Page 20 of 31
PE22.{7-8,11} | Cardiovascular Examination Workflow — SDL Guide
Learning Objectives
- Describe the clinical indications for cardiovascular examination in children and approach the examination with empathy
- Identify the surface anatomy landmarks relevant to paediatric cardiovascular examination
- Demonstrate correct technique for measuring pulse, blood pressure, temperature, and respiratory rate in children and interpret results against age-appropriate reference ranges
- Perform a systematic cardiovascular examination including inspection of the precordium, palpation, percussion, auscultation, and peripheral pulse assessment including femoral pulses
- Interpret findings — precordial bulge, JVP significance, apex displacement, thrills, heaves, murmur grading, abnormal heart sounds — and document findings accurately
INSTRUCTIONS
Cardiovascular examination is one of the most complex and high-yield skills in paediatric clinical medicine. A skilled examiner can detect a ventricular septal defect, coarctation of the aorta, rheumatic valvular disease, or pulmonary hypertension from the bedside — before any investigation. The paediatric cardiovascular examination differs importantly from the adult approach: heart sounds are louder and higher-pitched, the chest wall is thinner, innocent murmurs are extremely common, and vital-sign interpretation requires age-specific reference ranges. Equally important is the human dimension: examining a frightened 4-year-old or explaining a cardiac diagnosis to anxious parents requires deliberate empathic skill. This module trains both.
References
- Ghai Essential Pediatrics, 9th ed., Ch 14 (Cardiovascular System) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 452–453 (Evaluation of the Cardiovascular System) (textbook)
- Forfar and Arneil's Textbook of Pediatrics, 7th ed. (textbook)
- IAP Standard Treatment Guidelines — Paediatric Cardiology (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are posted in a busy paediatric outpatient department. A mother brings her 5-year-old daughter for a routine visit — she is growing well and has no complaints. As part of your examination, you listen to the heart and hear a soft, mid-systolic, musical murmur at the left sternal border. You are not sure if this is innocent or pathological. You need to complete a full cardiovascular examination — but the child is restless and the mother is anxious. How will you examine this child systematically and communicating findings reassuringly, and what will the examination tell you about the significance of the murmur?
WHY THIS MATTERS
The cardiovascular examination is often underutilised in paediatric practice. Studies suggest that congenital heart disease affects approximately 8–10 per 1,000 live births in India, and many cases are detected late because clinicians do not routinely auscultate or palpate during general consultations. An undetected ventricular septal defect, patent ductus arteriosus, or pulmonary stenosis found on an opportunistic examination can lead to timely referral and definitive treatment. Rheumatic heart disease — a sequela of untreated streptococcal pharyngitis — remains a significant burden in India, causing valvular disease in school-age children that is entirely preventable. The ability to detect a new cardiac murmur, assess vital signs accurately for age, and recognise early cardiac failure are foundational skills for every paediatrician.
RECALL
Before proceeding, recall the following prior knowledge: (1) Cardiac anatomy — the heart lies in the mediastinum, with the right ventricle forming most of the anterior surface, the left ventricle forming the left border and apex. The four valve areas on the chest surface: aortic (right 2nd intercostal space), pulmonary (left 2nd intercostal space), tricuspid (left 4th–5th intercostal space, lower sternal border), mitral/apex (5th intercostal space, midclavicular line in adults — slightly more medial in children). (2) Heart sounds — S1 is produced by mitral and tricuspid valve closure at the start of systole; S2 by aortic and pulmonary valve closure at the end of systole. Physiological splitting of S2 widens with inspiration (pulmonary component delayed by increased right ventricular filling). (3) The cardiac cycle — systole (ventricular contraction, S1 to S2) and diastole (ventricular filling, S2 to S1). Murmurs in systole occur between S1 and S2; diastolic murmurs between S2 and S1. (4) Coarctation of the aorta — narrowing typically just distal to the left subclavian artery, causing upper-limb hypertension and lower-limb hypotension, with weak or absent femoral pulses.
