Page 1 of 16
PE15.1 | Fluid Requirements — SDL Guide
Learning Objectives
- Describe the distribution of body fluid compartments in infants, children, and adults
- Calculate maintenance fluid requirements using the Holliday-Segar method
- Assess the degree of dehydration using IMNCI clinical criteria
- Outline the principles of oral rehydration therapy (ORT) and intravenous fluid management in dehydration
INSTRUCTIONS
Fluid and electrolyte balance is one of the most fundamental and clinically critical areas in paediatric practice. Children — especially infants — have a high body water content and a proportionally large surface area, making them uniquely vulnerable to rapid fluid loss and severe dehydration. A thorough understanding of maintenance fluid calculation and dehydration assessment is essential for every doctor managing children. This module builds directly on your knowledge of renal physiology and osmotic regulation from pre-clinical years and applies it to the bedside.
References
- Ghai Essential Pediatrics, 9th ed, Ch 18 (Fluid and Electrolyte Disturbances) (textbook)
- Nelson Textbook of Pediatrics, 21st ed, Ch 68 (Maintenance and Replacement Therapy) (textbook)
- WHO/UNICEF IMNCI Chart Booklet — Management of the Sick Child (2014) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-month-old girl is brought to the outpatient department by her mother after three days of watery diarrhoea and vomiting. She weighs 9 kg. On examination she is irritable, her eyes are mildly sunken, her mouth and tongue are dry, and her skin pinch goes back slowly — in about 2 seconds. Her respiratory rate is 38 per minute. The house officer is asked to prescribe her fluids. How much fluid does this child need, and by which route?
WHY THIS MATTERS
Diarrhoeal disease remains one of the leading causes of under-five mortality in India and globally, and the overwhelming majority of these deaths are caused by dehydration that is either unrecognised or incorrectly treated. The Holliday-Segar formula, developed in 1957, gives every clinician a rapid, evidence-based method to calculate how much fluid a child needs per day merely by knowing their weight. Paired with the IMNCI dehydration-assessment framework, which classifies children into three actionable severity groups (no/some/severe dehydration), these tools form the backbone of paediatric fluid management in both primary and referral care settings across India. Understanding these principles not only saves lives but is a core competency expected of every graduate.
RECALL
Before reading further, recall from your pre-clinical studies: (1) What are the major body fluid compartments? (2) What determines the osmolality of plasma, and which organ is primarily responsible for regulating water balance? (3) What is the glomerular filtration rate in a healthy child, and how does the kidney respond to dehydration via antidiuretic hormone (ADH)? Revisiting these concepts will help you understand why children lose water more rapidly than adults and why the choice of replacement fluid matters.
