Page 23 of 31
PE22.9-10 | Cardiovascular Investigations — SDL Guide
Learning Objectives
- State the clinical indications for ordering a chest X-ray (CXR) and ECG in children with suspected cardiovascular disease
- Describe the anatomical basis of cardiac shadows and electrical signals that underpin CXR and ECG interpretation
- Perform a systematic interpretation of a paediatric chest X-ray, recognise cardiomegaly by calculating the cardiothoracic (CT) ratio, and identify abnormal pulmonary vascular patterns
- Apply a structured framework for paediatric ECG interpretation — rate, rhythm, axis, intervals, waveform — and distinguish normal paediatric variants from pathological findings
- Recognise ECG patterns of ventricular hypertrophy, AV block, prolonged QT, and common congenital heart disease in children
INSTRUCTIONS
The chest X-ray and ECG are the two most accessible, cost-effective, and widely available cardiovascular investigations in any clinical setting. A clinician who can reliably interpret a paediatric CXR and ECG can detect cardiomegaly, pulmonary plethora, right ventricular hypertrophy, complete heart block, or a prolonged QT interval at the bedside — each of which has immediate diagnostic and management implications. The paediatric ECG is not a 'smaller adult ECG': its normal reference ranges differ significantly by age, and several patterns that would be pathological in an adult are entirely normal in an infant. Mastering these distinctions is a specific, learnable skill that this module trains through systematic framework and applied practice.
References
- Ghai Essential Pediatrics, 9th ed., Ch 14 (Cardiovascular System) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 454 (Laboratory Investigations in Heart Disease) (textbook)
- Moss & Adams Heart Disease in Infants, Children and Adolescents, 9th ed. (textbook)
- IAP Standard Treatment Guidelines — Paediatric Cardiology (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old boy is referred to you from a peripheral health centre with a note: 'Murmur noted, please investigate.' You perform a full examination — the child has a Grade 3/6 pansystolic murmur at the lower left sternal border, mild tachypnoea, and is noted to be slightly underweight. You order a CXR and ECG. The CXR shows an enlarged cardiac shadow with increased pulmonary vascular markings. The ECG shows right-axis deviation with R waves dominant in the right precordial leads. What do you see on this CXR, and what does this ECG pattern suggest about the haemodynamic state of this child's heart?
WHY THIS MATTERS
The chest X-ray and ECG are universal investigations available even in basic district hospital settings — unlike echocardiography, which requires trained technicians and expensive equipment. In India, where the paediatric cardiology subspecialty is unevenly distributed, these two investigations are the first-line diagnostic tools in any child with suspected cardiac disease. The ability to identify cardiomegaly on a CXR and recognise right ventricular hypertrophy on an ECG can change a management decision — whether to refer urgently, initiate diuretic therapy, or pursue further investigation. For a newly qualified doctor working at a primary or secondary care level, this skill is not optional; it is frequently the only cardiac investigation available.
RECALL
Before proceeding, activate the following prior knowledge: (1) Cardiac anatomy: the right ventricle forms the anterior surface and left sternal border; the left ventricle forms the left cardiac border and apex; the right atrium forms the right cardiac border; the aortic arch and pulmonary artery knuckle are visible on the left side of the mediastinum. (2) Cardiac electrical conduction: the SA node (right atrium) generates the P wave; the AV node and Bundle of His delay conduction; left and right bundle branches generate the QRS complex; ventricular repolarisation produces the T wave. (3) Foetal circulation: the right ventricle pumps against pulmonary vascular resistance in foetal life, making it dominant — this produces the right-axis deviation and right ventricular dominance seen in neonatal ECGs. (4) Cardiothoracic (CT) ratio = widest cardiac shadow / widest internal diameter of thoracic cage — measured on a standard inspiratory PA chest X-ray.
Clinical Indications for Cardiovascular Investigations
Cardiovascular investigations — particularly the chest X-ray and ECG — should be ordered in a purposeful, hypothesis-driven manner based on the clinical assessment rather than as routine investigations for every child. Understanding when each investigation adds diagnostic value is an important part of clinical reasoning. In paediatric practice, where the clinical examination is often challenging (an uncooperative toddler, a murmur heard through crying), the CXR and ECG extend the examination and provide objective structural and electrical information that cannot be inferred from auscultation alone. A CXR and ECG ordered without a pre-test hypothesis do not replace clinical examination; rather, they confirm, extend, or refute the working diagnosis formed at the bedside. The clinician must therefore formulate a clinical question before ordering: is this cardiomegaly due to a shunt or cardiomyopathy? Is this child's tachycardia sinus tachycardia or an arrhythmia? Each investigation then answers a specific question rather than generating findings to be interpreted without context.
