Page 21 of 31
PE22.{7-8,11} | Cardiovascular Examination Workflow — SDL Guide (Part 2)
Cardiovascular Examination Technique
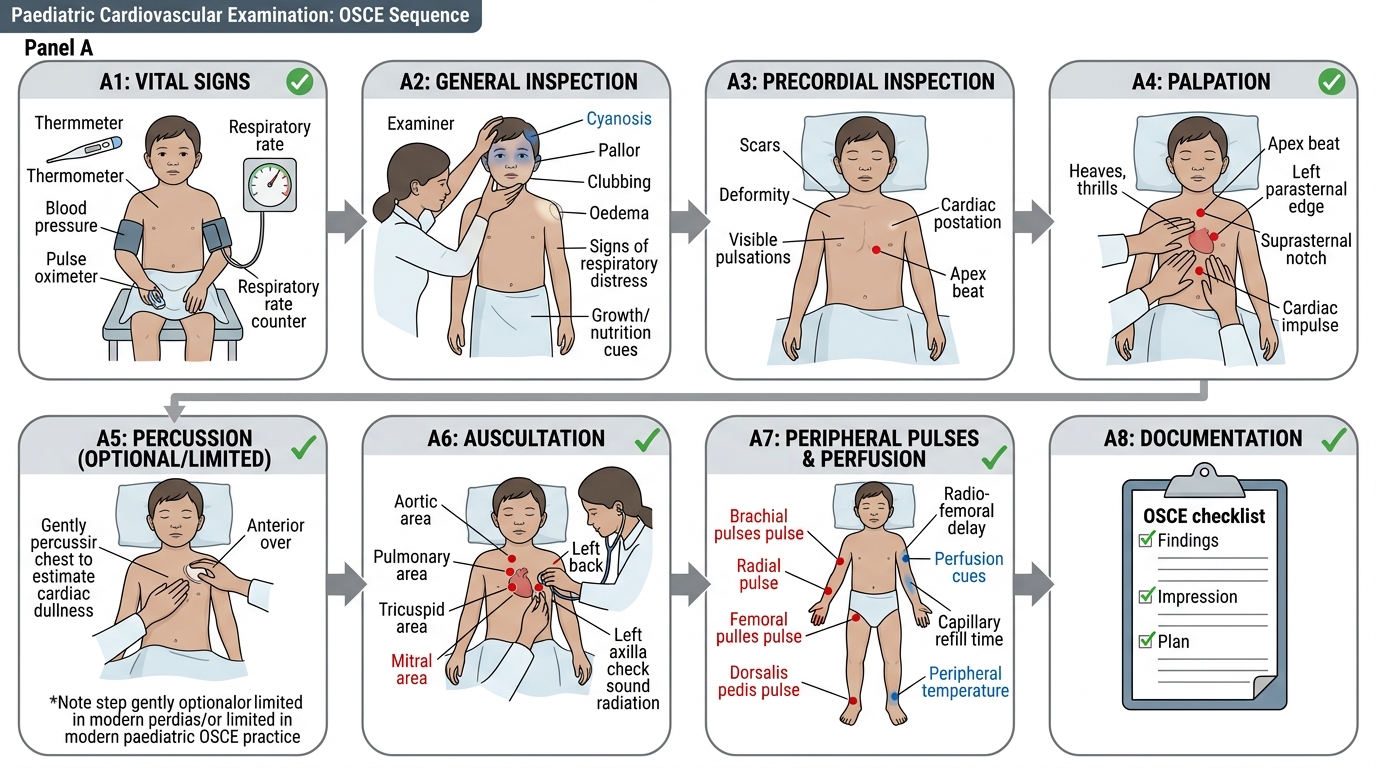
The cardiovascular examination in children follows the systematic IPPA sequence (Inspection → Palpation → Percussion → Auscultation), supplemented by peripheral vascular and venous assessment. In paediatric practice, this sequence often needs to be opportunistic — a skilled examiner auscultates when the child is quiet and calm, even if this means departing from the textbook order (auscultating before percussion, for instance, while the child is settled on the parent's lap). The full structured examination is ultimately completed systematically, but clinical flexibility is essential — a child who begins to cry during inspection cannot be reliably auscultated. The examination should begin as soon as the child enters the room: observe gait, colour, breathing, and behaviour before the child is aware of being examined. In acutely unwell children, the sequence should be adapted to prioritise the most diagnostically urgent components. The student is expected to be able to perform this examination independently on paediatric patients in a supervised clinical setting, applying each manoeuvre with correct technique and anatomical understanding.
