Page 8 of 31
PE22.3 | Cardiac Failure — SDL Guide
Learning Objectives
- Describe the aetiology and pathogenesis of cardiac failure in infants and children, including neurohormonal mechanisms
- Recognise the age-specific clinical features of cardiac failure in neonates, infants, and older children
- Apply the Ross Heart Failure Classification for children
- Interpret chest X-ray, ECG, and echocardiographic findings in paediatric cardiac failure
- Outline weight-based pharmacological management including digoxin, furosemide, and ACE inhibitors with correct dosing
INSTRUCTIONS
Cardiac failure in children is not simply an adult heart problem in a smaller body — the causes, clinical features, and priorities of management differ fundamentally by age. A 3-month-old with a large VSD develops failure from volume overload; a teenager with dilated cardiomyopathy develops it from pump dysfunction; a neonate with an arrhythmia may develop it within hours. Recognising this syndrome early — and knowing the weight-based drug doses precisely — is a core competency for any doctor managing children. This module equips you with both the conceptual framework and the practical dosing knowledge you will need at the bedside.
References
- Ghai Essential Pediatrics, 9th edition, Ch 14 — Cardiac Failure in Children (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 452 — Heart Failure (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 3-month-old male infant is brought to the outpatient clinic with a 2-week history of poor feeding — he takes only 40–50 mL per feed, sweats profusely, and falls asleep exhausted midway through a bottle. His weight gain has been only 100 g over the past month (expected 600 g). On examination: respiratory rate 62/min, heart rate 158/min, SpO₂ 93% on room air. There is a grade 3/6 pansystolic murmur at the left sternal border. The liver is palpable 4 cm below the right costal margin. Chest X-ray shows marked cardiomegaly and increased pulmonary vascular markings. What is the syndrome? What is the most likely underlying structural cause? What drug would you start first, and at what dose?
WHY THIS MATTERS
Cardiac failure (heart failure) is a clinical syndrome in which the heart cannot deliver adequate cardiac output to meet the body's metabolic demands, or can do so only at the cost of elevated filling pressures. In children, congenital heart disease — particularly left-to-right shunts — is the most common cause, and cardiac failure from a large VSD or PDA typically manifests at 6–8 weeks of age when pulmonary vascular resistance falls and left-to-right shunting increases dramatically. Cardiac failure is a leading cause of hospitalisation and mortality in children with structural heart disease in India. Understanding the age-specific aetiology, the pathophysiological mechanisms driving compensatory changes, and the precise weight-based dosing of digoxin and furosemide enables you to begin treatment safely before specialist review — a skill that directly affects outcomes in under-resourced settings.
RECALL
Before proceeding, consolidate these prior concepts:
- Cardiac output (PY) = heart rate × stroke volume. Stroke volume depends on preload (filling volume), afterload (vascular resistance), and contractility. In cardiac failure, all three are targeted by treatment.
- Frank-Starling mechanism (PY): up to a point, increased ventricular filling improves stroke volume; beyond that point, the dilated failing heart sits on the flat part of the Starling curve and excess preload worsens congestion without improving output.
- RAAS activation (PY): reduced renal perfusion in cardiac failure activates renin → angiotensin II → aldosterone → sodium and water retention → worsens congestion. ACE inhibitors block this cascade.
- Acyanotic CHD (PE22.1): large VSD and PDA cause left-to-right shunts — increased pulmonary blood flow → increased pulmonary venous return → left heart volume overload → left heart failure. This is the single most common cause of cardiac failure in the 6–12 week age group.
- Normal paediatric vital signs by age (PE): heart rate and respiratory rate are higher in infants than adults — tachycardia in a 3-month-old is ≥160 bpm; tachypnoea is ≥60/min.
