Page 47 of 53
PE19.17 | Oxygen Toxicity — SDL Guide (Part 2)
Management: Prevention, SpO2 Targets, ROP Treatment, and BPD Care
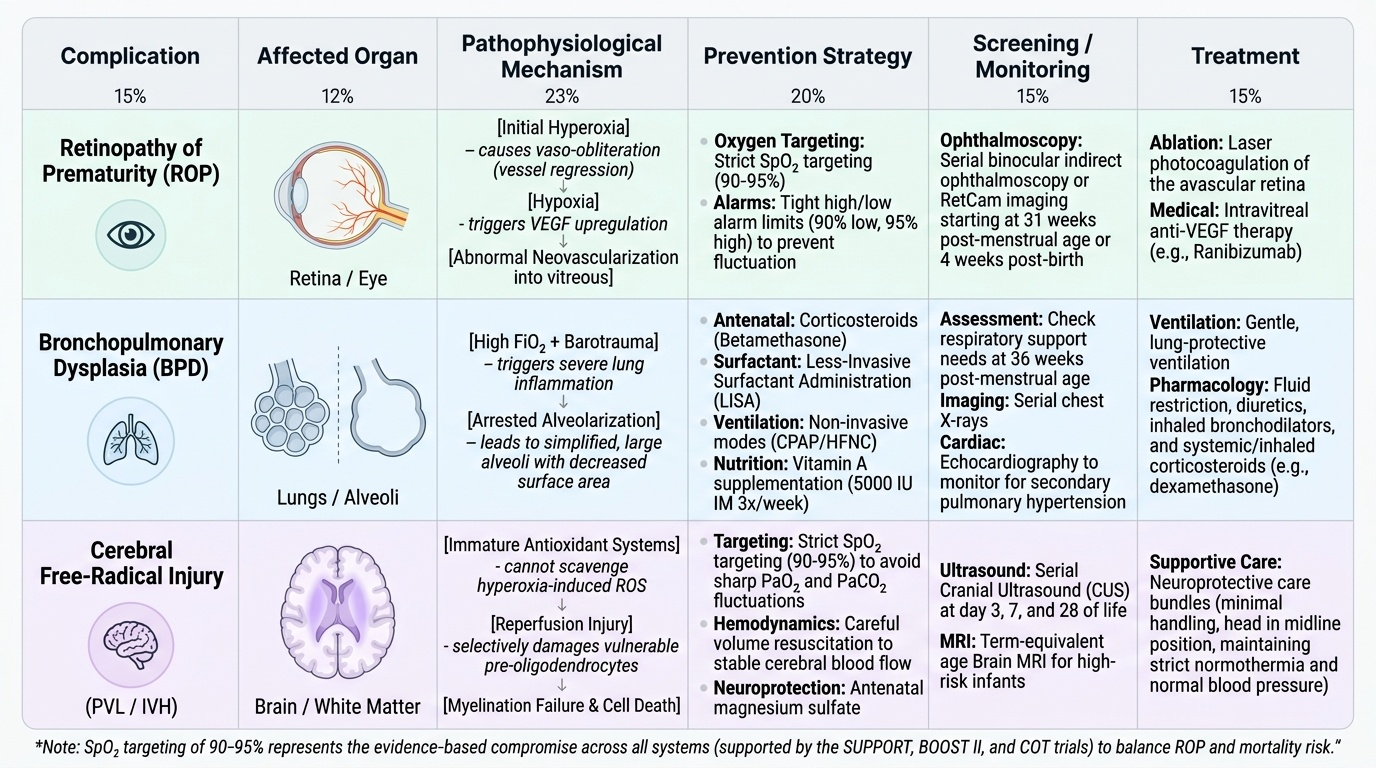
The management of oxygen toxicity in neonates operates at three levels: primary prevention through evidence-based oxygen monitoring (SpO2 targeting), treatment of established ROP to prevent blindness and preserve vision, and supportive care for the chronic lung disease of BPD including its complication of pulmonary arterial hypertension. Each level requires a different set of clinical skills, but all are within the expected scope of the general paediatrician who cares for preterm infants. The single most impactful action is correct SpO2 targeting — getting this right from day one of NICU care reduces both ROP and BPD risk before either condition has an opportunity to develop.