1. Inspection:
Begin with a general inspection before touching the child. Look for:
- Cyanosis: central (tongue, mucous membranes — true hypoxaemia) vs peripheral (hands/feet only — may be normal in cool environments). Use your thumb to displace the tongue laterally to assess central cyanosis reliably.
- Respiratory distress: tachypnoea, subcostal/intercostal/suprasternal retractions, nasal flaring, head bobbing in infants
- Nutritional status and growth: failure to thrive is a classic presentation of haemodynamically significant cardiac disease in infants
- Dysmorphic features: Down syndrome (AV canal, VSD), Turner syndrome (coarctation, bicuspid aortic valve), Noonan syndrome (pulmonary stenosis, HCM), Marfan syndrome (aortic root dilatation, mitral valve prolapse)
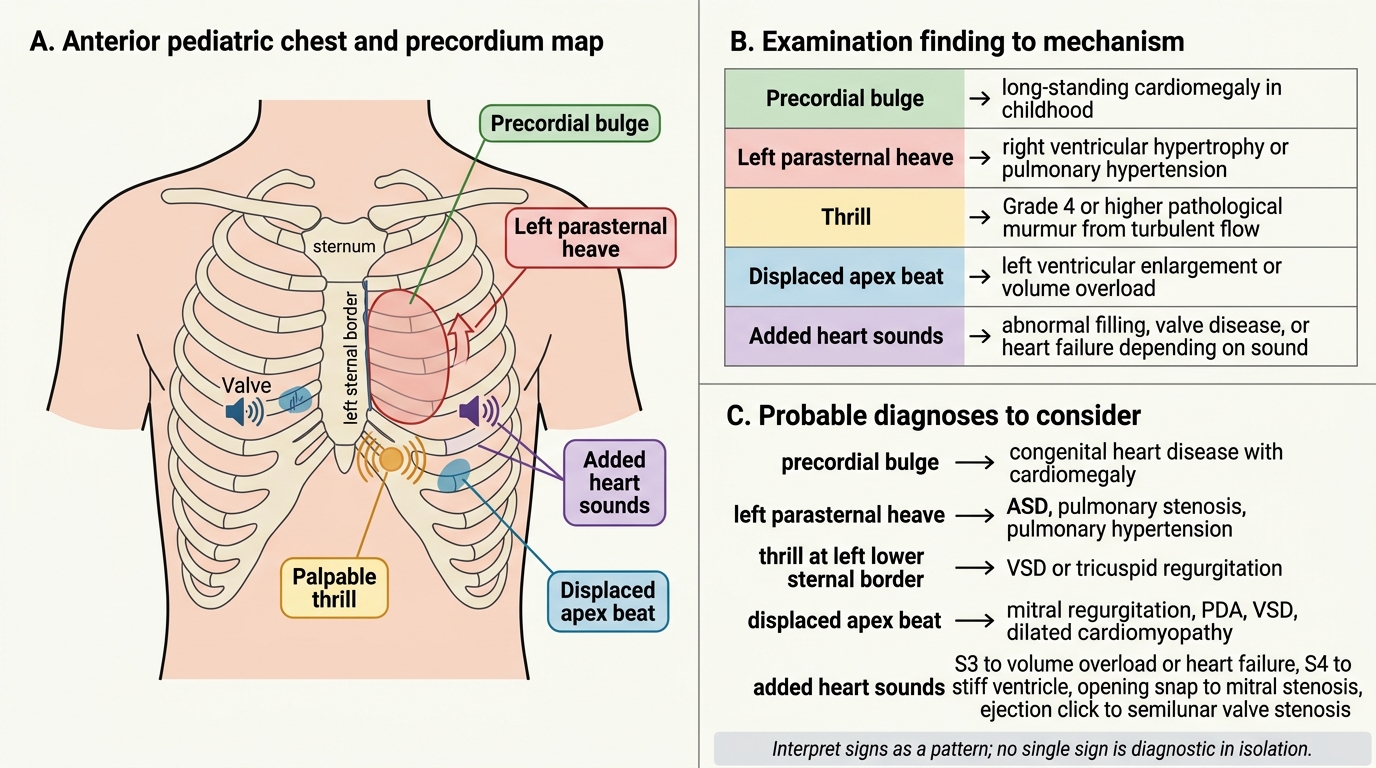
- Precordial bulge (precordial prominence): a visible bulge of the left precordium indicates cardiomegaly — most commonly caused by a large left-to-right shunt (VSD, PDA) or rheumatic heart disease. In a normal thin-chested child, mild precordial prominence may be normal; a marked bulge is significant.