Clinical Presentation of Cardiac Failure in Children
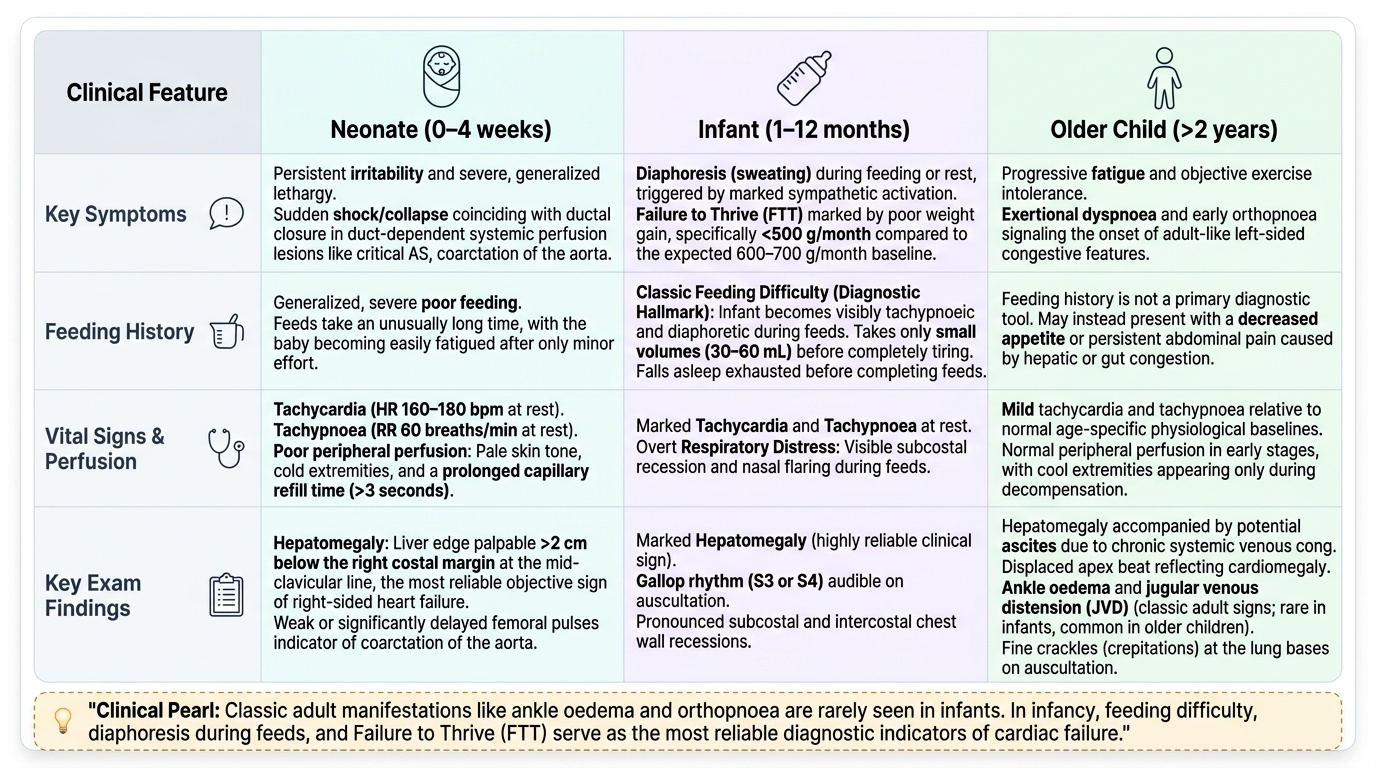
Cardiac failure in children presents differently depending on age, and the 'classic' adult features of ankle oedema and orthopnoea are rarely seen in infants. The clinical manifestations are largely the consequences of pulmonary venous congestion (left heart failure), systemic venous congestion (right heart failure), and reduced cardiac output (poor perfusion). In infants, the most common presentation is feeding difficulty and failure to thrive — both are high-yield clinical features that distinguish cardiac failure from simple respiratory infection. Recognising these age-specific patterns is the first clinical skill this section develops. The clinical history — particularly the feeding history in infants — is often more revealing than the examination, and a systematic age-stratified approach ensures that no key feature is missed when evaluating a child in whom cardiac failure is suspected.