Indications for a Chest X-Ray (CXR) in suspected cardiac disease:
- Detection or confirmation of cardiomegaly (enlarged cardiac shadow)
- Assessment of pulmonary vascular markings — increased (left-to-right shunt), decreased (right-to-left shunt), or pulmonary oedema (cardiac failure)
- Identification of specific cardiac silhouette shapes associated with cardiac anomalies (e.g. 'egg-on-string' in transposition, 'boot-shaped' in tetralogy of Fallot, 'snowman' in total anomalous pulmonary venous connection)
- Assessment of situs (cardiac position — situs solitus, inversus, or ambiguus)
- Detection of associated thoracic abnormalities — pleural effusions, atelectasis, rib notching (coarctation of aorta — seen in older children)
- Pre-operative baseline and post-intervention follow-up
Indications for an ECG in paediatric cardiac disease:
- Evaluation of arrhythmias — palpitations, syncope, bradycardia, tachycardia
- Detection of ventricular hypertrophy — assessment of the haemodynamic load on each ventricle
- Screening for conduction defects — AV block, bundle branch block, pre-excitation (Wolff-Parkinson-White)
- Prolonged QT syndrome screening — family history, syncope during exercise, QT-prolonging drugs
- Baseline assessment before starting QT-prolonging medications
- Children with Down syndrome, Williams syndrome, or other syndromes with cardiac associations
- Following cardiac surgery or in known congenital heart disease — monitoring for new conduction abnormalities
- Chest pain, unexplained syncope or exercise intolerance
Both investigations complement clinical examination: the CXR provides structural information about chamber size, pulmonary vascularity, and great vessel position, while the ECG provides functional information about the electrical conduction, chamber thickness (hypertrophy voltages), rhythm, and rate.
Normal Paediatric Cardiac Borders and Cardiothoracic Ratio
Anatomy and Technical Principles
Interpreting cardiovascular investigations correctly requires a clear mental model of the anatomical structures that generate the visible shadows on a CXR and the electrical signals on an ECG. Without this anatomical grounding, the findings cannot be reliably linked to pathological processes — a student who sees cardiomegaly on a CXR but cannot identify which border is enlarged, or who sees a tall R wave in V1 but does not know which ventricle this represents, cannot translate the investigation into a diagnostic conclusion. This section provides the anatomical and physiological foundations that make interpretation systematic rather than pattern-recognition based. The two key principles to hold in mind are: (1) on the CXR, the cardiac borders correspond to specific chambers and great vessels, and enlargement of a border localises the affected chamber; and (2) on the ECG, the voltage and polarity of QRS complexes in the precordial leads reflect the relative mass of the right vs left ventricle — a relationship that changes dramatically with age in children.