Clinical Indications and Relevance of CVS Examination in Children
The cardiovascular examination in children is indicated in a wide range of clinical contexts, far beyond the obviously cardiac presentation. Every new paediatric patient encounter ideally includes at minimum a pulse rate, respiratory rate, and cardiac auscultation — because congenital heart disease and arrhythmias are prevalent and often asymptomatic. A systematic cardiovascular assessment is specifically indicated when a child presents with: (1) a heart murmur detected by any clinician; (2) symptoms of cardiac disease — breathlessness, cyanosis, poor feeding in infants, palpitations, syncope, or exercise intolerance; (3) failure to thrive or poor weight gain, which may be an early sign of cardiac failure in infants; (4) hypertension detected on BP screening; (5) fever with a new murmur (suspicion of infective endocarditis); (6) Down syndrome, Turner syndrome, Marfan syndrome, or other syndromes with known cardiac associations.
Approaching the child with empathy is inseparable from clinical examination. A child who is frightened or distressed cannot be properly examined — they cry, breath-hold, and tense their muscles, making auscultation impossible and vital-sign measurement unreliable. Skilled paediatric examination requires deliberate effort to build rapport before laying a finger on the child. Practical empathic approaches include:
• Introducing yourself to the child (not only the parent), making eye contact at the child's level
• Explaining what you are going to do in simple, age-appropriate language ('I'm going to listen to your heart with this big earphone')
• Allowing the child to hold or examine the stethoscope first
• Examining a stuffed toy or the parent first if the child is anxious
• Using a warm stethoscope and gentle hands throughout
• Allowing the child to sit in the parent's lap for younger children
Documentation should follow the systematic IPPA sequence (Inspection, Palpation, Percussion, Auscultation) and should explicitly record all vital signs with reference to age-specific normal ranges, not just absolute values.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