Provided image
Neonatal cardiac failure (0–4 weeks):
• Tachycardia (HR >160–180/min), tachypnoea (RR >60/min) at rest, often with subcostal and intercostal recession
• Pallor and poor peripheral perfusion (cold extremities, prolonged capillary refill >3 sec)
• Hepatomegaly — the most reliable sign of right heart failure in neonates and infants; liver edge >2 cm below the right costal margin at the mid-clavicular line
• Poor feeding, irritability
• In duct-dependent obstructive lesions (critical AS, coarctation of the aorta, hypoplastic left heart), cardiac failure coincides with ductal closure and presents as a shocked neonate
Infantile cardiac failure (1–12 months):
• Feeding difficulties are the hallmark: the infant becomes tachypnoeic and diaphoretic during feeds, takes only small volumes (30–60 mL) before tiring, and falls asleep without completing the feed
• Diaphoresis (sweating) during feeding or at rest — sympathetic activation causes increased sweat-gland activity
• Failure to thrive (FTT): weight gain <500 g/month (expected ~600–700 g/month at 1–3 months); combined effects of increased metabolic demand, decreased caloric intake, and malabsorption from gut congestion
• Respiratory distress during feeds: tachypnoea, subcostal recession, nasal flaring; the infant literally cannot breathe and feed simultaneously
• Hepatomegaly on examination; gallop rhythm (S3/S4) if the examiner is attentive
Older children (>2 years):
• Exercise intolerance — unable to keep up with peers; equivalent to NYHA class II–III in adults
• Orthopnoea (preference for sitting or sleeping elevated) — from pulmonary venous congestion worsening in the recumbent position
• Peripheral oedema — pitting oedema of the dependent areas (ankles/legs in ambulatory children; sacral in bedridden)
• Fatigue, poor appetite
The Ross Heart Failure Classification (validated for children):
| Grade | Symptoms |
|---|---|
| I | Asymptomatic |
| II | Mild tachypnoea/diaphoresis with feeding (infants) or dyspnoea on exertion (older children) |
| III | Marked tachypnoea/diaphoresis, prolonged feeds >40 min, growth failure (infants); significant dyspnoea on minimal exertion |
| IV | Symptoms at rest: tachypnoea, recession, diaphoresis; poor perfusion |
Aetiology and Pathogenesis
Cardiac failure in children results from a diverse range of aetiologies, best understood by grouping them into the physiological mechanism of failure: volume overload, pressure overload, pump failure (myocardial dysfunction), and high-output states. The age at presentation is the single most useful clinical clue to the likely aetiology — different structural and functional causes manifest at predictable developmental timepoints related to the natural history of the lesion, changes in pulmonary vascular resistance, and the timing of ductus closure. Neurohormonal activation is the common downstream pathway regardless of aetiology and directly explains both the clinical signs and the therapeutic targets — making it the essential conceptual bridge between understanding why a child has heart failure and selecting the most appropriate drugs to treat it.
Aetiology by mechanism and age:
Volume overload (left-to-right shunts — most common cause in infants):
• Large VSD: onset of failure at 6–8 weeks (when pulmonary vascular resistance falls physiologically, increasing left-to-right shunt). Pansystolic murmur at left sternal border, cardiomegaly, pulmonary plethora.
• PDA: continuous machinery murmur under left clavicle; predominant left heart volume overload; wide pulse pressure; bounding pulses.
• Large ASD: rarely causes failure in infancy (right heart dilates gradually); onset of symptoms more often in childhood/adulthood.
• AVSD (atrioventricular septal defect, associated with Down syndrome): combined volume overload via atrial and ventricular components.
Pressure overload (outflow obstruction):
• Critical aortic stenosis (AS): neonatal emergency; left heart failure with pulmonary oedema; weak pulses; urgent valvuloplasty.
• Coarctation of the aorta: presents either as neonatal collapse (ductal-dependent systemic flow) or gradual hypertension/failure in older children; discrepant arm/leg pulses and BP.
Myocardial pump failure:
• Dilated cardiomyopathy (DCM): most common cardiomyopathy in children; dilated left ventricle with reduced ejection fraction; idiopathic (majority), post-viral, metabolic, familial.
• Myocarditis: acute inflammatory cardiomyopathy (viral — coxsackievirus B, adenovirus, parvovirus B19); rapid-onset failure, ECG changes (ST changes, arrhythmia), raised cardiac enzymes.
• Hypertrophic cardiomyopathy (HCM): diastolic dysfunction from stiff, hypertrophied LV; risk of sudden cardiac death with exertion.
Arrhythmias:
• Supraventricular tachycardia (SVT): sustained tachyarrhythmia produces tachycardia-induced cardiomyopathy; failure resolves after cardioversion.