Provided image
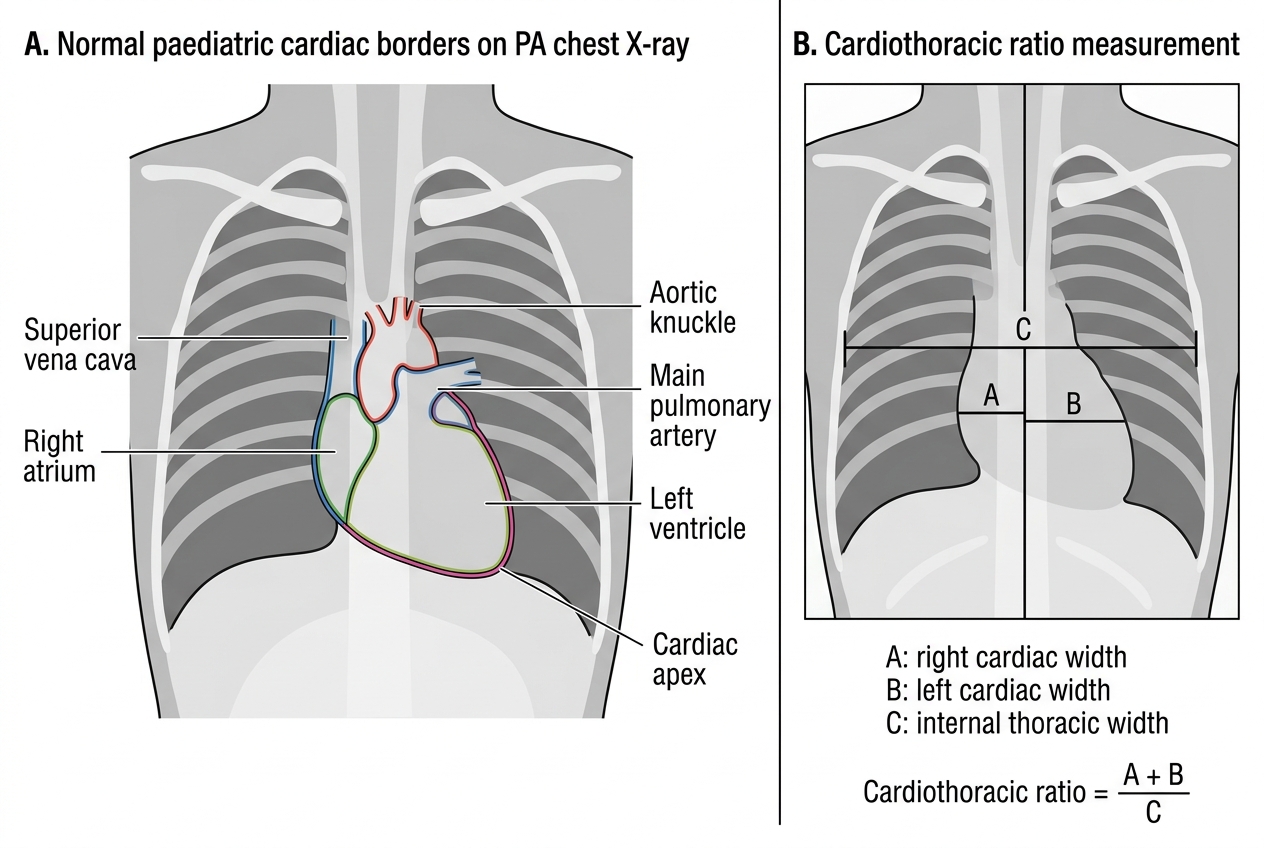
Anatomical basis of the cardiac silhouette on CXR:
The cardiac shadow on a CXR represents the outer silhouette of the cardiac chambers and great vessels in contact with the air-filled lung. Different borders of the cardiac shadow correspond to specific structures:
- Right cardiac border (from top to bottom): superior vena cava (SVC) — right atrium. Enlargement of the right atrium widens the right cardiac border.
- Left cardiac border (from top to bottom): aortic knuckle (aortic arch) — pulmonary artery trunk — left atrial appendage (normally not visible) — left ventricle (forms the majority of the left border and the apex).
- The apex is the lowest leftward point of the cardiac shadow; it represents the left ventricle in situs solitus.
