Page 2 of 30
PE20.1 | Urinary Tract Infection — SDL Guide (Part 2)
Management and Complications
Management of UTI in children is guided by three intersecting variables: the child's age (which determines pharmacokinetic parameters and the risk of systemic spread), the severity of the episode (febrile upper UTI with systemic compromise versus afebrile lower urinary tract infection), and the results of urine culture and sensitivity testing. The overarching treatment goals are eradication of the infecting organism from the urinary tract, relief of acute symptoms, prevention of renal parenchymal damage and scarring, and prevention of recurrent infection. Empirical antibiotic selection must account for local resistance patterns — resistance of community E. coli to co-trimoxazole exceeds 30% in many Indian settings, which makes culture-guided therapy essential rather than optional. Antibiotic choice, route, and duration are therefore age-stratified, and the clinician must be prepared to de-escalate or switch regimens promptly once sensitivity results are available.
Antibiotic therapy:
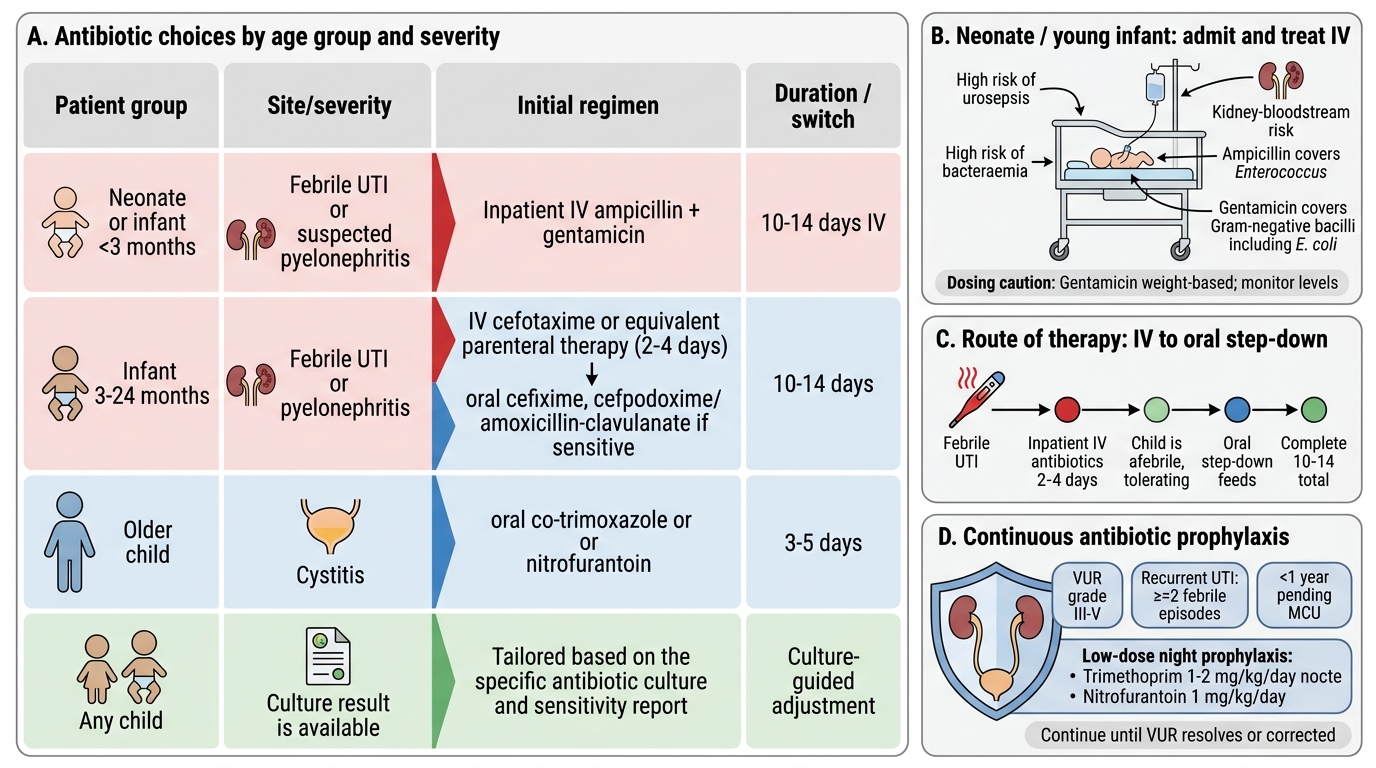
Paediatric UTI Antibiotic Choices by Age and Severity
- Neonates and infants < 3 months: All require inpatient IV antibiotics regardless of clinical appearance, because of high risk of urosepsis and bacteraemia. Standard regimen: ampicillin + gentamicin (covers E. coli and Enterococcus; gentamicin is weight-based: 5–7.5 mg/kg/day OD in neonates; dose adjustments per serum levels). Duration 10–14 days IV.