Body Fluid Compartments and Distribution in Children
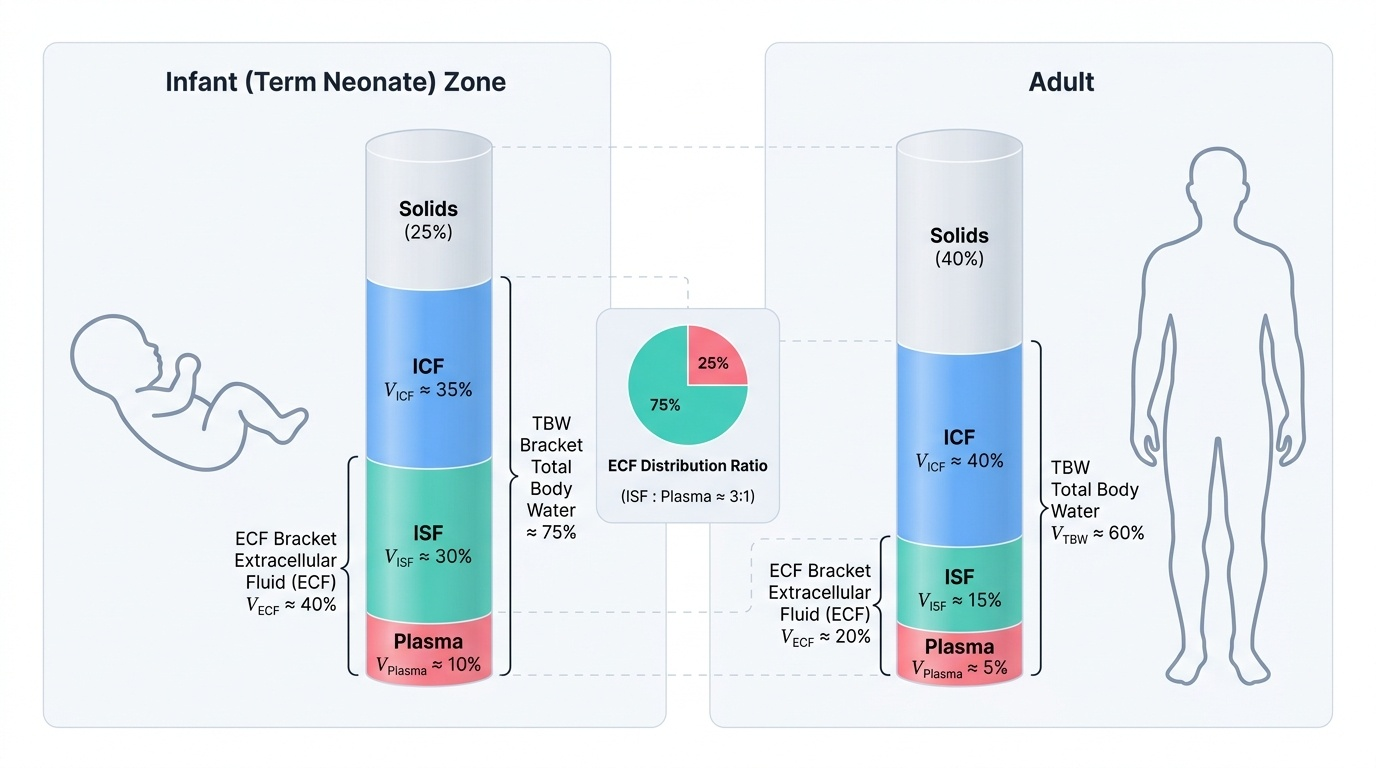
Total body water (TBW) makes up a greater proportion of body mass in children than in adults, and this proportion decreases progressively with age. A premature neonate may have TBW as high as 85% of body weight; a term neonate has approximately 75-80%; by one year of age TBW is around 70%; and by adulthood it has fallen to approximately 60% in males and 55% in females. This higher water content in young children is predominantly in the extracellular fluid (ECF) compartment, which constitutes roughly 40-45% of body weight in neonates (compared with 20-25% in adults). As a result, the absolute ECF volume per kilogram of body weight is much larger in infants, and when fluid is lost, the ECF depletes more rapidly.
Provided image
The intracellular fluid (ICF) compartment contains approximately 30-40% of body weight in neonates, rising toward the adult value of ~40% as muscle mass develops with age. Within the ECF, approximately three-quarters is interstitial fluid (bathing tissues) and one-quarter is intravascular plasma (within blood vessels). For clinical fluid management it is the ECF — particularly the plasma volume and interstitial space — that is directly affected by vomiting, diarrhoea, and inadequate intake.
The surface area-to-weight ratio is much higher in infants than in adults, which means insensible water losses (through skin and respiration) per kilogram are greater. A febrile infant may lose 10-12 mL/kg/°C above 38°C through skin, raising maintenance needs substantially. Similarly, respiratory fluid loss is proportionally higher during tachypnoea. These physiological facts explain why even a brief illness causing vomiting and diarrhoea can produce clinically significant dehydration within hours in a young infant.
- TBW as % body weight: preterm neonate ~85%, term neonate ~75-80%, 1 yr ~70%, adult ~60%
- ECF: ~40-45% body weight in neonates → ~20-25% in adults
- ICF: ~30-40% body weight in neonates → ~40% in adults
- Interstitial : plasma split: approximately 3:1 within ECF
Normal Fluid Requirements: The Holliday-Segar Method
The Holliday-Segar method, published in 1957 by Malcolm Holliday and William Segar, provides a simple weight-based formula to estimate daily maintenance fluid requirements in children. The formula is derived from the observation that, over a wide range of mammalian body sizes, caloric expenditure (and therefore water turnover) is proportional to approximately 100 kcal/kg for the first 10 kg of body weight, declining per additional kilogram as body mass increases. Since approximately 100 mL of water is required for every 100 kcal metabolised, the formula translates directly into a volume calculation.
