Page 1 of 30
PE20.1 | Urinary Tract Infection — SDL Guide
Learning Objectives
- Enumerate the common aetiological agents and pathogenetic mechanisms of UTI in children across age groups
- Describe the age-specific clinical presentation of UTI from neonates to school-age children
- Outline the appropriate diagnostic approach including urine collection methods, bacteriological criteria, and risk-stratified imaging protocol
- Plan antibiotic management by age and severity, and identify indications for prophylaxis and surgical referral
- Recognise the complications of UTI — renal scarring, hypertension, and chronic kidney disease — and the role of early treatment in prevention
INSTRUCTIONS
Urinary tract infection is the most common serious bacterial infection in young children and a leading preventable cause of acquired renal scarring. Because symptoms are non-specific in infants, the diagnosis demands a high index of suspicion and meticulous urine collection. This module builds the diagnostic and therapeutic framework you will use every time you encounter a febrile child without an obvious focus — a scenario encountered daily in paediatric wards and outpatient practice.
References
- Ghai Essential Pediatrics, 9th edition, Ch 18 — Nephrology (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 553 — UTI (textbook)
- IAP Standard Treatment Guidelines — Urinary Tract Infection in Children (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-month-old girl is brought with a 3-day history of fever (temperature 39.2°C), poor feeding, and two episodes of vomiting. There is no cough, rash, or ear discharge. The anterior fontanelle is normotensive and the throat is clear. On urine dipstick you detect leucocyte esterase 2+ and nitrites positive. You send a catheter-specimen urine for culture. While awaiting the result, the parents ask: 'Why does a baby this young get a urine infection? Can it damage her kidneys permanently?' How would you answer?
WHY THIS MATTERS
Urinary tract infection (UTI) accounts for approximately 7–8% of all febrile episodes in infants under 2 years and is the commonest serious bacterial infection in this age group after septicaemia and pneumonia. Its clinical significance extends far beyond the acute episode: up to 15% of children who sustain pyelonephritis develop permanent renal scarring, and children with untreated high-grade vesicoureteric reflux (VUR) face a risk of hypertension and chronic kidney disease in adulthood. Because symptoms in infants are entirely non-specific — fever, vomiting, poor feeding — the diagnosis is frequently delayed. Understanding UTI from aetiology through imaging to long-term follow-up is therefore a core competency that directly protects kidney health across a patient's lifetime.
RECALL
Before proceeding, recall the following from your Anatomy and Physiology modules:
- Renal anatomy: the ureter enters the bladder at the vesicoureteric junction (VUJ) at an oblique angle, forming a functional one-way valve. When this valve is incompetent — as in VUR — urine refluxes under pressure towards the renal pelvis and parenchyma.
- Voiding physiology: bladder filling and voiding are coordinated by the pontine micturition centre. Dysfunctional voiding (incomplete emptying, high post-void residual) creates stagnant urine — an ideal culture medium.
- Female anatomy: the shorter female urethra (∼4 cm in adults; proportionally shorter in girls) provides a significantly easier ascent pathway for periurethral flora than the male urethra.
- Urine as a culture medium: urine is normally sterile. Its pH, osmolarity, and organic acid content inhibit bacterial growth to some degree, but stagnant, alkaline, or dilute urine facilitates colonisation.
Clinical Presentation of UTI in Children
The presentation of UTI in children is strikingly age-dependent, and this age-dependence is one of the most clinically important facts about the condition. In the neonate and young infant (< 3 months), symptoms are entirely non-specific: fever without focus, hypothermia, poor feeding, irritability, prolonged neonatal jaundice, or frank sepsis. Classic urinary symptoms such as dysuria and frequency cannot be elicited at this age. In infants aged 3 months to 2 years, fever without a source is the cardinal feature; accompanying symptoms may include vomiting, diarrhoea, abdominal pain, and crying on micturition — though none are diagnostic. In children over 2 years, the presentation begins to resemble adult UTI: cystitis (lower UTI) presents with dysuria, frequency, urgency, haematuria, and suprapubic discomfort, while pyelonephritis (upper UTI) adds systemic features — high fever (≥38°C), rigors, loin pain or tenderness, and vomiting. The clinically critical distinction is between lower UTI (confined to the bladder and urethra) and upper UTI / pyelonephritis (involving the renal parenchyma), because pyelonephritis drives the risk of permanent scarring and systemic sepsis.