- Visible pulsations: visible cardiac impulse over the precordium; visible pulsation in the suprasternal notch (aortic arch pulsation — prominent in hyperkinetic states, aortic regurgitation, coarctation).
2. Palpation:
- Apex beat: using the flat of the fingers, locate the point of maximum impulse (PMI). Normally at 4th ICS at or medial to MCL in children <7 years; 5th ICS at MCL in older children. A displaced apex (laterally/downward) indicates left ventricular dilatation or enlargement.
- Thrills: palpable vibrations from turbulent blood flow — equivalent to Grade 4+ murmur on the Levine scale. Felt as a fine sustained buzz under the fingers. Locate and characterise (systolic vs diastolic; site).
- Left parasternal heave: place the heel of the right hand along the left sternal border. A heave (sustained lifting impulse) indicates right ventricular hypertrophy or dilatation (e.g., pulmonary hypertension, ASD, large VSD with pulmonary HTN).
- Palpable P2: a palpable pulmonary component of S2 at the left 2nd intercostal space indicates pulmonary hypertension.
- Peripheral pulses: assess rate, rhythm, volume, and character bilaterally. Bounding pulse — patent ductus arteriosus, aortic regurgitation, severe anaemia. Weak thready pulse — shock, cardiac failure, severe AS. Radio-femoral delay — coarctation.
3. Percussion:
Percussion has a limited but relevant role in paediatric cardiovascular examination. It is less informative than in adults because the chest wall is thinner and resonance is more uniform. The primary uses are:
- Confirming cardiomegaly: percuss the left cardiac border — normally at or inside the midclavicular line. Dullness beyond the MCL suggests left heart enlargement.
- Detecting pericardial effusion: massive effusion may produce dullness in atypical areas.
- Detecting pleural effusion or pulmonary oedema in cardiac failure.
Note: echocardiography and chest X-ray are far more accurate for assessing cardiac size in children — percussion is a bedside screening technique.
4. Auscultation:
The most information-rich component of the CVS examination in children. Use the diaphragm (high-pitched sounds: S1, S2, aortic regurgitation, friction rub) and the bell (low-pitched sounds: S3, S4, mitral stenosis rumble) in a systematic sequence. Auscultate in at least four standard positions (aortic area, pulmonary area, tricuspid area, apex) and also in the axilla (mitral murmur radiation), the back (PDA, coarctation), and the neck (aortic stenosis radiation).
