Page 13 of 20
PE21.5 | Juvenile Idiopathic Arthritis — SDL Guide
Learning Objectives
- Define juvenile idiopathic arthritis (JIA) using ILAR criteria (onset <16 years, arthritis ≥6 weeks)
- Classify the seven ILAR subtypes of JIA and identify their distinguishing clinical, serological, and genetic features
- Explain the pathophysiological basis of JIA including immune dysregulation, cytokine involvement, and synovial inflammation
- Recognise the major complications of JIA — particularly chronic anterior uveitis and macrophage activation syndrome (MAS)
- Outline a stepwise management approach: NSAIDs, intra-articular corticosteroids, DMARDs (methotrexate), and biologics with appropriate surveillance
INSTRUCTIONS
JIA is the most common chronic inflammatory arthritis in childhood, yet it remains a diagnosis of exclusion that demands a systematic, subtype-aware approach. Misclassifying the subtype leads to inadequate treatment and avoidable complications — the most feared being chronic uveitis that silently destroys vision. As a final-year student you will encounter children with limp, joint swelling, or unexplained fever in paediatric outpatient and emergency settings. Understanding JIA deeply enables you to distinguish it from septic arthritis (an emergency), guide appropriate investigation, initiate treatment, and organise long-term multidisciplinary follow-up.
References
- Ghai Essential Pediatrics, 9th Ed, Ch 17 — Connective Tissue Disorders (textbook)
- Nelson Textbook of Pediatrics, 21st Ed, Ch 180 — Juvenile Idiopathic Arthritis (textbook)
- IAP Guidelines on JIA Management, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old girl is brought to the paediatric OPD by her mother who noticed the child limping every morning for the past three months. The limp is worse upon waking and gradually improves by mid-morning. On examination you find a warm, swollen, non-tender right knee without redness. There is no fever today, but the mother recalls two brief episodes of low-grade fever last month. Ophthalmology screening, arranged by a vigilant intern, reveals bilateral posterior synechiae on slit-lamp examination — the child had no eye complaints whatsoever. What unifying diagnosis explains the joint disease and the silent ocular findings? How would you subtype it, investigate it, and protect this child's vision and joint function over the next decade?
WHY THIS MATTERS
Juvenile idiopathic arthritis affects approximately 1 in 1,000 children worldwide and is the leading cause of childhood-onset disability from arthritis in India. Unlike adult rheumatoid arthritis, JIA is a heterogeneous umbrella of at least seven distinct subtypes, each with different prognosis, complication profiles, and treatment targets. The stakes are high: oligoarticular JIA can destroy vision through an insidious, asymptomatic uveitis that presents long after irreversible band keratopathy has formed; systemic JIA can trigger macrophage activation syndrome (MAS), a potentially fatal cytokine storm. Early recognition and subtype-correct management with modern DMARDs and biologics has transformed outcomes — most children treated on current protocols maintain functional joints and normal schooling. Your ability to recognise JIA, distinguish it from infection, classify it correctly, and initiate or refer for treatment promptly determines whether a child lives a normal childhood or one defined by pain and disability.
RECALL
Before proceeding, activate your prior knowledge:
- Synovial joint anatomy (from Anatomy): synovial membrane, articular cartilage, joint space, joint capsule — these structures are the targets of JIA inflammation.
- Immune tolerance and autoimmunity (from Physiology/Pathology): T-cell activation requires two signals (antigen + co-stimulation); failure of self-tolerance generates autoreactive lymphocytes; cytokines (TNF-α, IL-1, IL-6) mediate tissue damage.
- Rheumatoid factor (RF) and ANA (from Pathology): RF is an IgM antibody against IgG Fc; ANA detects antinuclear antibodies — both are used in JIA subtyping.
- Septic arthritis (from Paediatric Infections): acute, febrile, single hot joint; Staphylococcus aureus most common; emergency joint aspiration required — must be excluded before diagnosing JIA.
- NSAIDs mechanism (from Pharmacology): COX inhibition → reduced prostaglandin synthesis → anti-inflammatory, analgesic, antipyretic effects; weight-based dosing in children (naproxen, ibuprofen).
Clinical Presentation of JIA
Juvenile idiopathic arthritis is defined by the International League of Associations for Rheumatology (ILAR) as arthritis of unknown aetiology that begins before the age of 16 years, lasts for at least 6 weeks, and cannot be attributed to another identifiable cause. This definition is deliberate — it ensures that transient reactive arthritis (post-viral, lasting <6 weeks) and infections are excluded before a chronic inflammatory diagnosis is made.
