Page 9 of 31
PE22.3 | Cardiac Failure — SDL Guide (Part 2)
Management of Cardiac Failure in Children
Management of cardiac failure in children follows the same physiological principles as in adults — reduce preload (diuresis), reduce afterload (vasodilators/ACE inhibitors), and augment contractility (inotropes/digoxin) — but the drug doses are strictly weight-based and the threshold for definitive surgical or catheter correction of the underlying cause is typically lower than in adults. The overarching goal is to stabilise the child haemodynamically, optimise nutrition, and plan timely repair of the underlying structural defect. Medical management is a bridge to surgery in most children with structural heart disease, not a permanent solution. This temporal framing — stabilise now, repair definitively soon — should guide every prescribing and monitoring decision in this group, and it is a key difference from adult heart failure management where medical therapy is often long-term definitive care.
Provided image
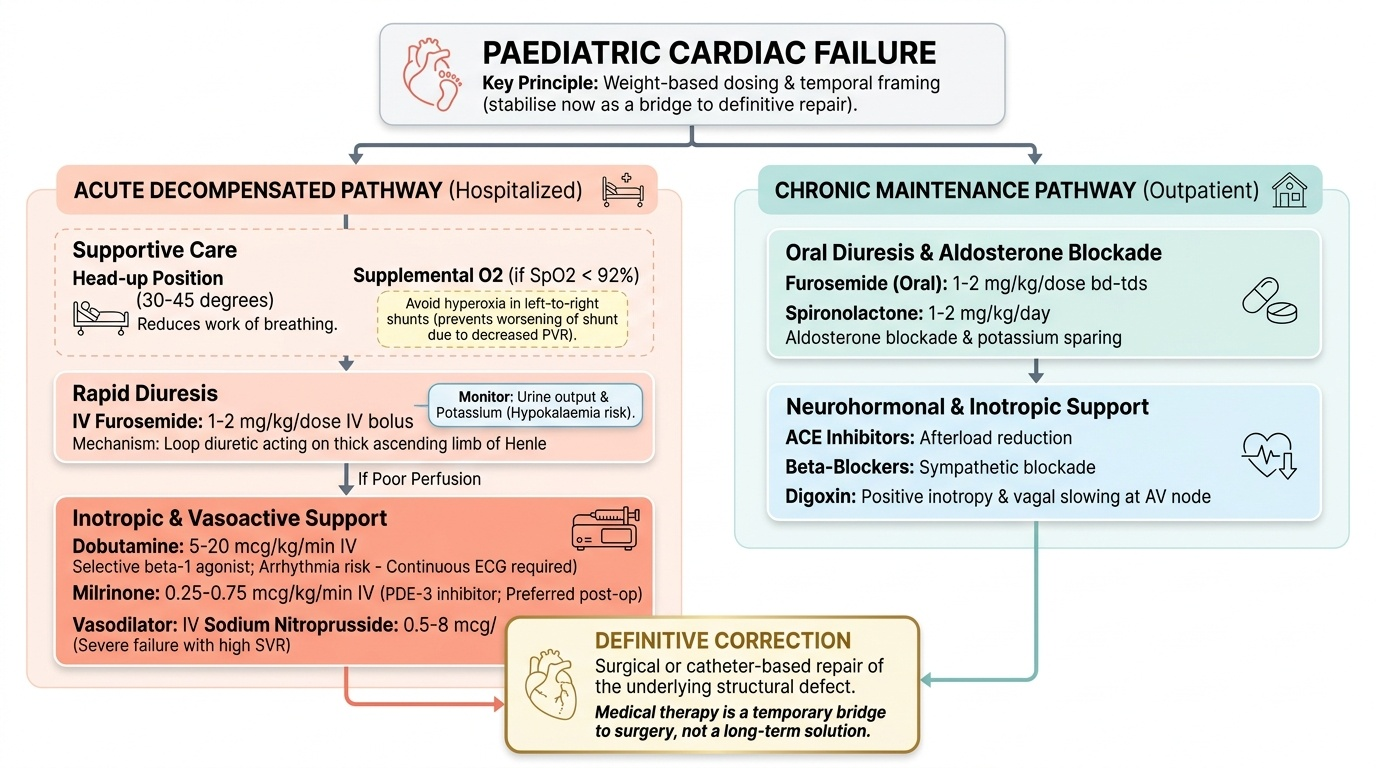
A. Acute decompensated cardiac failure (hospital management):
- Oxygen: supplemental oxygen for hypoxaemia (SpO₂ <92%); however, avoid hyperoxia in left-to-right shunt lesions as excess oxygen reduces pulmonary vascular resistance and worsens shunting.