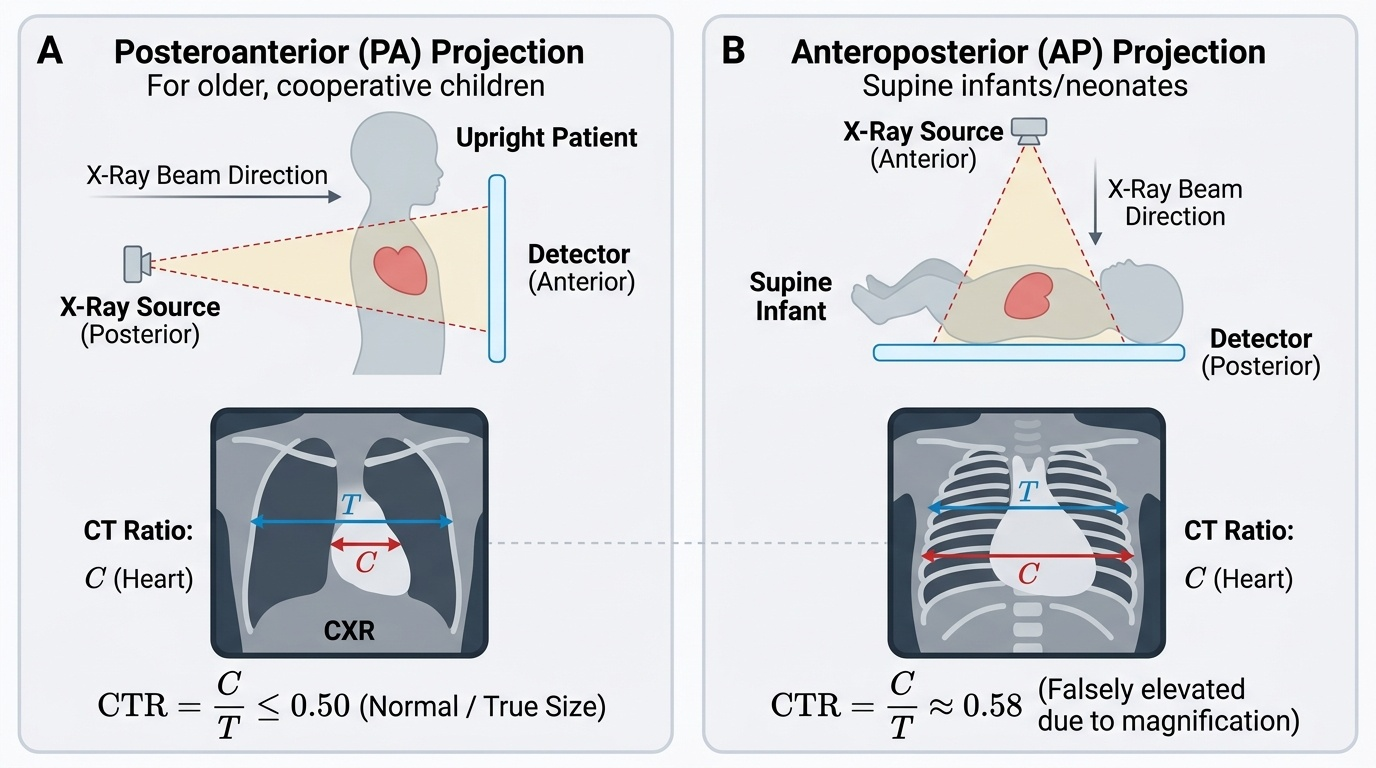
PA vs AP projection — critical for CT ratio assessment:
A posteroanterior (PA) view (standard in cooperative older children and adults — patient stands, X-ray beam from back to front, detector in front) produces a smaller cardiac magnification. A anteroposterior (AP) view (used in infants, ill children, and neonates who cannot stand — X-ray beam from front to back) magnifies the cardiac shadow, making the CT ratio appear larger than the true size. This is clinically important: a CT ratio of 0.58 in an infant on an AP film may be normal magnification rather than true cardiomegaly. Always note the projection before interpreting the CT ratio.
Electrical conduction anatomy and ECG waveforms:
The ECG records the sum of all electrical activity generated by cardiac muscle depolarisation and repolarisation:
- P wave: atrial depolarisation, originating from the SA node in the right atrium. Normal P wave is upright in leads I, II, and aVF (reflecting normal left-to-right, superior-to-inferior spread).
- PR interval: time from onset of atrial depolarisation to onset of ventricular depolarisation — includes the AV nodal delay. Prolongation = AV block.
- QRS complex: ventricular depolarisation. The initial Q wave = septal depolarisation (left to right); the R wave = dominant ventricular free-wall depolarisation; the S wave = basal ventricular depolarisation. The QRS morphology in the precordial leads reflects the relative dominance of the right vs left ventricle — right-sided leads (V1, V2) normally show a dominant R wave when the right ventricle is thicker (as in the neonate), and a dominant S wave when the left ventricle is thicker (as in the adult).
- T wave: ventricular repolarisation. T wave polarity is determined by the direction of repolarisation.
- QT interval: total duration of ventricular systole — from onset of QRS to end of T wave. Rate-corrected using the Bazett formula: QTc = QT / √RR (RR in seconds). Normal QTc < 0.44 s in children.