Primary prevention — SpO2 targeting:
The cardinal principle of oxygen therapy in preterm neonates is to use the lowest FiO2 that maintains SpO2 within the target range of 90–95%. This range was established by three landmark randomised controlled trials — SUPPORT (2010), BOOST II (2013), and COT (2013) — which enrolled preterm infants <28–32 weeks and compared SpO2 targets of 85–89% vs 91–95%. The lower target group had significantly reduced rates of ROP (confirming that oxygen drives ROP) but significantly higher mortality and increased rates of necrotising enterocolitis. The 90–95% range represents the evidence-based compromise. SpO2 >95% in a preterm neonate on supplemental oxygen must trigger a reduction in FiO₂. Pulse oximetry alarms should be set with high alarm at 95% and low alarm at 90% (with a brief desaturation limit of 88% to avoid excessive alarm fatigue from transient dips).
Provided image
Additional prevention measures include: (1) antenatal corticosteroids (betamethasone 12 mg IM × 2 doses, 24 hours apart, for mothers at risk of preterm delivery <34 weeks) to accelerate lung maturation and reduce RDS severity; (2) surfactant therapy in the delivery room (less-invasive surfactant administration, LISA) to reduce mechanical ventilation requirements; (3) non-invasive ventilation (CPAP, HFNC) preferred over intubation and mechanical ventilation to reduce barotrauma; (4) vitamin A supplementation (5000 IU IM three times weekly for 4 weeks in VLBW infants) reduces BPD risk by supporting epithelial repair.
ROP treatment:
Type 1 ROP requires treatment within 48–72 hours of identification. Two treatment modalities are available:
• Laser photocoagulation (ablation of the avascular peripheral retina): the established gold standard; performed under sedation or general anaesthesia; destroys the avascular retina that is driving VEGF production. Requires specialist facility and follow-up.
• Intravitreal anti-VEGF therapy (bevacizumab 0.625 mg, off-label): blocks the VEGF surge driving neovascularisation; particularly effective for Zone I and posterior Zone II AP-ROP where laser may not reach; induces regression but does not destroy avascular retina (vasculature may complete development over months); requires long-term ophthalmology follow-up as late reactivation can occur.
Stages 4–5: vitreoretinal surgery (vitrectomy, scleral buckling) — outcomes are poor for Stage 5 (established total detachment).
BPD management:
• Oxygen therapy: maintain SpO2 88–92% as the minimum acceptable threshold to avoid pulmonary hypertension while minimising further oxygen toxicity; wean as tolerated
• Diuretics: furosemide (1 mg/kg/dose) for pulmonary oedema; risk of electrolyte disturbance and ototoxicity
• Bronchodilators: salbutamol inhaled via spacer for bronchospasm
• Systemic corticosteroids: dexamethasone was previously used for BPD but is now restricted due to neurodevelopmental risk; inhaled budesonide is a safer option in selected cases
• Pulmonary vasodilators: sildenafil (0.5–1 mg/kg TDS, increasing to 2 mg/kg TDS) for established PAH associated with BPD; inhaled iNO in acute severe PAH
• Nutritional support: high-calorie formula (24–30 kcal/oz) as BPD babies have high caloric demands from increased work of breathing
• Home oxygen: infants with moderate-severe BPD are discharged home on supplemental oxygen; oxygen can be weaned over months as the lung grows and matures
SELF-CHECK
A 27-week preterm infant has undergone ROP screening at 31 weeks corrected age. The ophthalmologist reports Zone II, Stage 3, with plus disease. What is the correct classification and management?