• Complete heart block: bradycardia-induced cardiac failure (especially in neonatal lupus — maternal anti-Ro/La antibodies damage the AV node).
High-output failure:
• Severe anaemia (Hb <4–5 g/dL) — compensatory tachycardia and hyperdynamic circulation; treat the anaemia.
• Thyrotoxicosis, large arteriovenous fistula (vein of Galen malformation in neonates).
Pathogenesis — neurohormonal activation:
Reduced cardiac output → baroreceptor-mediated sympathetic activation → tachycardia, vasoconstriction, increased myocardial contractility (short-term compensation) → simultaneously, reduced renal perfusion → RAAS activation → angiotensin II (vasoconstriction + aldosterone release) → sodium and water retention → increased preload and congestion → ventricular dilatation and remodelling → further reduction in contractility (maladaptive long-term effect). BNP (brain natriuretic peptide) is released from distended ventricles and is a useful biomarker of HF severity.
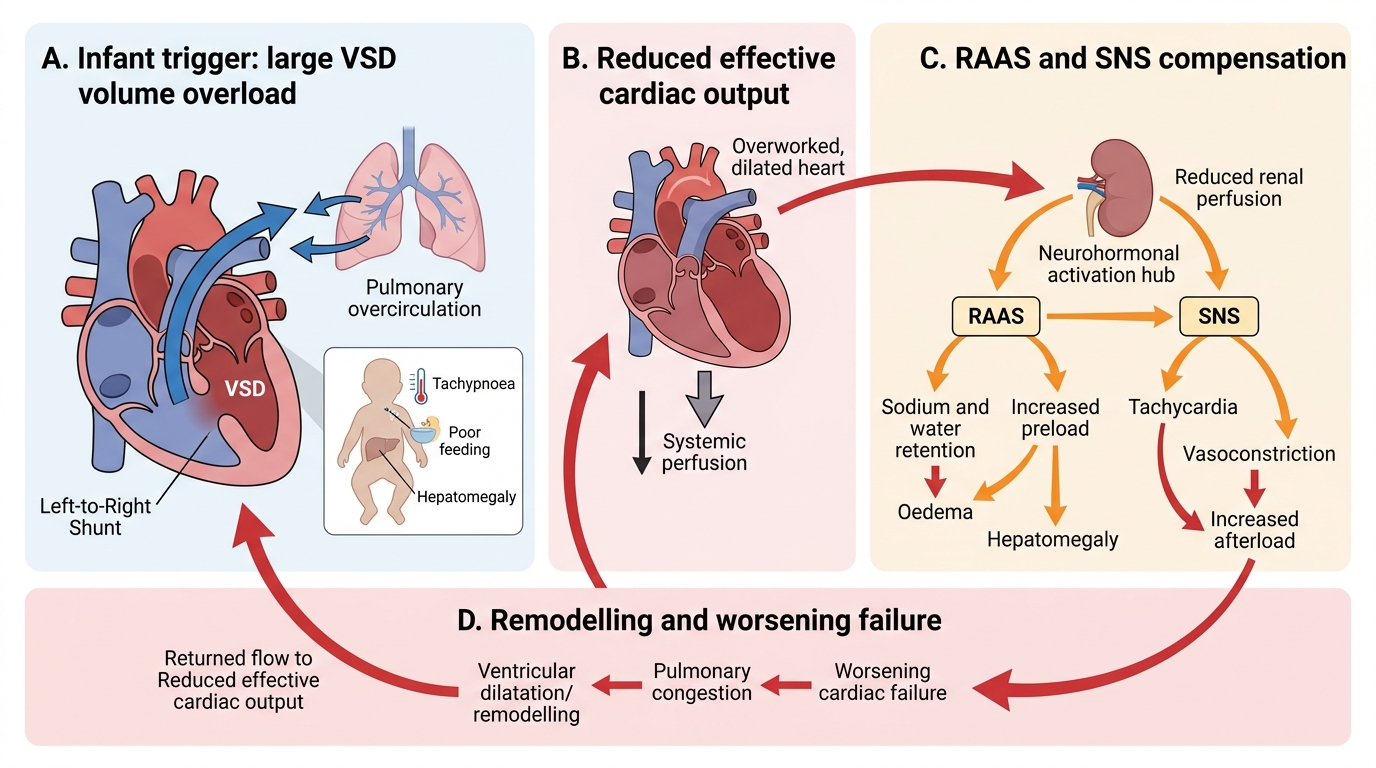
Pathogenesis of Cardiac Failure in Infants
SELF-CHECK
A 2-month-old infant presents with poor weight gain, tachypnoea (RR 64/min), tachycardia (HR 166/min), hepatomegaly (4 cm below costal margin), and a grade 3/6 pansystolic murmur. CXR shows cardiomegaly and increased pulmonary markings. What is the most likely underlying cause of cardiac failure?