Provided image
The clinical presentation of JIA depends heavily on the subtype, but several features are shared across subtypes and should raise suspicion in any child. The cardinal symptom is morning stiffness — the child is stiff and unwilling to move upon waking, a phenomenon sometimes called the "gel phenomenon" because the joints have "gelled" during rest and require warm-up activity to loosen. Unlike adult arthritis, children rarely complain of pain directly; instead, caregivers notice a limp, reluctance to use an arm, or a child who stops participating in play. Physical examination reveals joints that are swollen, warm, and tender on stress but often not as red or acutely inflamed as in septic arthritis. Functional limitation — a child who cannot fully extend the knee or who walks with a flexion deformity — is a late sign of progressive disease.
The affected joint distribution is the first clue to subtype: a single knee in a young girl suggests oligoarticular disease; symmetric small-joint involvement of the hands in an older child with elevated RF suggests polyarticular RF-positive disease; high quotidian fever with a salmon-coloured evanescent rash and joint pain in a toddler points to systemic JIA. Each pattern will be elaborated under the ILAR classification.
Key distinguishing features from other joint disorders include:
• Septic arthritis: acute onset, high fever, extreme tenderness, raised WBC/CRP, requires emergency aspiration
• Reactive arthritis: follows a documented infection (streptococcal, enteric), usually self-limiting <6 weeks
• Trauma: history, usually single joint, no systemic features
• Leukaemia: bone pain rather than joint swelling, night pain, anaemia, lymphadenopathy — must be excluded before JIA treatment
ILAR Classification of JIA Subtypes
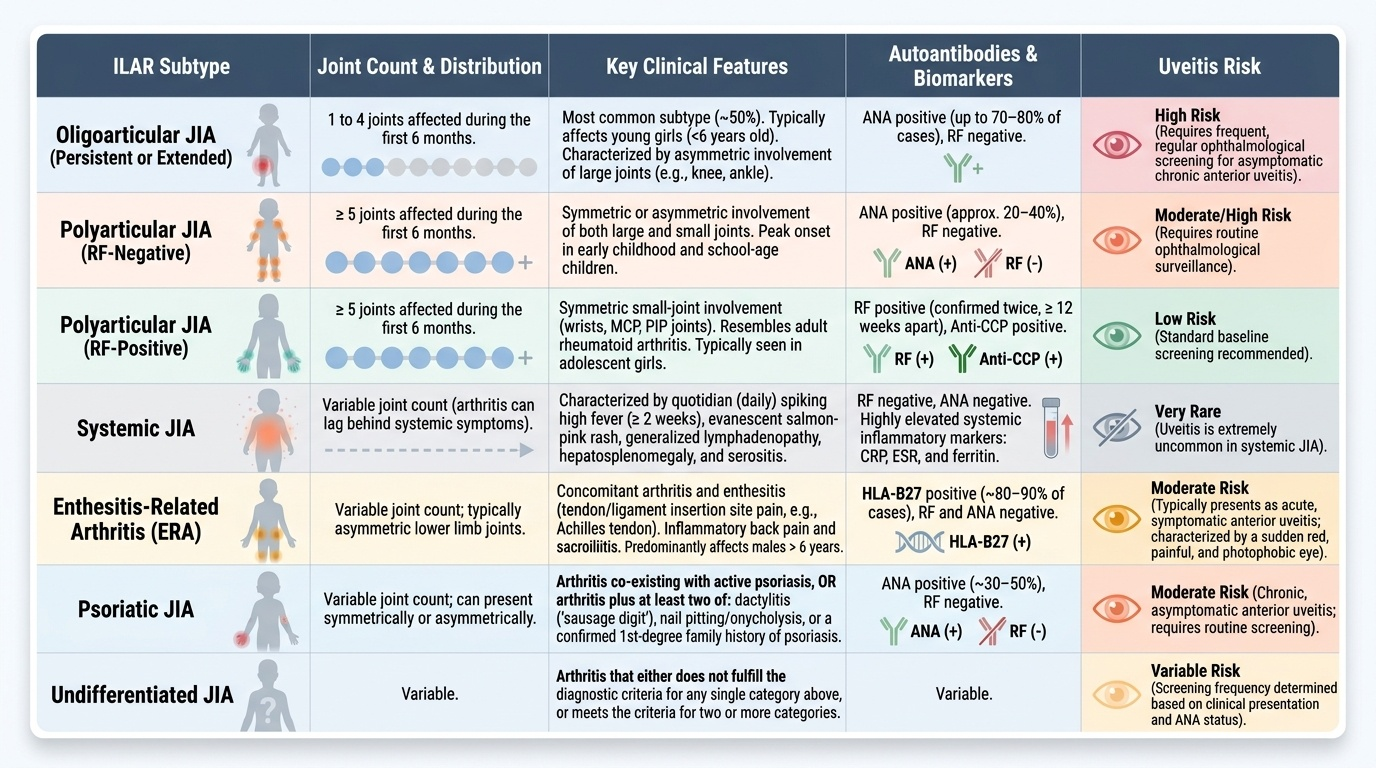
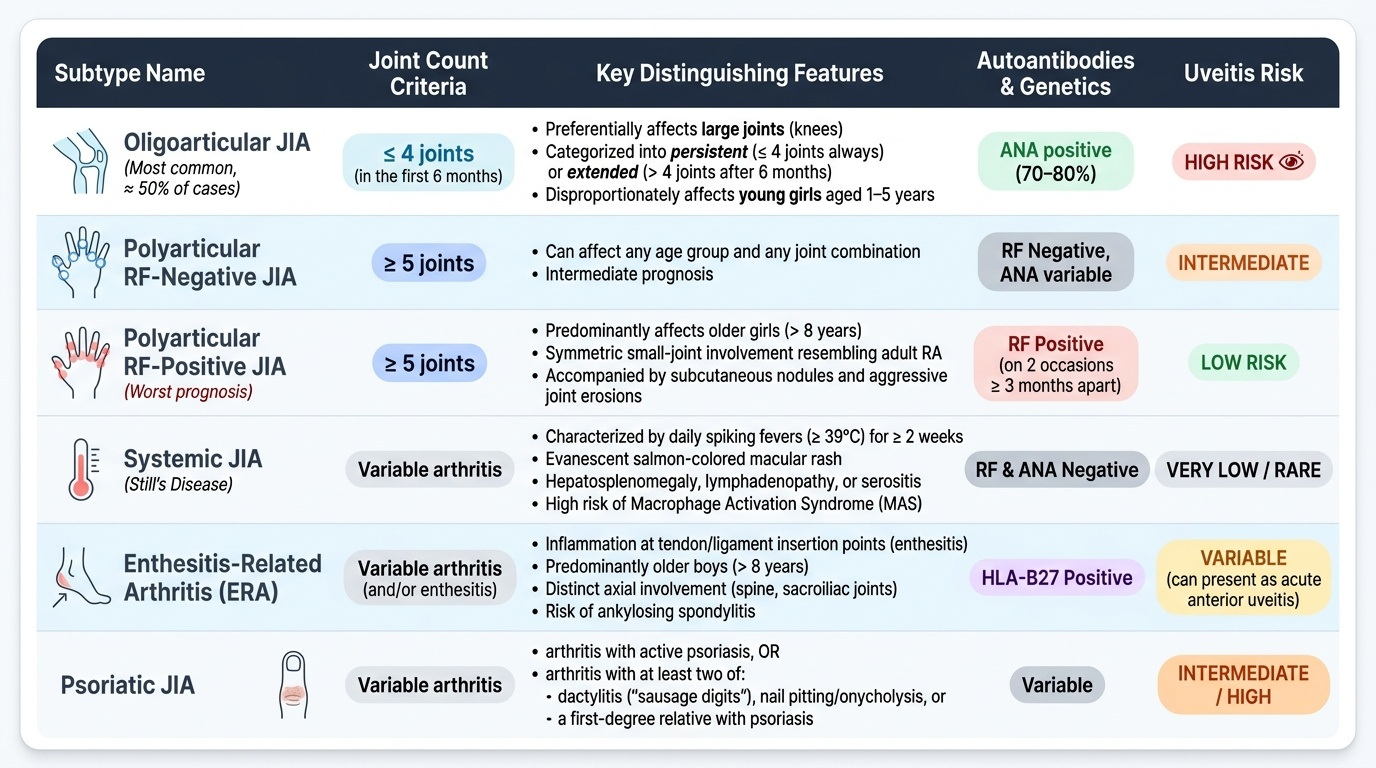
The ILAR classification (revised Durban 2001) recognises seven mutually exclusive subtypes of JIA, each defined by joint count, disease duration, serology, and systemic features in the first six months of illness. Understanding the subtypes is not merely academic — it determines prognosis, complication surveillance, and treatment targets.