| Age Group | Predominant Symptoms | Upper vs Lower UTI clue |
|---|---|---|
| Neonate (<1 month) | Fever, jaundice, poor feeding, sepsis | Almost always upper UTI / urosepsis |
| Infant 1–24 months | Fever without source, vomiting, irritability | Fever ≥38°C + pyuria suggests pyelonephritis |
| Child 2–5 years | Abdominal pain, vomiting ± dysuria | Fever + loin tenderness → pyelonephritis |
| Older child (>5 yr) | Dysuria, frequency, urgency, haematuria | Cystitis pattern common; fever → upper UTI |
Physical examination should document temperature (fever ≥38°C in a non-toxic infant is the most sensitive pointer to UTI among laboratory tests), abdominal palpation for loin tenderness, and assessment of the external genitalia for phimosis (males) and labial adhesions (females) — both anatomical factors predisposing to UTI.
Pathophysiology and Aetiology
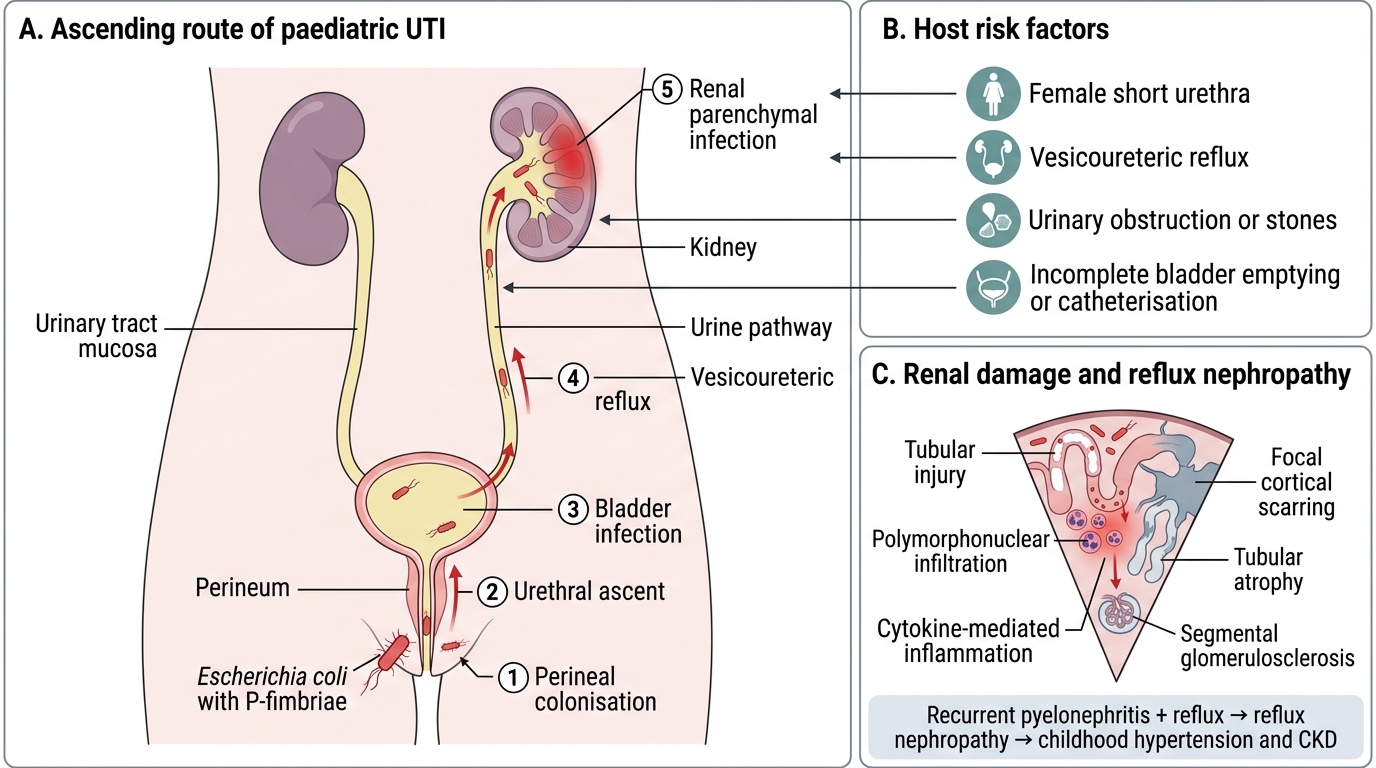
The great majority of UTIs in children arise by the ascending route: bacteria colonising the perineum and periurethral area ascend through the urethra into the bladder, and in the presence of vesicoureteric reflux (VUR) or other structural anomaly, continue upward into the renal pelvis and parenchyma. This ascending pathway explains both the female preponderance (shorter urethra) and the central role of anatomical risk factors.
Aetiological agents: Escherichia coli is responsible for approximately 80% of all paediatric UTIs. Its key virulence factors include type 1 and P-fimbriae (pili) that allow binding to uroepithelial cells, haemolysin production, aerobactin-mediated iron acquisition, and resistance to complement-mediated serum killing. Other organisms in decreasing order of frequency include Klebsiella pneumoniae, Proteus mirabilis (associated with struvite stones), Enterococcus faecalis, Pseudomonas aeruginosa (nosocomial or structural abnormality), and Staphylococcus saprophyticus (adolescent females). In neonates, group B Streptococcus and Staphylococcus aureus may cause haematogenous UTI.