Provided image
This method deliberately divides body weight into three zones because the relationship between metabolic rate and body size is not linear — a 30 kg child does not expend three times the calories of a 10 kg infant. As body mass increases, the metabolic rate per kilogram declines. The formula captures this by applying a higher rate per kilogram to smaller children and a progressively lower rate to each additional kilogram. Understanding this gradient helps clinicians avoid over-hydrating larger children (which can cause fluid overload and hyponatraemia) while ensuring smaller infants receive enough volume to match their higher metabolic demand.
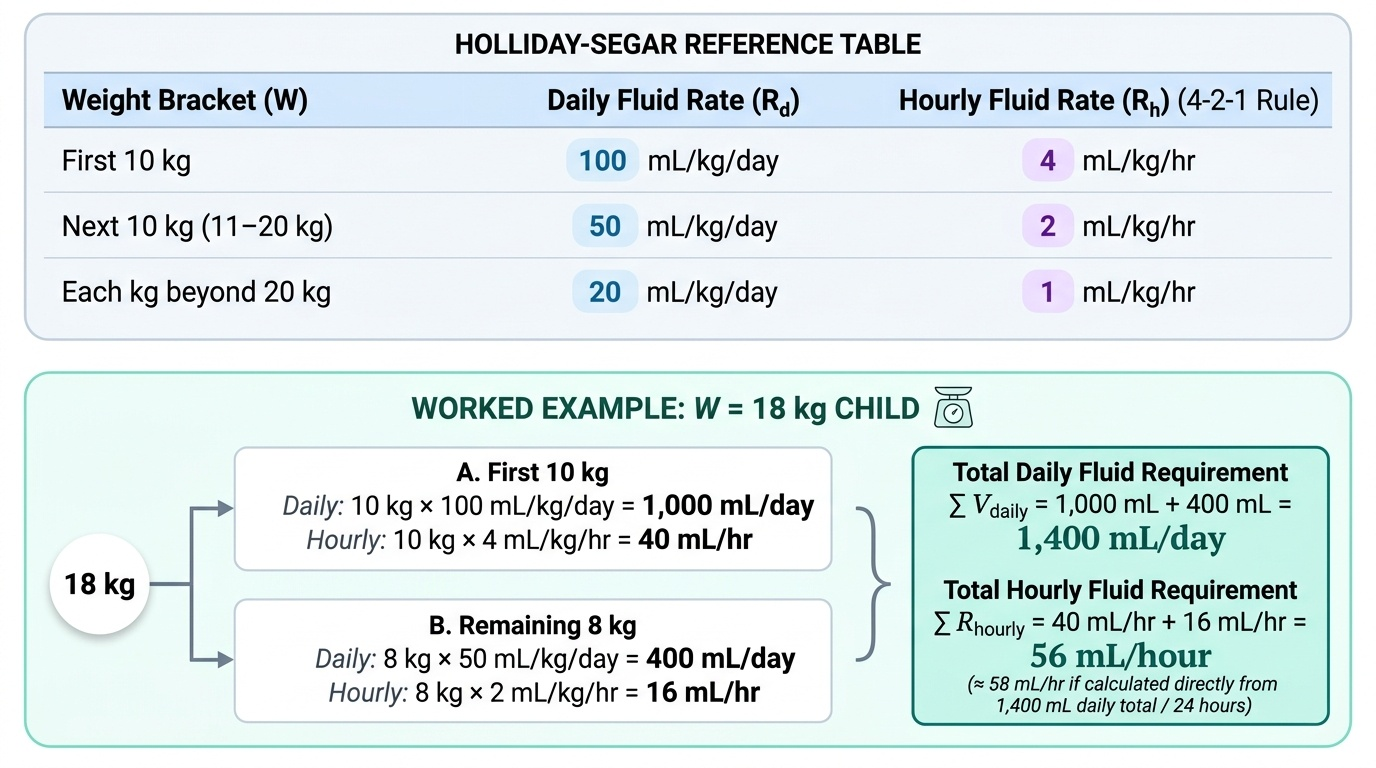
The Holliday-Segar rule states:
• First 10 kg of body weight: 100 mL/kg/day
• Next 10 kg (11–20 kg): 50 mL/kg/day
• Each kg beyond 20 kg: 20 mL/kg/day
For example, a child weighing 18 kg needs:
(10 × 100) + (8 × 50) = 1000 + 400 = 1400 mL/day (approximately 58 mL/hour).