- Infants 3–24 months with febrile UTI / pyelonephritis: Parenteral therapy for 2–4 days until afebrile and tolerating feeds; transition to oral. Third-generation cephalosporins (cefotaxime IV, cefpodoxime or cefixime oral) or amoxicillin-clavulanate (if sensitivities known). Total duration 10–14 days.
- Older children with cystitis (afebrile): Oral antibiotics for 3–5 days: trimethoprim-sulfamethoxazole (co-trimoxazole) or nitrofurantoin (for lower UTI only — does not achieve tissue levels for pyelonephritis). Local resistance patterns must guide empirical choice.
- Adjust all regimens per culture and sensitivity results.
Antibiotic prophylaxis: Low-dose continuous prophylaxis (trimethoprim 1–2 mg/kg/day at night, or nitrofurantoin 1 mg/kg/day) is recommended for children with VUR grade III–V, following recurrent UTIs (≥2 febrile episodes), and in all children <1 year pending MCU results. Duration: until VUR resolves on surveillance MCU or surgical correction is completed.
Surgical referral: Children with high-grade VUR (IV–V), posterior urethral valves, obstructive uropathy causing hydronephrosis, or renal stones causing obstruction should be referred to a paediatric urologist. Endoscopic submucosal injection (STING procedure) or open/laparoscopic ureteric reimplantation corrects VUR in selected cases.
Complications of untreated or recurrent UTI:
• Renal scarring (reflux nephropathy): the most serious long-term consequence; occurs in 10–15% of children after pyelonephritis, and in a much higher proportion with high-grade VUR and delayed treatment.
• Hypertension: renal scars activate the renin-angiotensin-aldosterone system; affected children need periodic blood pressure monitoring.
• Chronic kidney disease (CKD): bilateral scarring with significant nephron loss may progress to CKD; the leading indication for renal transplantation in young adults in some series is reflux nephropathy.
• Urosepsis / bacteraemia: particularly in neonates and immunocompromised children.
• Pyonephrosis and perinephric abscess: rare but potentially life-threatening complications of obstructed, infected systems.
Self-Assessment
Having worked through the clinical, pathophysiological, diagnostic, and therapeutic dimensions of UTI in children, you are now equipped to approach this common but consequential condition systematically. The self-assessment below tests not merely recall, but the application of integrated reasoning — the kind required in a ward round, an OSCE station, or a clinical examination. Before attempting the questions, take a moment to consolidate the key decision points: which collection method is appropriate for which patient, which imaging investigation answers which clinical question, how antibiotic selection and duration change with the child's age and the anatomical site of infection, and which structural abnormalities demand referral versus watchful waiting with prophylaxis. These are the pivots on which clinical management of paediatric UTI turns, and facility with them will serve you in every paediatric nephrology and general paediatrics encounter you face.
- UTI is the commonest serious bacterial infection in infants; presentation is age-dependent and non-specific in the very young.
- E. coli accounts for ~80% of cases; ascending infection via uroepithelial P-fimbriae adhesion is the dominant mechanism.
- Urine must be collected by the correct method — bag specimen is only valid for dipstick screening, not culture.
- Bacteriological thresholds differ by collection method: SPA any growth; catheter ≥10⁴ CFU/mL; midstream ≥10⁵ CFU/mL.
- Imaging is risk-stratified: USG first line; MCU for VUR detection; DMSA for renal scarring at 4–6 months post-infection.
- Neonates and young infants require IV antibiotics; older children with cystitis may be managed orally.
- Prophylaxis is indicated for VUR grade III–V and recurrent febrile UTI.
- Renal scarring → hypertension and CKD are the long-term stakes that make prompt treatment imperative.
SELF-CHECK
A 6-month-old boy presents with fever and is found to have pyuria on catheter specimen. Ultrasound shows mild left hydroureteronephrosis. What is the most appropriate next imaging investigation to detect vesicoureteric reflux?
A. DMSA scintigraphy
B. MAG-3 renogram
C. Micturating cystourethrogram (MCU)
D. CT urogram
Reveal Answer
Answer: C. Micturating cystourethrogram (MCU)
MCU (micturating cystourethrogram / voiding cystourethrogram) is the standard investigation for detecting and grading vesicoureteric reflux (VUR). It is performed after recovery from the acute infection (≥4–6 weeks) to avoid falsely elevated reflux grades. DMSA detects renal scarring (not VUR) and is done 4–6 months post-infection. MAG-3 assesses drainage kinetics. CT urogram delivers significant radiation and is not first-line for VUR.