A. Type 2 ROP — follow up in 2 weeks and observe
B. Type 1 ROP — treat with laser photocoagulation or anti-VEGF within 48–72 hours
C. Threshold ROP — observe for 1 week and re-screen before treatment
D. Stage 3 ROP — treat only if it progresses to Stage 4
Reveal Answer
Answer: B. Type 1 ROP — treat with laser photocoagulation or anti-VEGF within 48–72 hours
Zone II, Stage 3 WITH plus disease meets the Type 1 ROP treatment threshold (Zone II Stage 2 or 3 with plus disease = Type 1). Type 1 ROP requires treatment within 48–72 hours to prevent progression to retinal detachment. The treatment options are laser photocoagulation or intravitreal anti-VEGF (bevacizumab 0.625 mg). Waiting and observing (Type 2 management) is appropriate only for Zone I Stage 1–2 without plus, or Zone II Stage 3 without plus. Plus disease at Zone II Stage 3 is an active disease requiring urgent treatment.
SELF-CHECK
A 26-week preterm infant at 36 weeks corrected gestational age still requires FiO2 30% via CPAP. An echocardiogram shows elevated right ventricular pressure. What is the MOST likely diagnosis and an appropriate treatment?
A. Physiological oxygen requirement at term — wean oxygen over 2 weeks
B. Moderate bronchopulmonary dysplasia with pulmonary arterial hypertension — add sildenafil and nutritional support
C. Patent ductus arteriosus — close with ibuprofen
D. Residual RDS — repeat surfactant therapy
Reveal Answer
Answer: B. Moderate bronchopulmonary dysplasia with pulmonary arterial hypertension — add sildenafil and nutritional support
Oxygen requirement (FiO2 ≥30%) at 36 weeks corrected gestational age in a preterm infant = moderate BPD (Jobe and Bancalari criteria). Elevated right ventricular pressure on echo indicates pulmonary arterial hypertension (PAH), a recognised complication of BPD. Sildenafil (phosphodiesterase-5 inhibitor, 0.5–2 mg/kg TDS) is the primary pulmonary vasodilator for PAH in BPD; high-calorie nutritional support addresses the increased metabolic demand. PDA closure with ibuprofen is used earlier in the course (first weeks) and does not address PAH. Repeat surfactant is not effective for BPD — the pathology is fibrotic, not surfactant-deficient.
Self-Assessment: Oxygen Toxicity
This self-assessment section draws together the risk factors, pathophysiology, diagnostic classification, and management principles covered in this module. As you work through the scenarios, consider both the immediate clinical decision (which SpO2 to target, when to screen, when to treat ROP) and the long-term trajectory of the preterm infant at risk for oxygen toxicity. These patients require care that spans the NICU stay, discharge, and months of outpatient follow-up — and the paediatrician's role in that continuum is to ensure that no screening is missed, no SpO2 target is violated, and no intervention is delayed when the treatment threshold is reached. In settings where dedicated neonatologists are not available, the general paediatrician is the last line of defence against preventable childhood blindness and chronic lung disease. The core principles below serve as a structured self-check before you attempt the micro-quiz questions.