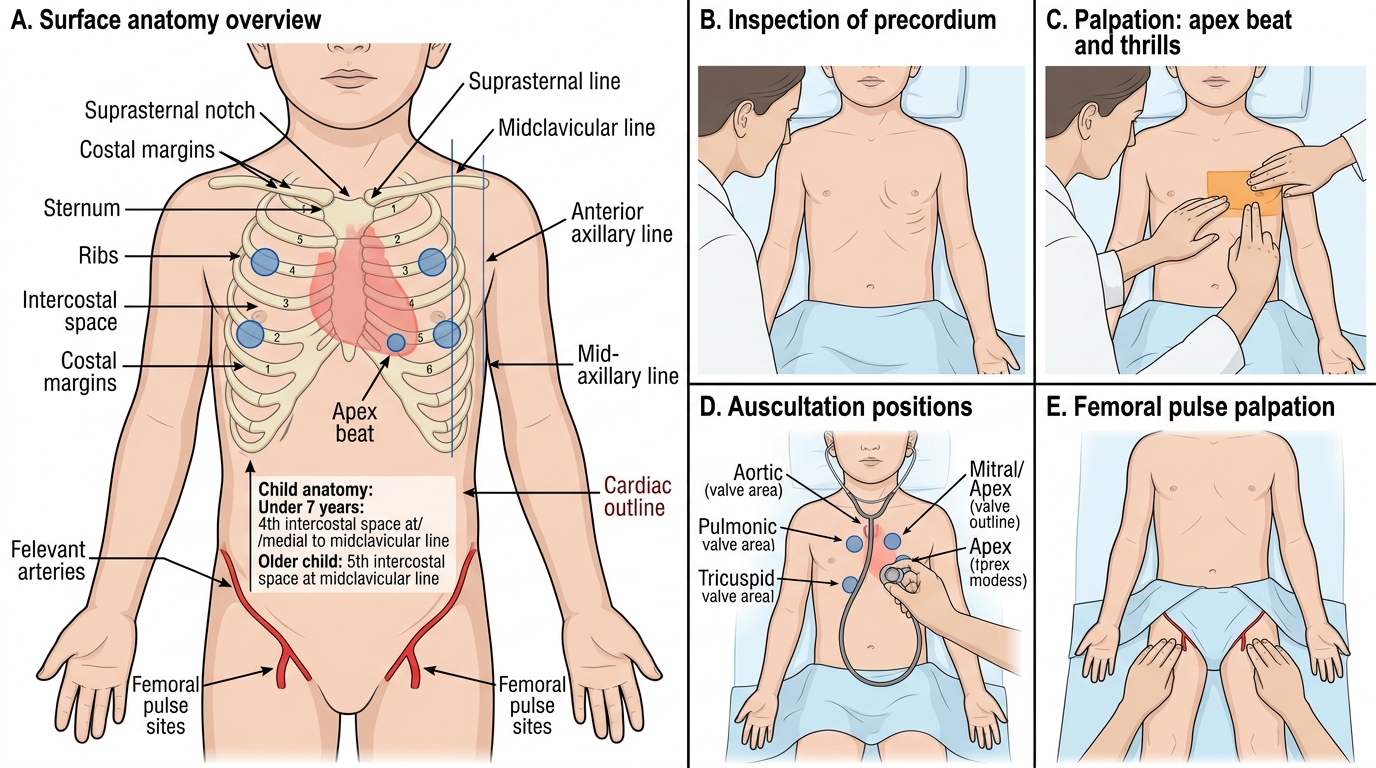
Paediatric Cardiovascular Examination Sequence
Anatomy and Governing Principles
A thorough understanding of cardiac surface anatomy is the foundation of a systematic cardiovascular examination. In children, several anatomical features differ from adults and directly affect examination findings and their interpretation.
Cardiac position and surface anatomy: The heart is positioned in the mediastinum, slightly left of centre. In children, the heart is proportionally larger relative to chest size and positioned more horizontally than in adults, which means the apex beat is typically felt in the 4th intercostal space at or medial to the midclavicular line in children under 7 years, and in the 5th intercostal space at the midclavicular line in older children and adults. The thinner chest wall in children means that cardiac impulses are more readily palpable and heart sounds are louder and higher-pitched. The right ventricle forms most of the anterior surface of the heart and the left sternal border; an enlarged right ventricle produces a left parasternal heave (a sustained lifting impulse along the left sternal border). The left ventricle forms the left border and apex; left ventricular dilatation or hypertrophy displaces the apex beat laterally and downward.
Auscultatory areas in children follow the same topographical convention as in adults, but because the chest is smaller, the areas overlap considerably:
- Aortic area: right 2nd intercostal space (RCSB) — best for aortic stenosis, aortic regurgitation
- Pulmonary area: left 2nd intercostal space (LCSB) — best for pulmonary stenosis, ASD, flow murmurs
- Tricuspid area: left lower sternal border (4th–5th ICS) — best for VSD, tricuspid disease
- Mitral/apical area: cardiac apex (5th ICS, MCL in older children) — best for mitral valve disease, innocent murmurs
In clinical practice, auscultation is not confined to these four spots — the stethoscope should be moved across the precordium and into the axilla, back, and neck (for radiation of murmurs). The back should always be examined: a patent ductus arteriosus murmur radiates to the back; coarctation may cause a systolic murmur in the interscapular region.