Provided image
1. Oligoarticular JIA (most common subtype, ~50% of all JIA in India and globally) affects ≤4 joints in the first 6 months. It preferentially involves large joints — the knee is the single most common affected joint. It is divided into persistent (never exceeds 4 joints) and extended (becomes polyarticular after 6 months). Young girls aged 1–5 years are disproportionately affected. ANA positivity is found in 70–80% and is the most important risk marker for chronic anterior uveitis (see complications).
2. Polyarticular RF-negative JIA affects ≥5 joints and is RF-negative. It can affect any age and any joint combination. It carries intermediate prognosis.
3. Polyarticular RF-positive JIA affects ≥5 joints with a positive rheumatoid factor on two occasions ≥3 months apart. It predominantly affects older girls (>8 years) and resembles adult rheumatoid arthritis in its symmetric small-joint involvement, subcutaneous nodules, and aggressive joint erosions. It has the worst prognosis among JIA subtypes.
4. Systemic JIA (Still's disease) is characterised by arthritis accompanied by fever for ≥2 weeks that is quotidian (daily spikes to ≥39°C, returning to normal between spikes), plus at least one of: evanescent salmon-coloured macular rash (appearing with fever, fading as fever resolves), hepatosplenomegaly, lymphadenopathy, or serositis (pericarditis, pleuritis). RF and ANA are typically negative. The major complication is macrophage activation syndrome (MAS), described under complications.
5. Enthesitis-related arthritis (ERA) is defined by arthritis and/or enthesitis (inflammation at tendon/ligament insertion points) in HLA-B27-positive children, predominantly older boys (>8 years). It may evolve into ankylosing spondylitis. Axial involvement (sacroiliac joints, spine) distinguishes it from other subtypes.
6. Psoriatic JIA is defined as arthritis with psoriasis, or arthritis with at least two of: dactylitis (sausage digit), nail pitting or onycholysis, and a first-degree relative with psoriasis. The joint pattern can be oligoarticular or polyarticular.
7. Undifferentiated JIA encompasses cases that fit none or more than one of the above categories.
The mnemonic "OPPER UP" (Oligoarticular, Polyarticular RF−, Polyarticular RF+, ERA, systemic [bRave], Undifferentiated, Psoriatic) may assist recall during clinical encounters.
SELF-CHECK
A 4-year-old girl presents with a swollen right knee for 3 months with morning stiffness. ANA is positive, RF is negative. Slit-lamp reveals asymptomatic anterior uveitis. Which JIA subtype does she most likely have?
A. Polyarticular RF-positive JIA
B. Oligoarticular JIA
C. Systemic JIA (Still's disease)
D. Enthesitis-related arthritis
Reveal Answer
Answer: B. Oligoarticular JIA
Oligoarticular JIA is the most common subtype (~50%), affecting ≤4 joints in the first 6 months; large joints (especially the knee) in young girls are the classic pattern. ANA positivity (70–80% of oligoarticular cases) is the primary risk marker for chronic anterior uveitis, which is often asymptomatic and discovered only on routine slit-lamp screening — exactly as in this case. Polyarticular RF-positive JIA affects older girls with symmetric small joints. Systemic JIA features quotidian fever and rash. ERA affects HLA-B27-positive older boys with enthesitis.
Pathophysiology and Aetiology of JIA
The aetiology of JIA is multifactorial, involving a complex interplay between genetic susceptibility, environmental triggers, and immune dysregulation. No single cause has been identified, and different subtypes appear to have distinct pathogenetic mechanisms, explaining why biologics targeting different cytokines work for different subtypes.
Genetic susceptibility is supported by the strong association with specific human leucocyte antigen (HLA) alleles. HLA-DRB1 alleles are associated with oligoarticular and polyarticular JIA. HLA-B27 is strongly associated with enthesitis-related arthritis (~80% of ERA patients) and carries risk for axial spondyloarthropathy. The clustering of JIA in families confirms a polygenic contribution, though concordance in identical twins is only ~30%, indicating that genes are necessary but not sufficient.
Environmental triggers include infectious agents (viral or bacterial antigens that may act as molecular mimics triggering autoreactive T cells), psychological stress, and possibly gut microbiome dysbiosis. No single pathogen has been causally proven, but the epidemiological temporal association with upper respiratory infections is noted in systemic JIA onset.
Immune dysregulation is the central mechanism:
- In oligoarticular and polyarticular JIA, CD4+ T helper cells (particularly Th17 cells) are activated in the synovium. They produce pro-inflammatory cytokines — tumour necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and interleukin-17 — that activate synovial fibroblasts and macrophages. The result is synovial membrane hyperplasia (pannus formation), leading to cartilage degradation and eventual bone erosion.