- S1: louder at apex and lower sternal border; a loud S1 with a short PR interval; soft S1 with first-degree AV block
- S2: at the upper left sternal border; listen specifically for splitting — physiological splitting widens with inspiration; fixed splitting = ASD; paradoxical (reversed) splitting = LBBB or severe AS
- A2-P2 relationship: normally A2 > P2. Loud P2 = pulmonary hypertension
- S3: low-pitched, early diastolic, at apex; physiological in children under 12; pathological in older children
- S4: always pathological; presystolic, at apex; ventricular hypertrophy
- Murmurs: characterise by timing (systolic vs diastolic vs continuous), site, intensity (Levine Grade 1–6), quality (harsh, blowing, musical, rumbling), radiation (neck for AS, axilla for MR, back for PDA/coarctation), and positional change
5. JVP Assessment:
Jugular venous pressure (JVP) assessment is useful in older children (>8–10 years) but is unreliable in infants and young children due to the short, chubby neck. In older children, use the hepatojugular reflux (HJR) — apply firm pressure to the right upper quadrant for 10–15 seconds; a rise in JVP by >3 cm indicates elevated right-sided filling pressure (right heart failure, constrictive pericarditis). Direct JVP measurement: position at 45°; the internal jugular vein column height above the sternal angle — >4 cm is elevated. JVP significance: elevated JVP + elevated hepatojugular reflux + right-sided heart failure = raised central venous pressure.
Abnormal CVS Examination Findings and Clinical Significance
SELF-CHECK
During cardiac auscultation, you detect a palpable thrill at the left lower sternal border. What does this signify?
A. A Grade 2 soft systolic murmur — likely innocent
B. A Grade 4 or higher murmur — likely pathological turbulent flow
C. Physiological S3 in a healthy child — no significance
D. Left parasternal heave indicating right ventricular hypertrophy
Reveal Answer
Answer: B. A Grade 4 or higher murmur — likely pathological turbulent flow
A thrill is a palpable vibration felt by the examining hand, corresponding to a Grade 4 or higher murmur on the Levine scale. It indicates high-velocity turbulent blood flow and is always pathological. Grade 1–2 murmurs are faint and may be innocent; Grade 3 is clearly audible but without thrill; Grade 4 and above have a palpable thrill. A palpable thrill at the left lower sternal border in a child is a strong pointer to a ventricular septal defect or other significant turbulence at the tricuspid area.
Interpretation of Findings
Interpreting cardiovascular examination findings requires correlating multiple signs into a coherent clinical picture. No single sign is diagnostic in isolation — the pattern of findings, in the context of the child's age and clinical presentation, guides diagnosis and the urgency of referral.
Precordial bulge and pulsations: A visible, prominent precordial bulge in a young child almost always indicates cardiomegaly from longstanding cardiac enlargement — most commonly a large ventricular or atrial septal defect, patent ductus arteriosus, or rheumatic valvular disease. The chest wall remodels over time in response to the enlarged heart beneath it. A newly prominent precordium in a previously normal child warrants urgent evaluation.
Apex displacement: The apex beat displaced laterally beyond the MCL indicates left ventricular dilatation (dilated cardiomyopathy, severe MR, severe AR). The apex displaced downward AND laterally indicates gross left ventricular enlargement.
Murmur grading — Levine scale:
| Grade | Description | Thrill? |
|---|---|---|
| 1 | Very faint — only heard in ideal conditions by an expert | No |
| 2 | Soft but heard by most listeners | No |
| 3 | Moderate, easily audible | No |
| 4 | Loud | Yes |
| 5 | Very loud — heard with stethoscope partially off chest | Yes |
| 6 | Heard without stethoscope | Yes |
Grade 1–2 murmurs without other signs are frequently innocent in children. Grade 3+ murmurs, diastolic murmurs, or any murmur with added features (thrill, click, abnormal S2, associated symptoms) are pathological until proven otherwise.
Innocent vs pathological murmurs:
Innocent (functional) murmurs are extremely common in children — estimated to occur in up to 80% of children at some point. Key features that characterise an innocent murmur (the '8 S's' mnemonic — Soft, Short, Systolic, Single [no clicks/added sounds], no Symptoms, no Sternal lift, no Spread/radiation, no Signs): soft (Grade 1–2), short midsystolic, heard best at the left sternal border or pulmonary area, musical or vibratory quality, diminishes with standing or Valsalva, no radiation, no thrill, no associated abnormal S2. Still's murmur (vibratory, low-pitched, heard at lower left sternal border in 2–7 year olds) is the most common innocent murmur in children.