Host and structural risk factors that predispose to UTI include:
• VUR — graded I–V; grades III–V are associated with the highest risk of ascending infection and renal scarring.
• Obstructive uropathy — pelviureteric junction (PUJ) obstruction, posterior urethral valves (PUV) in boys, ureterocele.
• Dysfunctional elimination syndrome — constipation + infrequent voiding + voiding dysfunction (a common, underdiagnosed triad).
• Phimosis in uncircumcised males: the relative risk of UTI in uncircumcised infant boys is 5–10× that of circumcised boys.
• Urinary catheterisation — catheter-associated UTI (CAUTI) is an important nosocomial risk.
• Immune compromise — chemotherapy, steroid therapy, HIV.
Ascending Route of Paediatric UTI and Reflux Nephropathy
Once bacteria reach the renal parenchyma, the host inflammatory response (polymorphonuclear infiltration, cytokine storm) triggers tubular cell damage and, with repetitive infection, focal cortical scarring (segmental glomerulosclerosis and tubular atrophy). This is the mechanism underlying reflux nephropathy, the commonest acquired cause of hypertension and CKD in children.
SELF-CHECK
Which organism is responsible for approximately 80% of urinary tract infections in children?
A. Klebsiella pneumoniae
B. Escherichia coli
C. Proteus mirabilis
D. Enterococcus faecalis
Reveal Answer
Answer: B. Escherichia coli
E. coli accounts for ~80% of paediatric UTIs. Its P-fimbriae allow adhesion to uroepithelial cells, facilitating colonisation and ascent. Klebsiella is the second commonest, while Proteus is associated with struvite stones due to its urease activity.