Physiological basis of examination findings:
- S1 (mitral and tricuspid closure): best heard at the apex and lower sternal border; louder when the PR interval is short, softer in first-degree AV block
- S2 (aortic [A2] and pulmonary [P2] closure): A2 > P2 normally; physiological splitting on inspiration widens the gap (P2 delayed by increased RV filling); fixed splitting suggests ASD; reversed (paradoxical) splitting is pathological
- S3 (rapid ventricular filling): common as a physiological finding in children under 12 years — heard at apex in early diastole; pathological S3 in older children/adults = ventricular dysfunction or volume overload
- S4 (atrial kick into non-compliant ventricle): always pathological in children — suggests ventricular hypertrophy
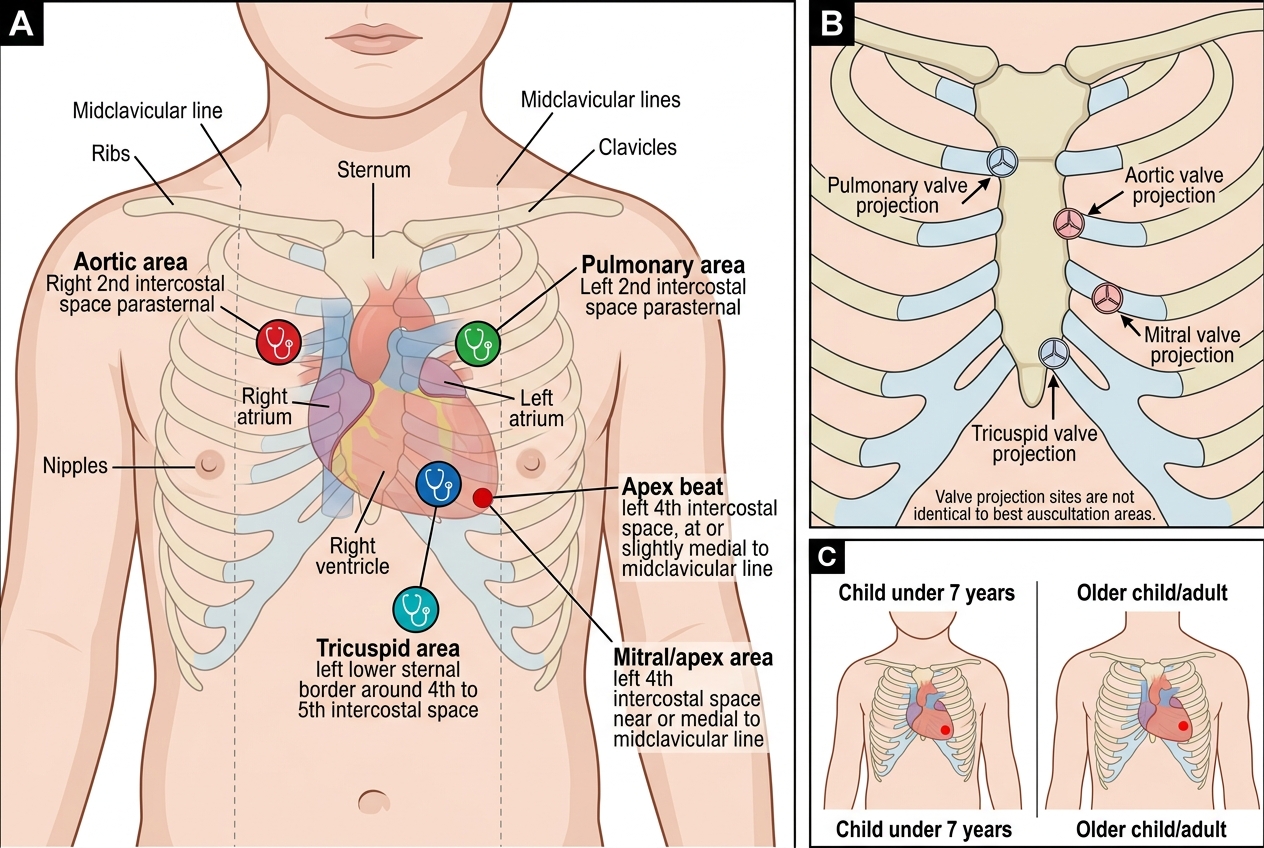
Cardiac Surface Anatomy and Auscultation Areas in a Child
SELF-CHECK
In a child aged 5 years, where would you normally expect to palpate the apex beat?