SELF-CHECK
An infant's chest X-ray was taken as an AP (anteroposterior) view. The cardiothoracic (CT) ratio measures 0.60. What is the most appropriate interpretation?
A. This infant has definite cardiomegaly requiring urgent echocardiography
B. The CT ratio on an AP view appears magnified; 0.60 may be within normal limits for an AP infant film
C. Normal CT ratio in infants is >0.65, so this child is normal
D. CT ratio is only valid on lateral views in children under 2 years
Reveal Answer
Answer: B. The CT ratio on an AP view appears magnified; 0.60 may be within normal limits for an AP infant film
The AP projection magnifies the cardiac shadow compared to the standard PA view. In infants, a CT ratio of up to 0.60 on an AP film can be within normal limits, partly due to this magnification effect. The threshold for cardiomegaly in infants on an AP view is generally >0.60; on a PA view in children >2 years, cardiomegaly is CT ratio >0.55. Always note the projection before interpreting the CT ratio, and use clinical context (examination findings, symptoms) to guide the significance of the measurement.
Chest X-Ray Interpretation — Technique and Normal Anatomy
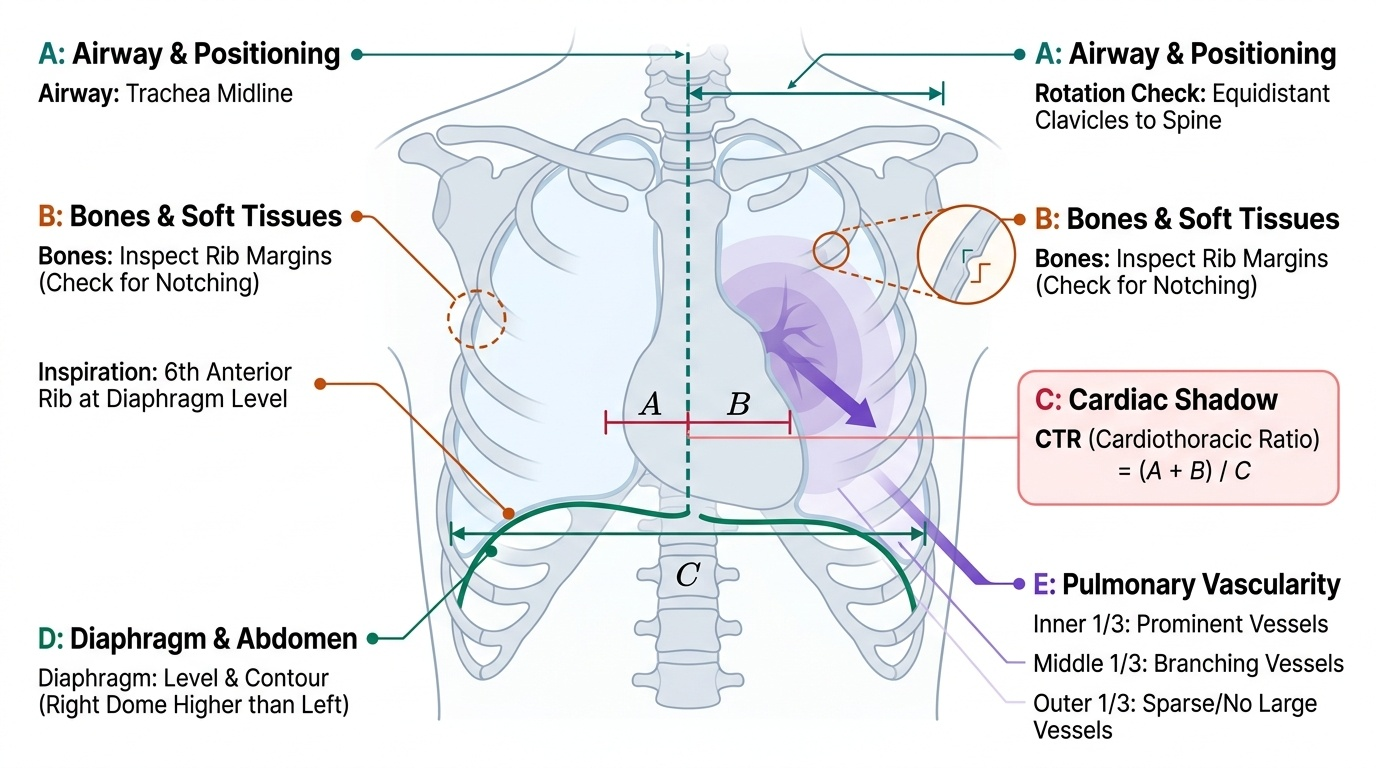
A systematic approach to paediatric CXR interpretation ensures that no important finding is missed and that findings are correctly attributed to their anatomical source. The recommended systematic review uses the ABCDE approach (Applied to Paediatric CXR: Airway/Position → Bones and soft tissues → Cardiac shadow → Diaphragm and abdomen → Everything else/Lung fields). Using a consistent, step-by-step framework prevents the common error of jumping to the most obvious abnormality (e.g., the large cardiac shadow) and missing a co-existing finding (e.g., a small pleural effusion or rib notching). In an examination setting, a structured report that addresses all components is expected and is scored in full. In clinical practice, a missed rib notching means a missed diagnosis of coarctation; a missed pulmonary oligaemia means a missed cyanotic cardiac lesion. The clinical stakes of a disorganised approach are high — systematic reporting is both an examination skill and a patient-safety habit.