- Positioning: nurse infant in a 30–45° head-up position to reduce work of breathing.
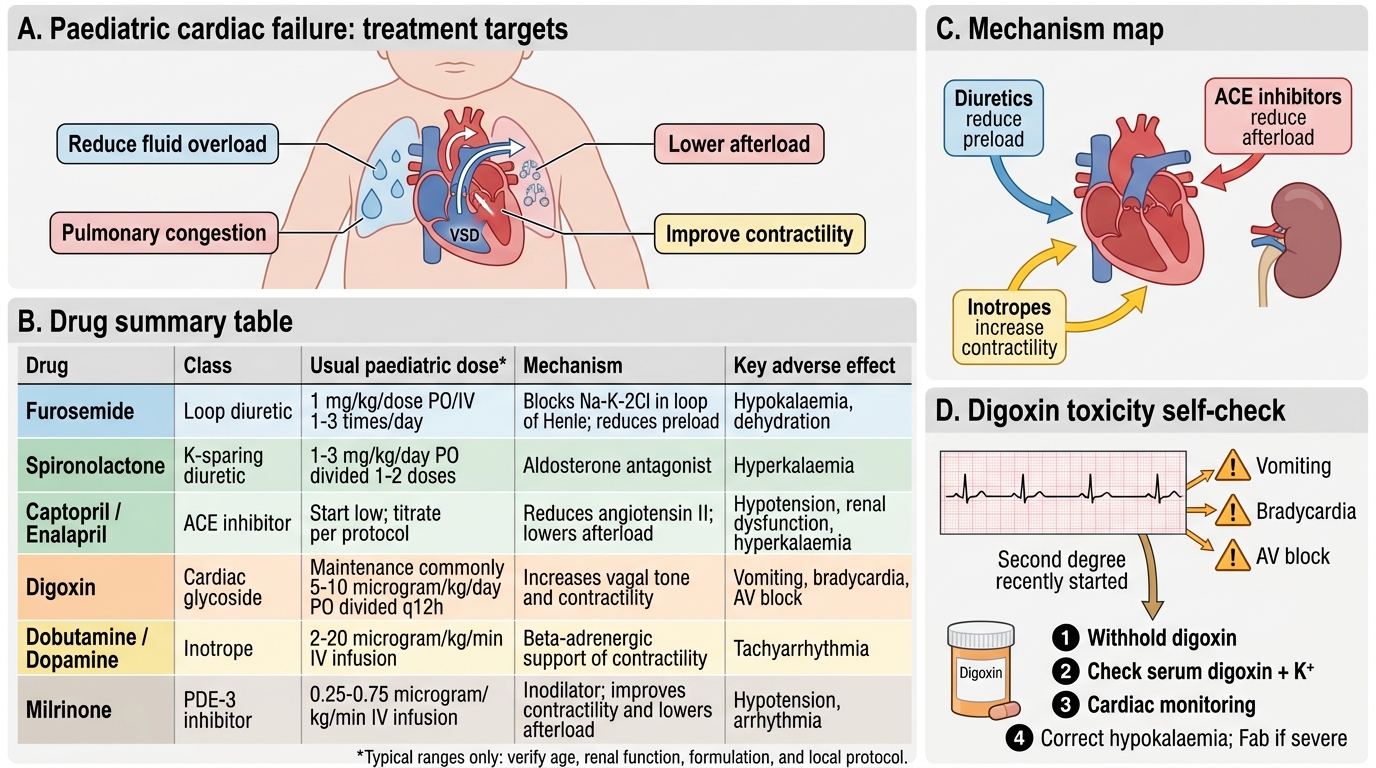
- IV furosemide: 1–2 mg/kg/dose IV bolus (loop diuretic — most potent rapid diuretic; inhibits Na-K-2Cl cotransporter in thick ascending limb of loop of Henle). May repeat every 6–8 h. Monitor urine output, electrolytes (hypokalaemia — supplement potassium).