A. 5th intercostal space at the midclavicular line
B. 4th intercostal space at or medial to the midclavicular line
C. 3rd intercostal space in the left midaxillary line
D. 5th intercostal space in the anterior axillary line
Reveal Answer
Answer: B. 4th intercostal space at or medial to the midclavicular line
In children under 7 years of age, the heart is positioned more horizontally and is relatively larger, so the apex beat is typically felt in the 4th intercostal space at or slightly medial to the midclavicular line. In older children (≥7 years) and adults, the apex moves to the 5th intercostal space at the midclavicular line. A displaced apex (lateral/downward) in any age group suggests left ventricular dilatation or hypertrophy.
Vital Signs Measurement and Age-Based Reference Ranges
Accurate vital sign measurement and correct interpretation against age-specific reference ranges is one of the most important — and most commonly erred — clinical skills in paediatric medicine. A single set of normal adult values does not apply to children: what is tachycardia in an adult may be normal in a toddler, and bradycardia in an infant is a medical emergency requiring immediate action. Unlike adults, in whom vital signs are relatively stable across the adult lifespan, each paediatric age group has its own physiological norm — the heart beats faster, the lungs ventilate at a higher rate, and the blood pressure runs lower in smaller children, reflecting the higher metabolic rate and different cardiovascular physiology of the growing body. An examiner who applies a heart rate of 150 beats per minute to an adult framework will diagnose tachycardia; that same rate is entirely normal in a neonate. For this reason, any paediatric vital-sign assessment must be explicitly referenced against the appropriate age-specific normative range, not intuition or adult norms. The ability to measure vital signs correctly and interpret them against paediatric norms is assessed in both clinical and written examinations.
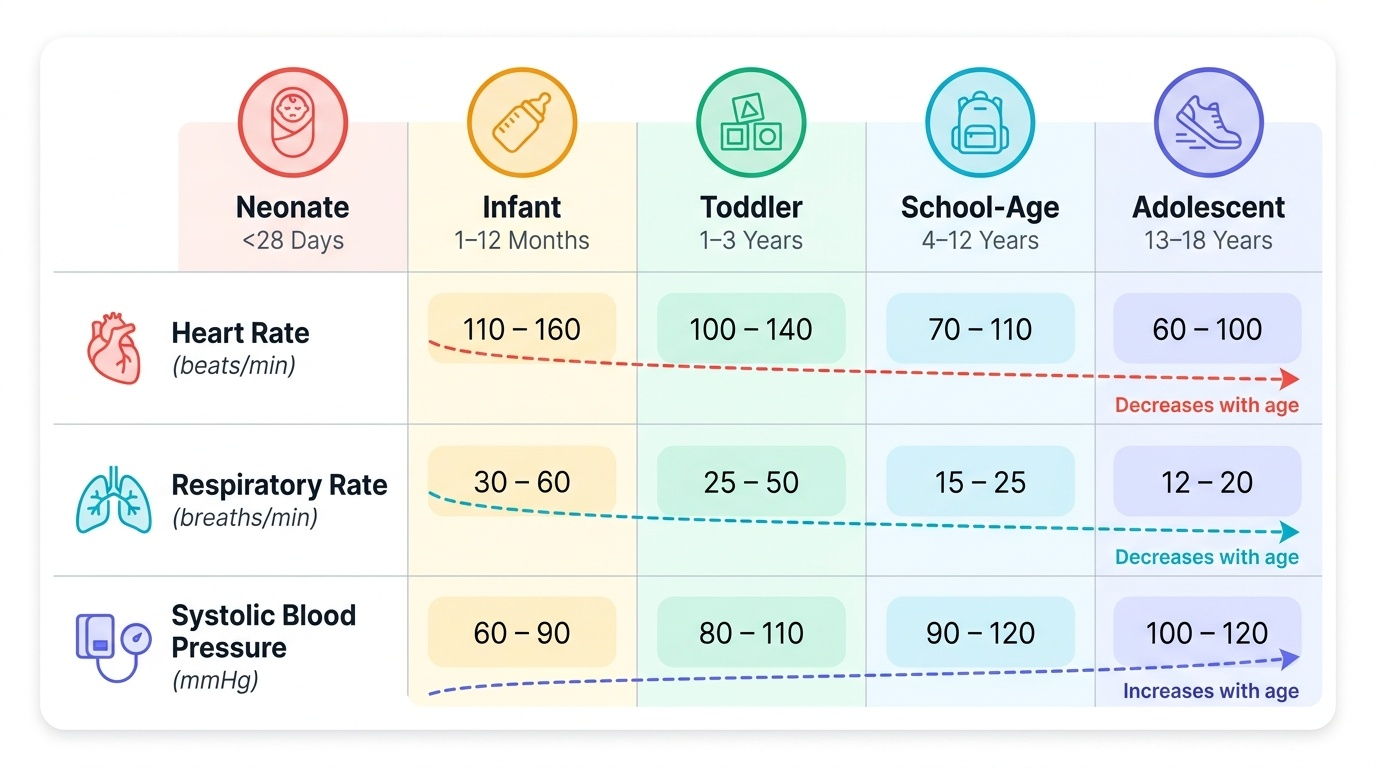
Provided image
Pulse (heart rate):
