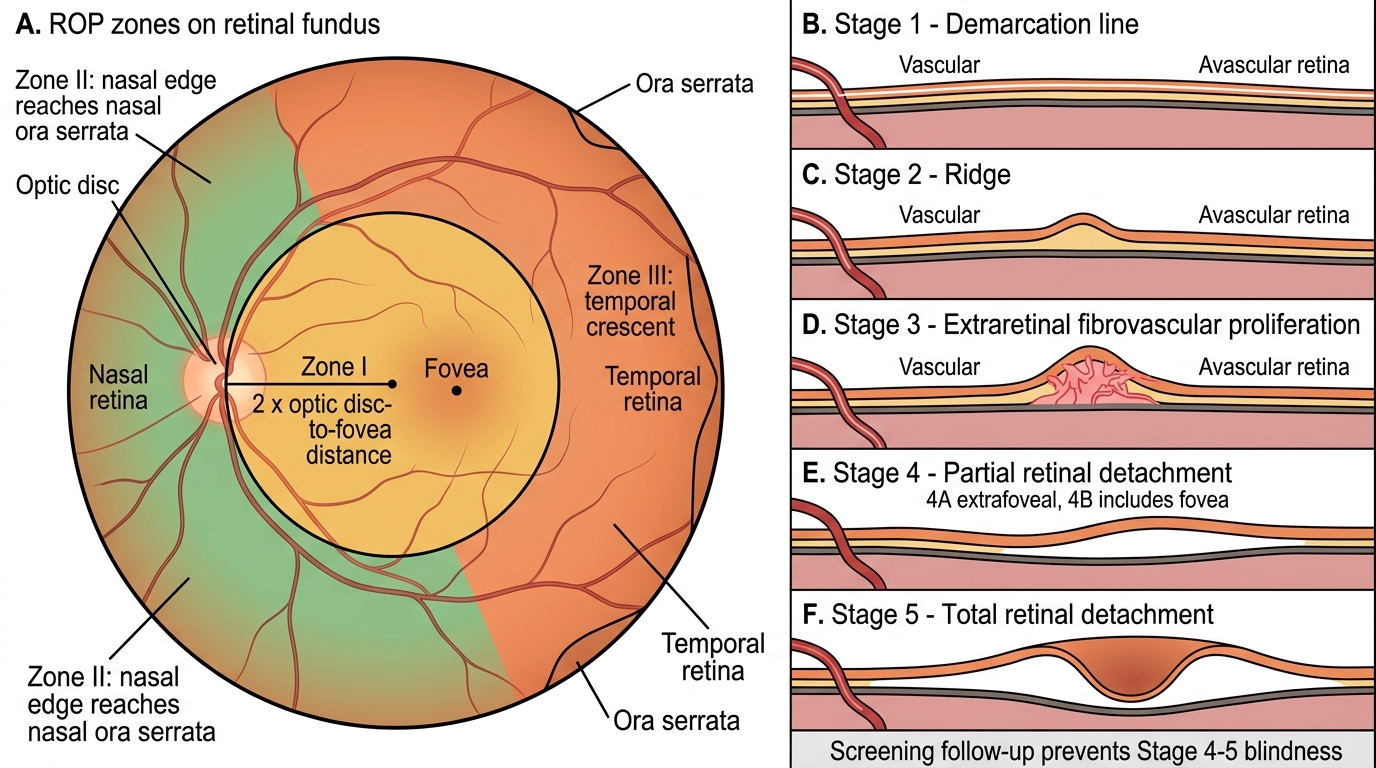
ROP Zones and Stages
CLINICAL PEARL
The most dangerous error in ROP management is missing the screening window. ROP screening requires trained paediatric ophthalmologists and indirect ophthalmoscopy with scleral depression — it cannot be done at the bedside without specialist equipment. If a premature infant is transferred from a NICU to a smaller hospital or discharged home before screening is complete, it is the paediatrician's responsibility to ensure the ophthalmology follow-up appointment is booked before discharge and documented in the referral letter. A missed screening appointment in a high-risk preterm infant can result in Stage 4–5 ROP and permanent blindness — a preventable outcome. Similarly, parents of VLBW infants must be counselled before discharge that ROP screening is a mandatory, ongoing process, not a single examination.