Page 2 of 16
PE15.1 | Fluid Requirements — SDL Guide (Part 2)
Oral Rehydration and IV Fluid Therapy: Clinical Application
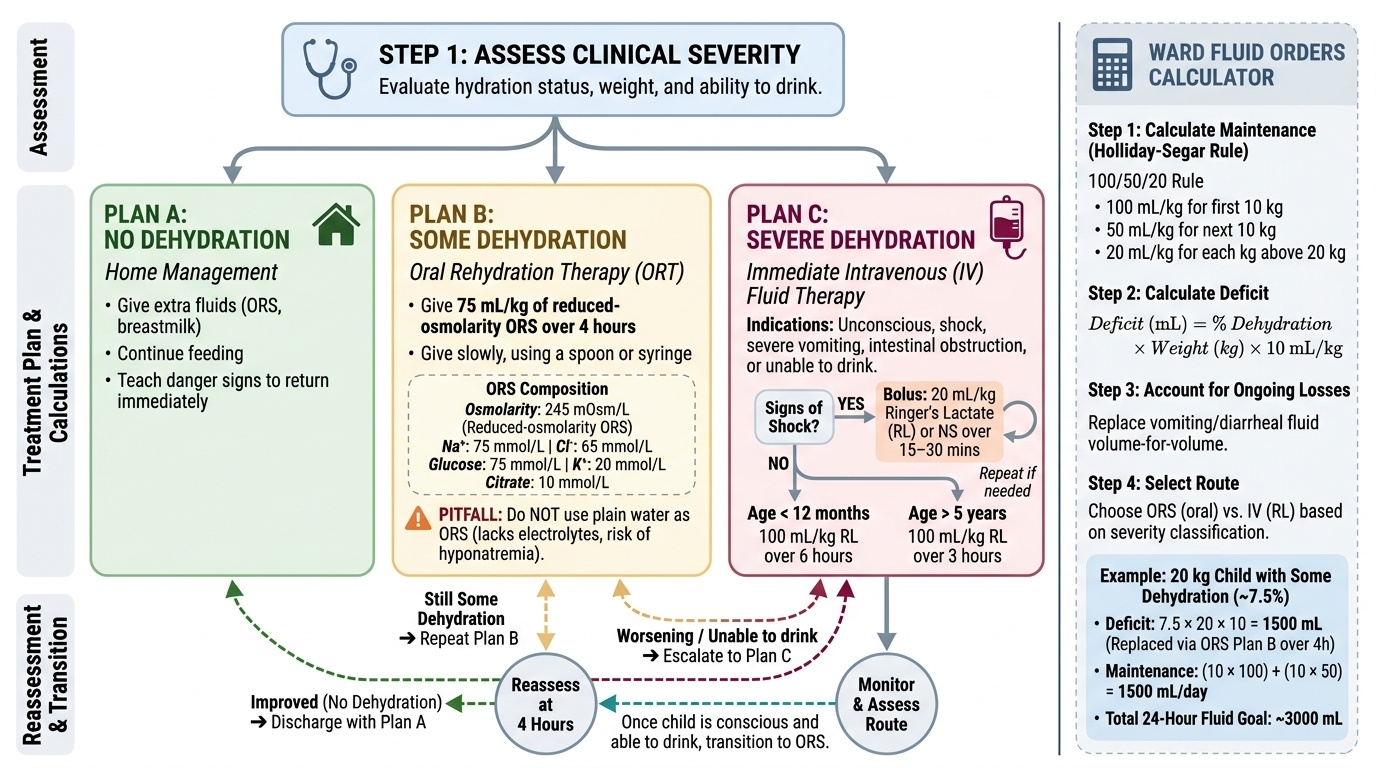
Effective fluid management in a dehydrated child combines two components: replacing the deficit (the water and electrolytes already lost) and providing ongoing maintenance fluids (what the child needs to sustain normal physiology going forward). In addition, any ongoing losses (continued diarrhoea or vomiting) must be replaced volume-for-volume.
Provided image
Oral rehydration therapy (ORT) with reduced-osmolarity ORS (Na⁺ 75 mmol/L, Cl⁻ 65 mmol/L, glucose 75 mmol/L, K⁺ 20 mmol/L, citrate 10 mmol/L; total osmolarity 245 mOsm/L) is the cornerstone of management for children with no or some dehydration. Multiple large WHO-coordinated trials demonstrated that reduced-osmolarity ORS (compared with the older standard ORS of 311 mOsm/L) reduced stool output by ~20% and vomiting episodes significantly in children with acute watery diarrhoea, without increasing the risk of hyponatraemia. For Plan B (some dehydration): give 75 mL/kg of ORS over 4 hours; reassess at the end. If the child has improved and can be classified as no dehydration, discharge with Plan A. If still some dehydration, repeat Plan B. If worsening or unable to drink, escalate to Plan C.