Provided image
Core principles to consolidate before the micro-quiz sections:
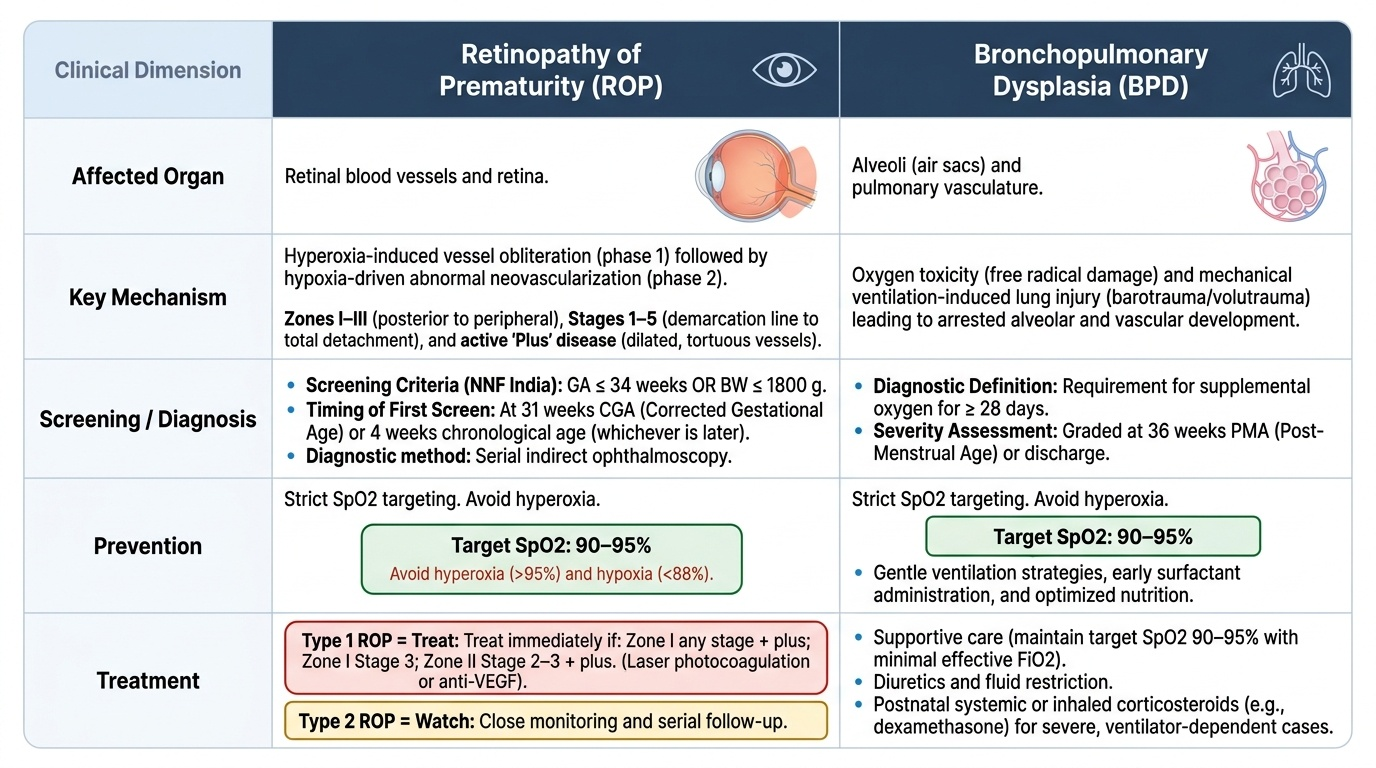
1. SpO2 90–95% is the evidence-based target for preterm neonates on supplemental oxygen — both hyperoxia (>95%) and hypoxia (<88%) cause harm; the 90–95% range balances ROP/BPD prevention against mortality from hypoxia (SUPPORT/BOOST II/COT trials)
2. ROP screening criteria (NNF India): GA ≤34 weeks OR BW ≤1800g; first screen at 31 weeks CGA or 4 weeks chronological age (whichever is later)
3. ROP zones I–III (posterior to peripheral) and stages 1–5 (demarcation line to total detachment); plus disease = active, aggressive disease
4. Type 1 ROP = treat (Zone I any stage + plus, Zone I Stage 3, Zone II Stage 2–3 + plus); Type 2 ROP = watch
5. BPD = oxygen requirement at 36 weeks CGA (mild <30% FiO2, moderate ≥30%/CPAP, severe = PPV); echocardiogram for PAH; sildenafil for PAH; nutritional support; home oxygen for moderate-severe
6. Prevention: antenatal steroids + surfactant + non-invasive ventilation + SpO2 monitoring + vitamin A in VLBW
Identify and reflect on the single most important action you would take in your future clinical practice to prevent a preterm infant under your care from developing preventable blindness from ROP.