Diagnosis and Investigation
Accurate diagnosis of UTI in children rests on two inseparable pillars: meticulous urine collection and bacteriological confirmation by culture. No clinical feature, symptom score, or rapid dipstick result alone is sufficient to diagnose UTI in a young child — each carries a meaningful false-positive and false-negative rate. The stakes are high: an over-diagnosed UTI leads to unnecessary antibiotics and missed alternative diagnoses, while an under-diagnosed or under-treated UTI in an infant may result in urosepsis or permanent renal scarring. The diagnostic approach must therefore be systematic, beginning with the collection method most likely to yield an uncontaminated sample, followed by culture to confirm infection, and then targeted blood tests and imaging to identify structural risk factors and assess the degree of renal involvement. Dipstick and microscopy serve as rapid orientation tools but are confirmatory only when both leucocyte esterase and nitrites are positive; a negative dipstick in a low-probability setting is reassuring, but a positive result in an infant must always be followed by culture from a reliable specimen.
Urine collection methods (in order of decreasing contamination risk):
1. Suprapubic aspiration (SPA): gold standard in infants; any growth of a uropathogen is significant. The bladder is located by ultrasound guidance and aspirated percutaneously.
2. Catheter specimen (in/out catheterisation): acceptable alternative to SPA; significant bacteriuria ≥10⁴ CFU/mL of a single organism.
3. Clean-catch midstream urine (MSU): feasible in toilet-trained children; significant bacteriuria ≥10⁵ CFU/mL of a single organism.
4. Urine bag (adhesive bag specimen): high contamination rate (∼30–50% false-positive culture); acceptable only for dipstick screening — a positive culture from a bag specimen must ALWAYS be confirmed by catheter or SPA before treating.
Dipstick and microscopy: Leucocyte esterase positive (≥1+) indicates pyuria; nitrites positive suggest gram-negative bacteriuria. Combined leucocyte esterase + nitrites positive has sensitivity ∼92% and specificity ∼72% for culture-confirmed UTI. Microscopy showing >10 WBC/mm³ (unspun) or >5 WBC/hpf (centrifuged) = pyuria; bacteria on unspun urine correlates with significant bacteriuria.
Urine culture remains the diagnostic gold standard. A pure growth of a uropathogen above the threshold for the collection method — combined with compatible clinical features — confirms UTI. Mixed growth of ≥2 organisms usually indicates contamination and warrants recollection.