A child weighing 25 kg needs:
(10 × 100) + (10 × 50) + (5 × 20) = 1000 + 500 + 100 = 1600 mL/day (~67 mL/hour).
It is equally useful to express the formula as a hourly rate (the 4-2-1 rule): 4 mL/kg/hr for the first 10 kg, 2 mL/kg/hr for the next 10 kg, and 1 mL/kg/hr for each kg beyond 20 kg. Both forms yield identical totals — the 4-2-1 rule is particularly useful when prescribing IV infusions.
Important clinical caveats: the Holliday-Segar formula gives baseline maintenance for a healthy, afebrile child at rest. It must be adjusted upward for fever (add ~10% per degree C above 38°C), tachypnoea, surgical losses, burns, or any state of increased insensible loss. It is used for maintenance only — fluid deficits from prior dehydration must be calculated separately and added to the daily requirement.
SELF-CHECK
A 12-month-old child weighs 10 kg. Using the Holliday-Segar method, what is the correct daily maintenance fluid requirement?
A. 500 mL/day
B. 750 mL/day
C. 1000 mL/day
D. 1200 mL/day
Reveal Answer
Answer: C. 1000 mL/day
For the first 10 kg, the Holliday-Segar formula gives 100 mL/kg/day. For a 10 kg child: 10 × 100 = 1000 mL/day. The formula allocates 50 mL/kg/day only for the next 10 kg (11-20 kg), which does not apply here. Answer: 1000 mL/day.
Assessing Dehydration in Children: IMNCI Framework
When a child loses more fluid than is replaced — through diarrhoea, vomiting, poor intake, increased insensible losses (fever, tachypnoea), or any combination — dehydration develops. The severity of dehydration reflects the fraction of body weight lost as water, and different severities carry different risks, requiring different management pathways. The IMNCI (Integrated Management of Neonatal and Childhood Illness) framework, recommended by WHO and adopted across India, classifies dehydration into three categories based on clinical signs, each linked to a treatment plan.
Provided image
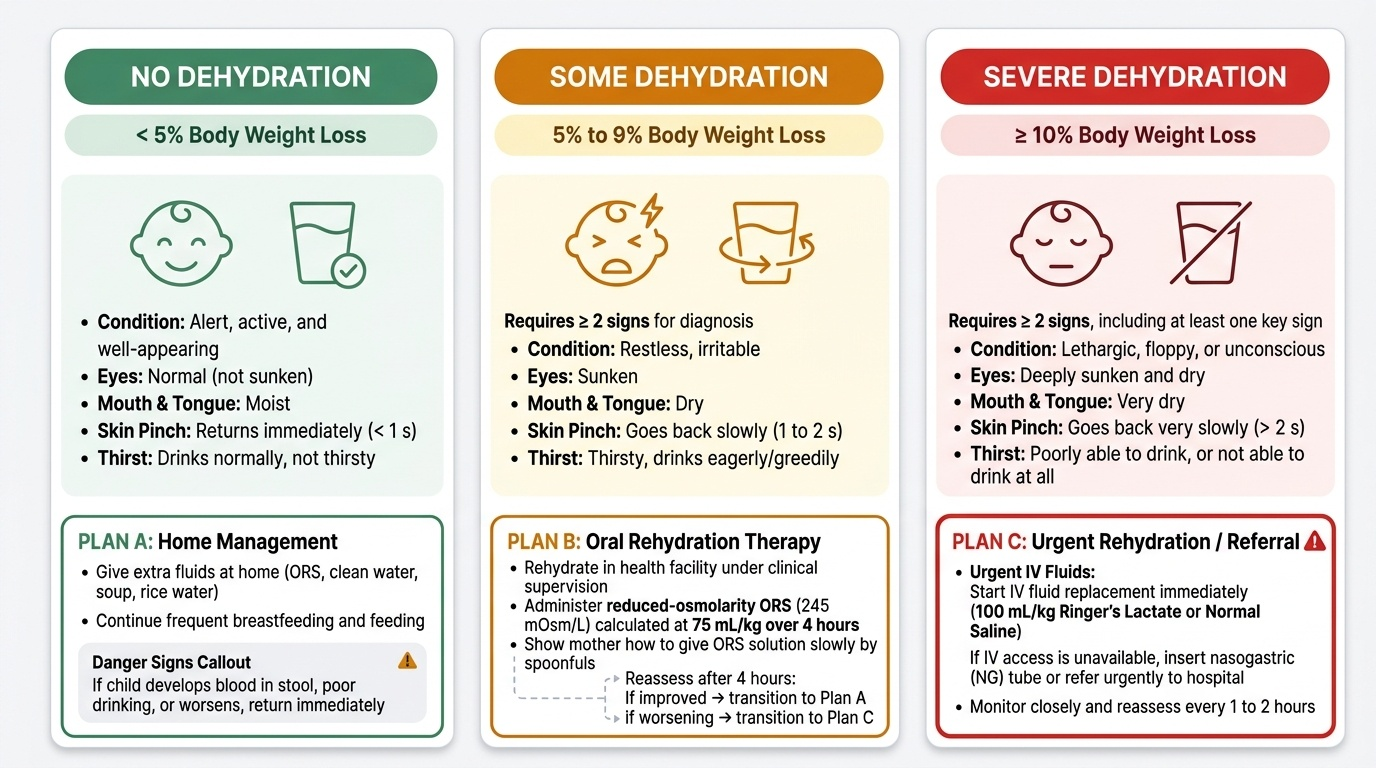
No dehydration (< 5% body weight loss): The child is alert and appears well. There are no or minimal signs of fluid deficit — no sunken eyes, moist mouth, skin pinch returns immediately (< 1 second). The child drinks normally. Management: continued feeding plus IMNCI Plan A — give extra fluids at home (ORS + food), advise mother on danger signs, return if worsens.