- Inotropic support in decompensated failure with poor perfusion:
- Dobutamine: 5–20 mcg/kg/min IV (selective beta-1 agonist; increases contractility and heart rate; requires continuous ECG monitoring for arrhythmias)
- Milrinone: 0.25–0.75 mcg/kg/min IV (phosphodiesterase-3 inhibitor; positive inotropy + vasodilation = 'inodilator'; preferred in post-operative cardiac surgery failure)
- Vasodilators: IV sodium nitroprusside (0.5–8 mcg/kg/min) for acute afterload reduction in severe failure with high systemic vascular resistance.
B. Chronic maintenance therapy (outpatient):
- Furosemide oral: 1–2 mg/kg/dose bd–tds. Consider adding spironolactone (1–2 mg/kg/day) for aldosterone blockade and potassium sparing.
- Digoxin: still used in paediatric practice for its positive inotropic effect and vagal slowing at the AV node (useful in AF/flutter). Digitalising doses (oral):
- Premature neonates: 20 mcg/kg total
- Term neonates: 25–30 mcg/kg total
- Infants and children: 30–40 mcg/kg total
- Divide the total digitalising dose: ½ immediately, then ¼ after 8h, then ¼ after further 8h
- Maintenance dose: one-quarter of the digitalising dose, given in two divided doses daily
- Digoxin toxicity: vomiting, bradycardia, AV block, visual changes (yellow-green vision). Therapeutic serum level: 0.8–2.0 ng/mL. Avoid hypokalaemia (potentiates toxicity).
- ACE inhibitors (afterload reduction, RAAS blockade):
- Captopril: 0.1–0.5 mg/kg/dose, 2–3 times daily (short-acting; used in neonates and infants where titrability is important)
- Enalapril: 0.1 mg/kg/day once or twice daily (longer-acting; preferred in older children)
- Monitor renal function and potassium; contraindicated in bilateral renal artery stenosis; avoid in neonates with renovascular disease.
- Beta-blockers (for chronic stable failure, particularly dilated cardiomyopathy): carvedilol 0.05–0.4 mg/kg/dose bd — initiated at low dose, up-titrated over weeks. Not used acutely in decompensated failure.
C. Nutritional support:
High-calorie feeds (100–150 kcal/kg/day; standard formula provides only 67 kcal/100 mL; may need energy supplements or nasogastric feeding if oral intake inadequate). Poor weight gain in cardiac failure is multifactorial and a key quality-of-life indicator.
D. Definitive treatment:
Surgical or catheter correction of the underlying structural defect (VSD patch, PDA ligation, balloon valvuloplasty for AS/PS, coarctation repair) is the definitive management in CHD-related failure and should not be indefinitely delayed by medical management.
SELF-CHECK
You are prescribing oral digoxin for a term neonate (weight 3.5 kg) with cardiac failure from a large VSD. Using the standard digitalising dose of 30 mcg/kg for a term neonate, what is the total digitalising dose, and how is it divided?