Blood investigations in suspected pyelonephritis: FBC (leucocytosis, neutrophilia), CRP and procalcitonin (raised in pyelonephritis, helping distinguish from cystitis), blood culture (bacteraemia in 2–10% of febrile UTI infants), urea, electrolytes, and creatinine (for renal function assessment).
Imaging protocol (risk-stratified, age-based):
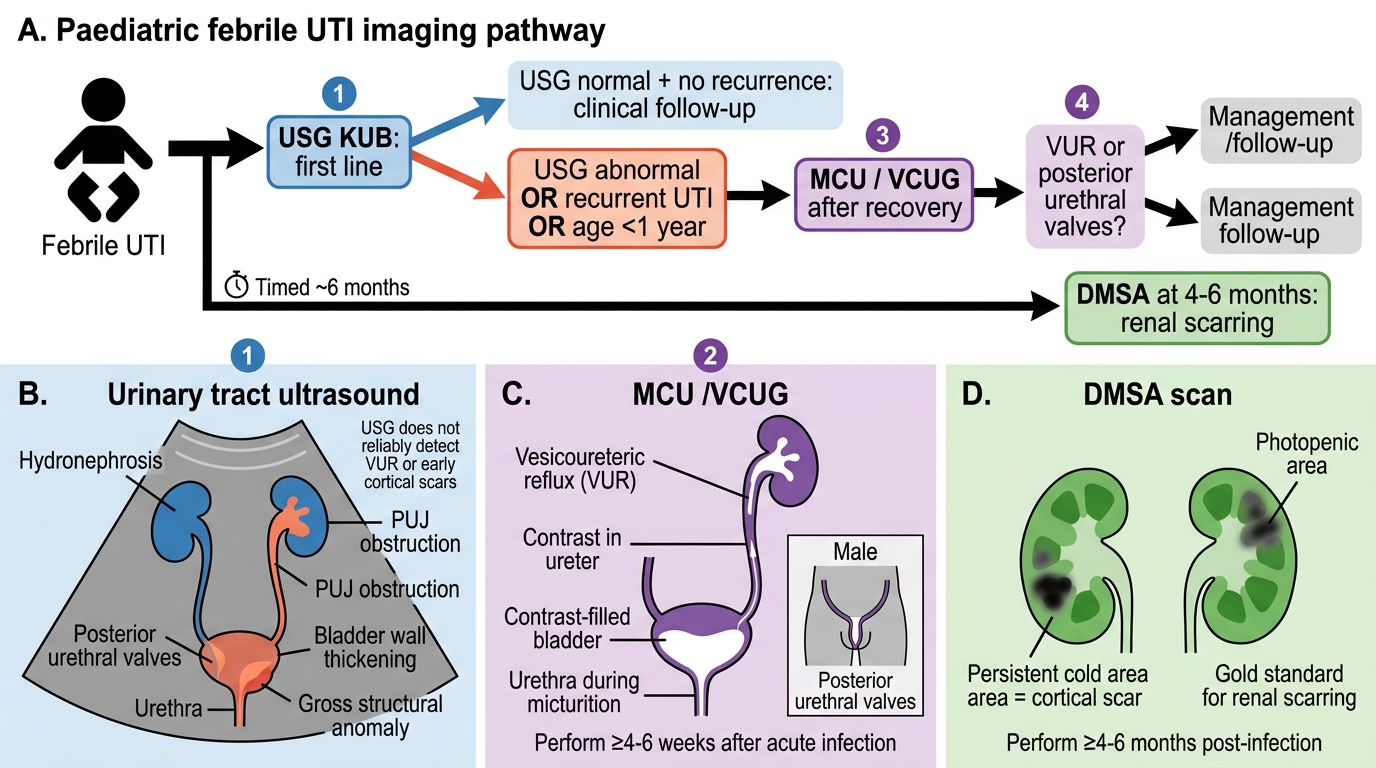
Paediatric Febrile UTI Imaging Algorithm
The imaging goal is to detect structural anomalies predisposing to recurrent infection and to identify renal scarring that will determine long-term follow-up:
• Ultrasound (USG) KUB: first-line in all children after febrile UTI; identifies hydronephrosis, PUJ obstruction, posterior urethral valves, bladder thickening, and gross structural anomalies. It does NOT reliably detect VUR or early cortical scars.
• Micturating cystourethrogram (MCU/VCUG): standard investigation for VUR; indicated when USG is abnormal, when the child is <1 year of age with febrile UTI, or when UTI recurs. Performed ≥4–6 weeks after the acute episode (acute infection increases false-positive grade). In boys, MCU also diagnoses posterior urethral valves.
• DMSA (dimercaptosuccinic acid) scintigraphy: radionuclide scan that detects acute pyelonephritis (photopenic areas) and permanent cortical scars. Performed ≥4–6 months post-infection to allow transient pyelonephritic changes to resolve; persistent cold areas = established scars. DMSA is the gold standard for detecting renal scarring.
• MAG-3 renogram/DTPA: used when differential renal function and drainage kinetics are needed (e.g., PUJ obstruction assessment).
The IAP/Ghai approach for children with first febrile UTI <1 year: USG promptly, MCU after recovery (as the risk of underlying VUR/anomaly is highest in this age group). In children >1 year with first uncomplicated UTI: USG within 6 weeks; MCU only if USG is abnormal or UTI recurs.
CLINICAL PEARL
Never use a bag urine specimen for culture to diagnose UTI in an infant. The contamination rate approaches 50%, and treating a positive bag culture without confirmation leads to over-treatment, antibiotic resistance, and missed alternative diagnoses. Always confirm a positive bag dipstick or bag culture with a catheter specimen or SPA before starting antibiotics in a non-critically-ill infant. The only acceptable role of a bag specimen is initial dipstick screening — if dipstick is negative, UTI is very unlikely; if positive, recollect by catheter.