Abnormal S2: Fixed splitting = ASD (right heart volume overload prevents S2 variation with respiration). Wide splitting without fixation = RBBB, pulmonary stenosis. Reversed splitting = severe AS, LBBB. Loud P2 = pulmonary hypertension. Single S2 = severe AS or PS with immobile valve.
Left parasternal heave: Right ventricular hypertrophy or dilatation — seen with pulmonary hypertension, large left-to-right shunts (ASD, VSD), pulmonary stenosis.
JVP significance in children: Elevated JVP (and positive hepatojugular reflux) indicates raised right heart filling pressure — right ventricular failure, constrictive pericarditis, cardiac tamponade, or superior vena caval obstruction. In infants, hepatomegaly is a more reliable sign of right heart failure than JVP.
Radio-femoral delay: Femoral pulse arrives after radial pulse — pathognomonic of coarctation of the aorta. Confirm by measuring BP in all four limbs — systolic BP >10 mmHg higher in the arm than the leg is significant.
CLINICAL PEARL
Innocent vs pathological murmur — the most important differentiation in paediatric cardiology bedside examination. A diastolic murmur is NEVER innocent — all diastolic murmurs in children are pathological and require echocardiographic evaluation. A murmur that radiates to the neck (consider aortic stenosis), to the back (consider PDA or coarctation), or to the axilla (consider mitral regurgitation) is not innocent. Conversely, a soft, short, systolic, vibratory murmur at the left lower sternal border in an otherwise well child with normal S2 and no symptoms is almost certainly innocent — Still's murmur — and does not require echocardiography unless clinical uncertainty persists. Never reassure a parent with 'it's probably nothing' — say: 'This is a very soft murmur that has the characteristics of an innocent one, but I will refer for a heart ultrasound to confirm.' This is both clinically correct and communicates appropriate care.
Applied Practice and Communication
Applying cardiovascular examination skills in clinical practice involves not only technical proficiency but also the ability to communicate findings with sensitivity and empathy — particularly when the findings are unexpected or potentially alarming. Competency PE22.11 specifically requires the student to 'demonstrate empathy while dealing with children with cardiac diseases in every patient encounter.' This is an affective-domain competency that must be actively practised at every clinical encounter, not merely learned from a textbook. Empathy in this context means recognising that a diagnosis of congenital heart disease — or even the possibility of it — can cause profound distress to a family, and that the way a clinician