Some dehydration (5-9% body weight loss): Two or more of the following signs are present — restlessness or irritability, sunken eyes, thirsty / drinks eagerly, skin pinch goes back slowly (1-2 seconds). Management: IMNCI Plan B — oral rehydration in a supervised health facility using reduced-osmolarity ORS (osmolarity 245 mOsm/L) at 75 mL/kg over 4 hours, reassess, then discharge with Plan A if improving.
Severe dehydration (≥ 10% body weight loss): Abnormal drowsiness or unconsciousness, inability to drink, very sunken and dry eyes, very sunken fontanelle, skin pinch goes back very slowly (> 2 seconds). Management: IMNCI Plan C — immediate IV fluid resuscitation (Ringer's lactate 100 mL/kg over 3-6 hours depending on age), hospitalise, close monitoring.
Key clinical point: the skin pinch (also called skin turgor) is one of the most reliable signs of moderate-to-severe dehydration — the skin is lifted between two fingers over the abdominal wall and released; a return time of 1-2 seconds (slowly) indicates some dehydration; > 2 seconds (very slowly) indicates severe dehydration. Skin turgor may be misleadingly poor in severe malnutrition and is less reliable in obesity or hypernatraemic dehydration.
- No dehydration → Plan A (home care, extra ORS)
- Some dehydration → Plan B (ORS 75 mL/kg over 4 h at facility)
- Severe dehydration → Plan C (IV RL + hospitalisation)
SELF-CHECK
A 9-month-old child has had diarrhoea for 2 days. On examination: irritable, sunken eyes, skin pinch returns in about 2 seconds, drinking eagerly. According to IMNCI, what is the correct classification?
A. No dehydration — Plan A
B. Some dehydration — Plan B
C. Severe dehydration — Plan C
D. Hypernatraemic dehydration — special protocol
Reveal Answer
Answer: B. Some dehydration — Plan B
This child has two or more signs of some dehydration: irritability, sunken eyes, skin pinch going back slowly (1-2 seconds), and eagerly drinking. This is IMNCI classification 'some dehydration', requiring Plan B — supervised oral rehydration with reduced-osmolarity ORS 75 mL/kg over 4 hours at a health facility.