A. Dilated cardiomyopathy
B. Large ventricular septal defect causing volume overload
C. Critical aortic stenosis causing pressure overload
D. Supraventricular tachycardia causing pump failure
Reveal Answer
Answer: B. Large ventricular septal defect causing volume overload
A large VSD is the most common cause of cardiac failure in infants at 6–8 weeks of age. As pulmonary vascular resistance falls physiologically after birth, left-to-right shunting through the VSD increases dramatically, causing left heart volume overload, increased pulmonary blood flow (cardiomegaly + plethora on CXR), and the classical features of infantile cardiac failure: poor feeding, diaphoresis, FTT, hepatomegaly, and pansystolic murmur. Critical AS would present with a systolic ejection murmur and poor pulses, not a pansystolic murmur. Cardiomyopathy presents without a structural murmur and at a different age.
Diagnosis and Investigation
The diagnosis of cardiac failure in children is primarily clinical, based on the age-specific features described above, supplemented by investigations that confirm the diagnosis, identify the aetiology, and assess severity. The key investigations are chest X-ray, ECG, and echocardiography, with biochemical tests serving as adjuncts. The priority is to stabilise the child while the workup proceeds — do not delay diuresis pending echocardiography in a decompensated infant with clear clinical features of cardiac failure. Each investigation answers a specific clinical question: CXR assesses cardiac size and pulmonary vascularity; ECG identifies an arrhythmic cause or myocarditis pattern; echocardiography defines anatomy and systolic function; biochemical tests quantify the severity of haemodynamic compromise and identify reversible precipitants such as anaemia or electrolyte disturbance.
1. Chest X-ray (CXR):
• Cardiomegaly: cardiothoracic (CT) ratio >0.55 in infants (>0.50 in older children). The CT ratio is measured as the widest cardiac diameter divided by the widest internal chest diameter on a PA or AP film.
• Increased pulmonary vascular markings (plethora): indicates increased pulmonary blood flow from left-to-right shunting (VSD, PDA, ASD, AVSD) — engorged pulmonary vessels extending to the lung periphery.
• Perihilar haziness / bat-wing pattern: suggests pulmonary oedema from elevated left atrial pressure (left heart failure, critical AS, severe mitral regurgitation).
• Pulmonary venous congestion: upper-lobe vascular diversion (Kerley B lines in interstitium; ground-glass haziness in alveoli).
2. Electrocardiogram (ECG):
• Identifies the underlying cause: SVT (regular, narrow complex, rate >200/min, absent P waves); complete heart block (dissociated P waves and QRS); ventricular hypertrophy patterns (LVH in volume overload, RVH in pulmonary hypertension).
• Myocarditis: diffuse ST changes, low voltages, PR prolongation, new bundle branch block.
3. Echocardiography — gold standard:
• Defines the structural cause (VSD, PDA, AVSD, outflow obstruction)
• Measures ejection fraction (EF) — reduced EF (<55%) in dilated cardiomyopathy/myocarditis
• Assesses diastolic function (relaxation abnormality in HCM)
• Quantifies shunt magnitude (Qp:Qs ratio), valvular regurgitation severity
• Guides urgency of surgical/catheter intervention
4. B-type natriuretic peptide (BNP) / NT-proBNP: elevated in proportion to ventricular wall stress; useful for monitoring treatment response and distinguishing cardiac from respiratory causes of dyspnoea. Age-specific reference ranges apply.
5. Pulse oximetry and arterial blood gas: assess oxygenation and acid-base status. Metabolic acidosis (elevated lactate, low pH, low bicarbonate) indicates reduced tissue perfusion — a marker of severe cardiac failure requiring urgent inotropic support.