communicates is as important as the information conveyed. Research in paediatric communication consistently shows that families remember how they were told about a diagnosis long after they have forgotten the clinical details. Students who practise deliberately empathic communication from their early clinical years develop a skill that becomes increasingly natural and effective over time, leading to better family engagement, improved adherence to management plans, and reduced parental anxiety.
Practical steps for empathic communication with the child during examination:
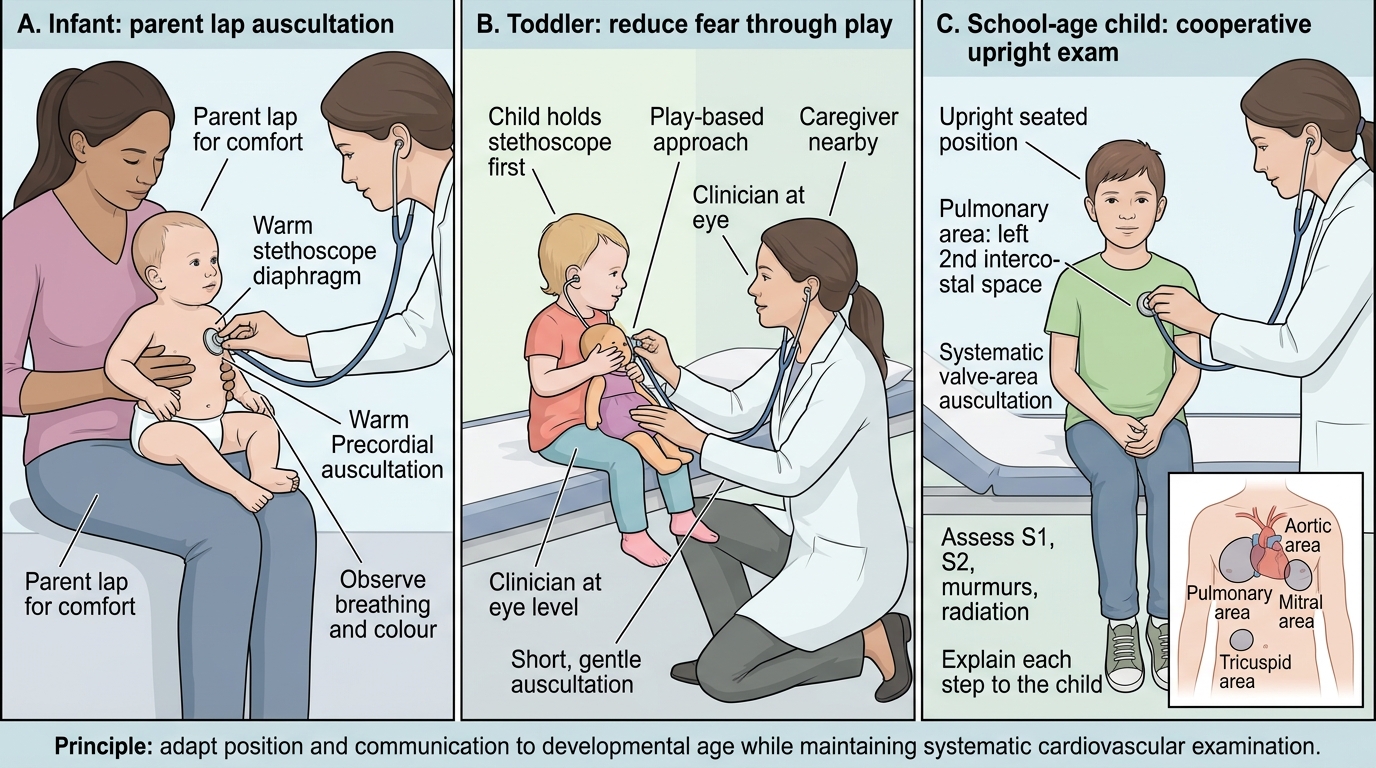
Children vary enormously in their willingness to cooperate with physical examination. A systematic, developmentally-appropriate approach reduces distress and improves examination quality:
- Infants (0–12 months): Examine on the parent's lap whenever possible. Auscultate before other manoeuvres, as infants quieten when held and suckling. Use a warm stethoscope. Avoid prolonged supine positioning.
- Toddlers (1–3 years): This age group is the most challenging. Approach very slowly; demonstrate the stethoscope on a toy first. Distraction (songs, pointing to the window) can facilitate examination. Never force the child down — this causes crying and makes auscultation impossible.
- School-age children (6–12 years): Explain what each part of the examination involves, e.g. 'I'm going to listen to your heart beating — you'll hear a lub-dub sound.' Involve them as 'helpers' — ask them to hold still and breathe normally. They generally cooperate well when respected and given information.
- Adolescents: Ensure privacy. Ask for parental presence only if the adolescent consents. Explain all procedures. Respect gender-specific sensitivities during examination of the precordium.
Communicating findings to parents:
Parents of children with cardiac murmurs or abnormal findings experience acute anxiety. Communication should be factual, jargon-free, and compassionate:
- State what you have found clearly: 'I have detected a murmur — a sound made by blood flowing through the heart. Many murmurs in children are completely innocent, but I want to investigate further to be certain.'
- Avoid creating unfounded alarm ('I think there might be a hole in the heart') before investigations are completed.
- Explain the next step clearly: 'We will arrange an echocardiogram (heart ultrasound) to look at the heart structure in detail.'
- Allow parents to ask questions and express concerns; actively listen without interrupting.
- For children already diagnosed with congenital heart disease, every encounter should reinforce understanding of the condition, the treatment plan, and warning signs.