Intravenous fluid therapy is indicated when oral hydration is not possible (unconscious, shock, severe vomiting, intestinal obstruction) or in severe dehydration (Plan C). The preferred IV solution is Ringer's lactate (RL). The WHO recommends for Plan C in children over 5 years: 100 mL/kg RL over 3 hours; for children under 12 months: 100 mL/kg RL over 6 hours. In shock, a bolus of 20 mL/kg RL (or normal saline) is given over 15-30 minutes and may be repeated. Once the child can drink, transition to ORS.
For calculating total fluid orders on a ward:
1. Calculate maintenance using Holliday-Segar (100/50/20 rule)
2. Calculate the deficit (% dehydration × weight in kg × 10 mL/kg)
3. Add ongoing losses if measurable
4. Choose the appropriate route (oral vs IV) based on dehydration severity
For example: A 20 kg child with some dehydration (~7.5%): deficit = 7.5 × 20 × 10 = 1500 mL; maintenance = (10×100)+(10×50) = 1500 mL/day; total over 24 h ≈ 3000 mL, with the deficit replaced preferably as ORS Plan B (75 mL/kg = 1500 mL over 4 h at facility) and maintenance continued.
Common pitfalls to avoid: do NOT use plain water as ORS — it lacks electrolytes and worsens hyponatraemia. Do NOT restrict oral fluids during diarrhoea — continued feeding and extra ORS reduces duration of illness and malnutrition. Do NOT use hypotonic IV fluids (e.g., 0.18% NaCl in 4% dextrose) as a first-line resuscitation fluid — it risks hyponatraemia and cerebral oedema.
SELF-CHECK
A 2-year-old child weighing 12 kg has some dehydration. What volume of reduced-osmolarity ORS should be given over 4 hours under IMNCI Plan B?
A. 600 mL over 4 hours
B. 900 mL over 4 hours
C. 1200 mL over 4 hours
D. 1500 mL over 4 hours
Reveal Answer
Answer: B. 900 mL over 4 hours
IMNCI Plan B prescribes 75 mL/kg of ORS over 4 hours. For a 12 kg child: 75 × 12 = 900 mL over 4 hours. This is given at a supervised health facility with reassessment at the end of the 4-hour period.
Self-Assessment: Fluids in Paediatric Practice
Having studied body fluid physiology, the Holliday-Segar maintenance formula, IMNCI dehydration assessment, and the principles of oral and intravenous rehydration, you are now equipped to apply these concepts to a realistic clinical scenario. Working through the questions below — before looking at the answers — consolidates all four areas into a single integrated reasoning exercise. Paediatric fluid management is a skill that becomes fluent only through repetition; every child with diarrhoea or poor intake in your ward is an opportunity to practise this calculation cycle. Work through each step methodically.
A 3-year-old boy weighing 14 kg is brought with two days of diarrhoea. He is irritable, his eyes are sunken, his mouth is dry, and his skin pinch returns in about 2 seconds. He cries without tears and is drinking eagerly.
Questions to answer:
1. What is his IMNCI dehydration classification?
2. What is the appropriate management plan?
3. Calculate his 4-hour ORS requirement under Plan B.
4. Calculate his daily maintenance fluid requirement (Holliday-Segar).
5. What electrolyte-containing fluid would you use, and why?
Worked answers:
1. Some dehydration — he has ≥2 signs: irritability, sunken eyes, skin pinch 1-2 seconds (slowly), drinking eagerly.
2. Plan B — supervised ORS at a health facility over 4 hours.
3. ORS = 75 mL/kg × 14 kg = 1050 mL over 4 hours; reassess and discharge with Plan A if improved.
4. Maintenance = (10 × 100) + (4 × 50) = 1000 + 200 = 1200 mL/day (50 mL/hour).
5. Reduced-osmolarity ORS (245 mOsm/L) — this formulation reduces stool output and vomiting better than standard ORS and is the WHO/IAP recommended solution for acute diarrhoea in children.
CLINICAL PEARL
The 4-2-1 rule for hourly IV maintenance: 4 mL/kg/hr for first 10 kg + 2 mL/kg/hr for next 10 kg + 1 mL/kg/hr per kg beyond 20 kg. This equals the Holliday-Segar daily total divided by 24. Use whichever form suits the setting — daily total for oral planning, hourly rate for IV pump orders. Remember: Holliday-Segar is for MAINTENANCE only. Deficit and ongoing losses are calculated separately and added. A common error is to prescribe only maintenance for a moderately dehydrated child and wonder why they don't improve.