- Technique: In infants, palpate the brachial artery (antecubital fossa) — it is more reliably palpable than the radial artery. In children over 2 years, use the radial artery. Count for a full 60 seconds (arrhythmias and irregular rhythms require a full minute). Simultaneously assess pulse rhythm, volume (full, normal, thready), and character (bounding in PDA, collapsing in aortic regurgitation).
- Femoral pulse: MUST be palpated in every child — compare with radial pulse simultaneously. A weak or absent femoral pulse, or a radio-femoral delay (femoral felt later than radial), is a cardinal sign of coarctation of the aorta.
- Normal ranges: Neonates 100–160/min; Infants 0–12 months 90–160/min; Toddlers 1–3 years 80–130/min; Preschool 3–5 years 75–115/min; School-age 6–12 years 70–110/min; Adolescents 12–18 years 60–100/min
Blood pressure:
- Technique: Use the correct cuff (bladder width ≥40%, length 80–100% of arm circumference). Measure after 5 minutes of rest, arm at heart level. Use auscultatory method (Korotkoff phase I and V); in young children where sounds persist to zero, use phase IV (muffling) for diastolic.
- Interpretation: Compare against normative percentile tables for age, sex, and height (not fixed cut-offs). Normal = <90th percentile. Right arm is standard; measure all four limbs if coarctation is suspected.
Respiratory rate:
- Technique: Count chest/abdominal movements for a full 60 seconds (respiratory rate is the vital sign most commonly measured inaccurately — timing errors introduce large errors). Count when the child is quiet and unaware — talking, crying, or feeding alters the rate significantly.
- Normal ranges: Neonates 40–60/min; Infants 30–60/min; Toddlers 25–35/min; School-age 20–25/min; Adolescents 12–20/min
- Tachypnoea at rest is a key early sign of cardiac failure in infants — often precedes other signs.
Temperature:
- Method: Axillary thermometry is standard in children. Axillary ≥37.5°C (99.5°F) = fever. Rectal temperature (most accurate for neonates) ≥38°C = fever. Tympanic thermometers are not recommended under 6 months.
Oxygen saturation (SpO₂):
- Peripheral pulse oximetry: normal ≥95% at sea level; <95% = significant hypoxaemia; <90% = severe. Pre- and post-ductal SpO₂ comparison is important in neonates (right hand = pre-ductal; foot = post-ductal) — a >3% difference suggests ductal-dependent circulation.