Provided image
Step 1 — Assess quality and positioning:
Before interpreting a CXR, assess whether it is technically adequate. An inadequate film can produce false findings:
- Rotation: the clavicular heads should be equidistant from the spinous processes of the vertebrae. Rotation makes the cardiac shadow appear deviated — a common pitfall.
- Inspiration: on a good inspiratory film in children, the anterior end of the 6th rib should be at the level of the diaphragm. An expiratory film will make the heart appear larger and the lung fields hazier.
- Projection: PA or AP (see above).
Step 2 — Airway and mediastinum:
- Is the trachea midline? Deviation may be caused by thyroid enlargement, pleural effusion, or pneumothorax pulling or pushing the mediastinum.
- Assess the mediastinal width — widening suggests aortic root dilatation, mediastinal mass, or vascular anomaly.
- Check situs: is the cardiac apex on the left (situs solitus — normal) or right (dextrocardia/situs inversus)?
Step 3 — Cardiac shadow:
- Size: calculate the cardiothoracic (CT) ratio = horizontal diameter of the cardiac shadow / horizontal diameter of the thoracic cage (inner rib cage at its widest). Normal: ≤0.55 in children >2 years (PA view); ≤0.60 in infants (AP view). Cardiomegaly = CT ratio exceeding these thresholds.
- Shape: the overall silhouette can suggest specific lesions (see Cardiomegaly section).
- Right border: examine for right atrial enlargement (prominent right cardiac border) or SVC dilatation.
- Left border: examine the aortic knuckle (absent in right-sided aortic arch), pulmonary artery segment (prominent in pulmonary hypertension or pulmonary artery dilatation — a convex left heart border), and left ventricular outline.
- Cardiac apex: upturned apex (right ventricular enlargement); prominent/rounded apex (left ventricular enlargement).
Step 4 — Lung fields and pulmonary vascularity:
The pulmonary vascular pattern is one of the most diagnostically useful aspects of the paediatric CXR:
- Normal: vessels visible to the outer third of the lung; vessels taper from hilum to periphery.
- Pulmonary plethora (increased vascularity): vessels prominent, extending to the periphery; hazy or indistinct lung fields. This indicates increased pulmonary blood flow — the hallmark of significant left-to-right shunts (ASD, VSD, PDA). The hila are prominent and vascular markings are visible in areas where they are normally sparse.
- Pulmonary oligaemia (decreased vascularity): vessels are reduced, lung fields appear dark/hyperlucent. This indicates reduced pulmonary blood flow — as in critical pulmonary stenosis, pulmonary atresia, or tetralogy of Fallot with significant right-to-left shunting.
- Pulmonary oedema: bilateral perihilar haziness, Kerley B lines (short horizontal lines at the lung bases indicating engorged lymphatics), fluffy bilateral infiltrates — seen in cardiac failure with elevated pulmonary venous pressure.
Step 5 — Bony structures:
Rib notching (bilateral inferior rib scalloping, ribs 3–8) is a classical sign of coarctation of the aorta in children older than 5 years — caused by enlarged collateral intercostal arteries eroding the rib undersurfaces. Not seen in young infants with coarctation.