A. Total 105 mcg; give all at once
B. Total 105 mcg; give 52.5 mcg immediately, then 26.25 mcg after 8h, then 26.25 mcg after further 8h
C. Total 70 mcg; give 35 mcg bd for 2 days
D. Total 140 mcg; give 70 mcg bd for 1 day
Reveal Answer
Answer: B. Total 105 mcg; give 52.5 mcg immediately, then 26.25 mcg after 8h, then 26.25 mcg after further 8h
Total digitalising dose = 30 mcg/kg × 3.5 kg = 105 mcg. The standard division is: ½ (52.5 mcg) immediately, then ¼ (26.25 mcg) after 8 hours, then ¼ (26.25 mcg) after a further 8 hours — total over 16–24h. The maintenance dose thereafter is ¼ of the total digitalising dose (26.25 mcg) given in two divided doses daily. Never give the entire digitalising dose at once — this risks acute digoxin toxicity including bradycardia and AV block.
Self-Assessment
This section consolidates the clinical and pharmacological knowledge from the module. Cardiac failure in children requires both pattern recognition — identifying the age-specific syndrome — and precise pharmacological knowledge, particularly the weight-based digoxin dosing scheme, which is a common source of potentially dangerous error. Work through the questions below systematically; the numerical thresholds are the most frequently examined and the most consequential in practice. A calculation error in the digoxin dose — using an adult fixed dose rather than the correct mcg/kg weight-based scheme — is one of the most common and serious prescribing errors in paediatrics. Practising these calculations until they are automatic is more than exam preparation: it is a direct patient-safety skill you will use in your very first on-call paediatric shift.
Key self-test questions:
- Name three clinical features that distinguish cardiac failure in a 2-month-old infant from a simple upper respiratory infection.
- What is the Ross Grade III cardiac failure in children, and what are its clinical features?
- Calculate the total digitalising dose of oral digoxin for a 5 kg infant (use 35 mcg/kg). How is the dose divided?
- What is the first-line diuretic for acute cardiac failure in children and its IV dose?
- Name three aetiologies of cardiac failure presenting at 6–8 weeks of age.
- Why is hepatomegaly more reliable than ankle oedema as a sign of heart failure in infants?
- What investigations would you request to confirm the diagnosis and identify the aetiology in a failing infant?
- Name a contraindication to ACE inhibitor use in a neonate with cardiac failure.
Key thresholds and doses:
• Furosemide (IV): 1–2 mg/kg/dose
• Digoxin digitalising dose (term neonate): 25–30 mcg/kg total, divided ½ → ¼ → ¼ over 16–24 h
• Digoxin maintenance: ¼ of digitalising dose in 2 divided doses daily
• Captopril: 0.1–0.5 mg/kg/dose 2–3 times daily
• Cardiomegaly on CXR: cardiothoracic ratio >0.55 in infants
Drugs Used in Paediatric Cardiac Failure
SELF-CHECK
A 5-month-old infant with known large VSD and cardiac failure on furosemide and captopril develops vomiting, bradycardia (HR 80 bpm), and second-degree AV block on ECG. His digoxin was recently started. What is the most likely cause and the immediate management?
A. Hypokalaemia from furosemide; give IV potassium
B. Digoxin toxicity; withhold digoxin, check serum level and potassium, give supportive care
C. Viral myocarditis; start IV immunoglobulin
D. Worsening VSD haemodynamics; arrange urgent surgery
Reveal Answer
Answer: B. Digoxin toxicity; withhold digoxin, check serum level and potassium, give supportive care
The triad of vomiting, bradycardia, and AV block in an infant recently started on digoxin is classic digoxin toxicity. Immediate management: withhold digoxin, check serum digoxin level (toxic >2 ng/mL), check electrolytes (hypokalaemia potentiates toxicity — correct if <3.5 mEq/L), provide cardiac monitoring. In severe toxicity (haemodynamically compromised), digoxin-specific antibody fragments (Fab) may be required. Hypokalaemia from furosemide is a precipitant of digoxin toxicity and must be corrected but is not itself the primary cause of AV block in this context.