6. Haemoglobin and full blood count: identify anaemia as a precipitating or contributing cause.
7. Thyroid function, viral titres, and metabolic screen as directed by clinical context (myocarditis, metabolic cardiomyopathy).
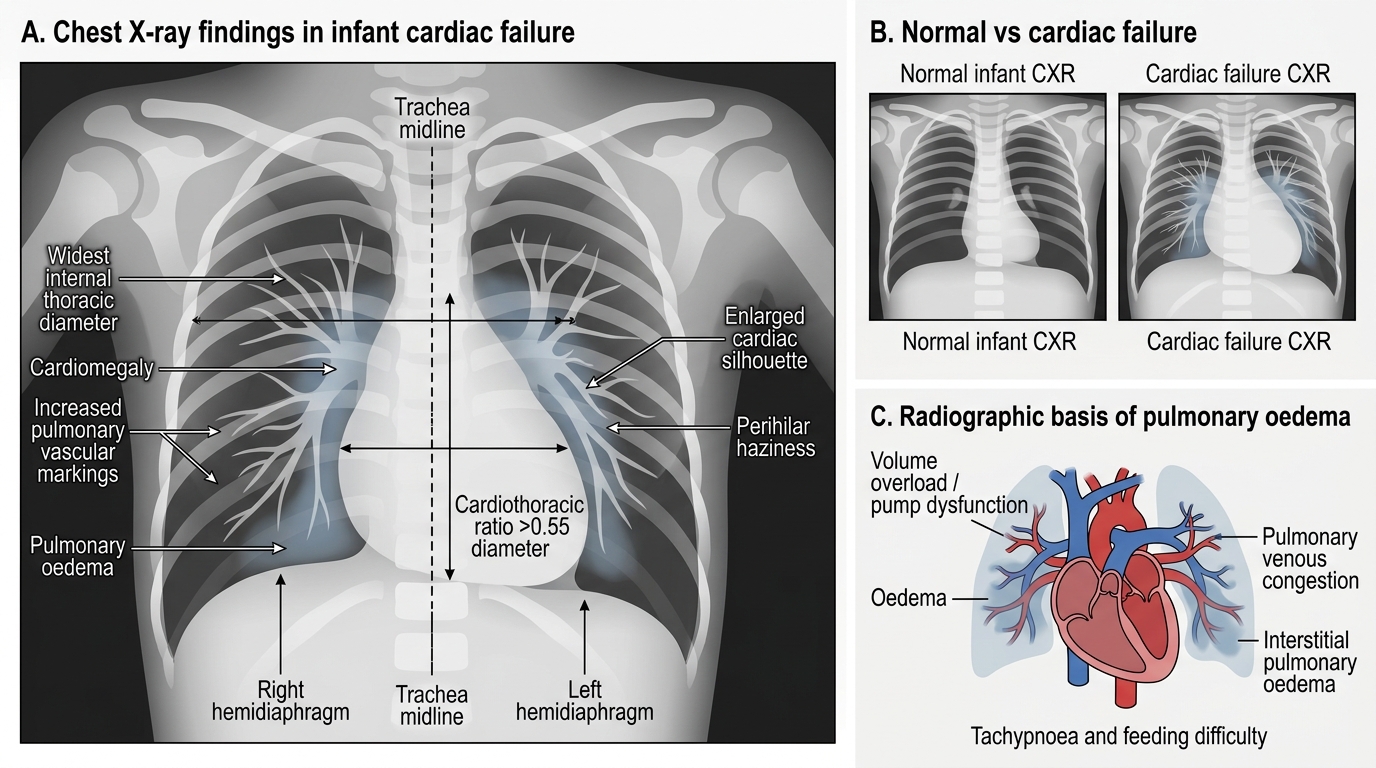
Infant Cardiac Failure on Chest X-Ray
CLINICAL PEARL
Hepatomegaly is the most reliable sign of right heart failure in infants and young children — ankle oedema (the adult hallmark) is rarely present below 2 years of age because infants are non-ambulatory and fluid distributes to the liver and sacrum rather than the ankles. Always measure and document the liver span and edge distance below the costal margin. A liver that decreases in size after diuretic therapy is one of the best clinical markers that treatment is working — even before the child's breathing improves. In contrast, a rapidly enlarging liver in a sick infant signals worsening right heart failure or cardiac tamponade.