Documentation of CVS examination findings should follow a standard structure:
1. Vital signs (pulse rate, BP with percentile interpretation, RR, SpO₂, temperature)
2. General inspection: cyanosis, dysmorphic features, nutritional status
3. Precordial inspection: bulge, visible pulsations, apex beat location
4. Palpation: apex beat position, thrills (site, timing), heaves
5. Percussion: cardiac dullness (if performed)
6. Auscultation: S1, S2 (splitting, intensity), added sounds (S3, S4, clicks), murmurs (timing, site, grade, quality, radiation)
7. Peripheral pulses and JVP
8. Summary interpretation and plan
Age-Appropriate Paediatric Cardiovascular Examination
SELF-CHECK
A 6-year-old girl has a Grade 2/6 midsystolic murmur at the pulmonary area with no radiation, normal S2, no thrill, no symptoms, and normal chest X-ray. What is the most appropriate next step?
A. Urgent echocardiography and cardiology referral — all murmurs require investigation
B. Reassure that this is likely an innocent murmur; consider echocardiography if clinical uncertainty persists
C. Start prophylactic penicillin for rheumatic heart disease prevention
D. Order a 24-hour Holter monitor for arrhythmia detection
Reveal Answer
Answer: B. Reassure that this is likely an innocent murmur; consider echocardiography if clinical uncertainty persists
This murmur has the classic features of an innocent murmur: soft (Grade 2), short, systolic, at the pulmonary area, no radiation, normal S2, no thrill, no symptoms. Innocent murmurs are extremely common in children — up to 80% have one at some point. The appropriate response is to reassure the parents about the likely benign nature while acknowledging clinical uncertainty and offering echocardiography to confirm. Urgent referral is not required; penicillin prophylaxis is not indicated without evidence of rheumatic disease; Holter monitoring is not indicated for a murmur without arrhythmia symptoms.
Self-Assessment
Apply your knowledge of cardiovascular examination skills to the following clinical scenarios. Work through each case before reading the analysis.
Scenario 1: You examine a 3-year-old boy and find: pulse 118/min regular, BP 92/60 mmHg (75th percentile for age), RR 28/min, SpO₂ 98%. Precordium: no visible bulge; apex beat at 4th ICS just medial to MCL. A Grade 3/6 harsh pansystolic murmur is heard best at the lower left sternal border, radiating towards the apex. No thrill. S2 normal.
Analysis: Grade 3 pansystolic murmur at the lower sternal border in a young child = ventricular septal defect (VSD) until proven otherwise. No thrill (Grade <4), normal S2 (no pulmonary hypertension yet), SpO₂ normal (no right-to-left shunting). Refer for echocardiography. This is not an innocent murmur — pansystolic, Grade 3, and anatomically consistent with VSD.
Scenario 2: A 10-year-old girl presents with easy fatigability. BP right arm 135/85 mmHg (>99th percentile). BP left arm 132/84 mmHg. You palpate the femoral pulses — they are weak and feel delayed compared with the radial. RR 18/min, SpO₂ 97%.
Analysis: BP significantly elevated for age on percentile tables. Weak, delayed femoral pulses = radio-femoral delay = coarctation of the aorta until proven otherwise. Measure BP in both legs — expected to be significantly lower than arms in coarctation. Urgent referral to paediatric cardiology; echocardiography and CT/MR aortography.
Scenario 3: A mother brings her 7-year-old son because her neighbour (a nurse) heard a heart murmur at a family function. On examination: pulse 88/min, BP 96/60 mmHg, RR 20/min, SpO₂ 99%. Precordium: no bulge. Apex beat 5th ICS at MCL. Grade 1–2 short midsystolic vibratory murmur at the lower left sternal border, no radiation, normal S2, no thrill, no symptoms. Mother is extremely anxious.
Analysis: Classic Still's murmur — the most common innocent murmur in school-age children. All features are reassuring. Address the mother's anxiety directly: explain that this type of murmur is very common, that the heart sounds are otherwise completely normal, and that an echocardiogram can be arranged if she remains concerned. Communicate with warmth and clarity.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Paediatric Cardiovascular Examination OSCE Checklist