- In systemic JIA, the predominant drivers are IL-1β and IL-6, produced by innate immune cells (macrophages, neutrophils) rather than adaptive T cells. This explains the dramatic response to IL-1 inhibitors (anakinra, canakinumab) and IL-6 inhibitors (tocilizumab) in systemic disease.
- Autoantibodies: ANA is found in ~70% of oligoarticular JIA; its target antigens are unclear but correlate with uveitis risk. RF (IgM anti-IgG Fc) in polyarticular RF-positive JIA mirrors adult RA immunopathology.
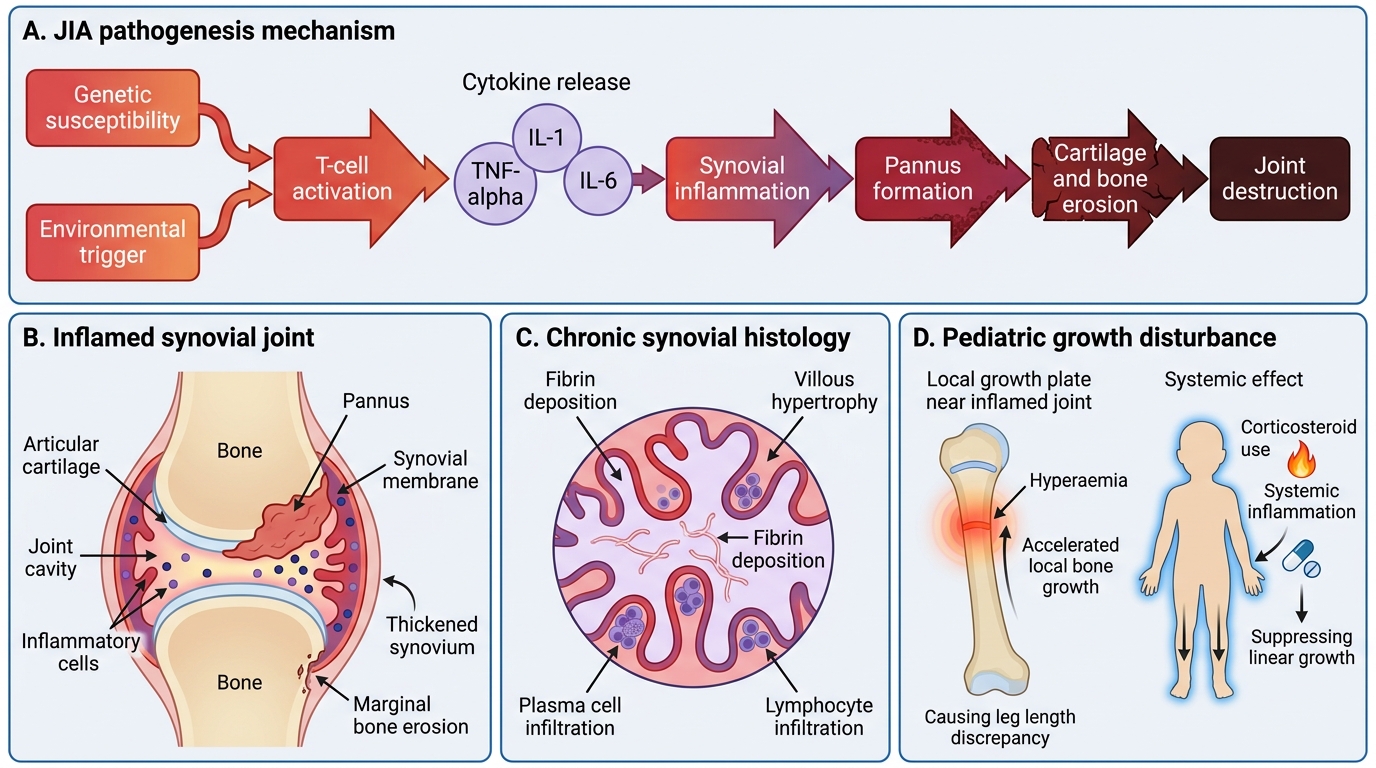
Juvenile Idiopathic Arthritis: Pathogenesis and Consequences
The chronic inflammation within the joint produces the classic synovial histology: villous hypertrophy, plasma cell and lymphocyte infiltration, and fibrin deposition. Growth disturbance is a unique paediatric consequence: chronic hyperaemia from synovitis around a growth plate accelerates local bone growth, causing leg length discrepancy; conversely, systemic inflammation and corticosteroid use suppress linear growth systemically.