Page 24 of 31
PE22.9-10 | Cardiovascular Investigations — SDL Guide (Part 2)
Recognising Cardiomegaly and Abnormal CXR Patterns
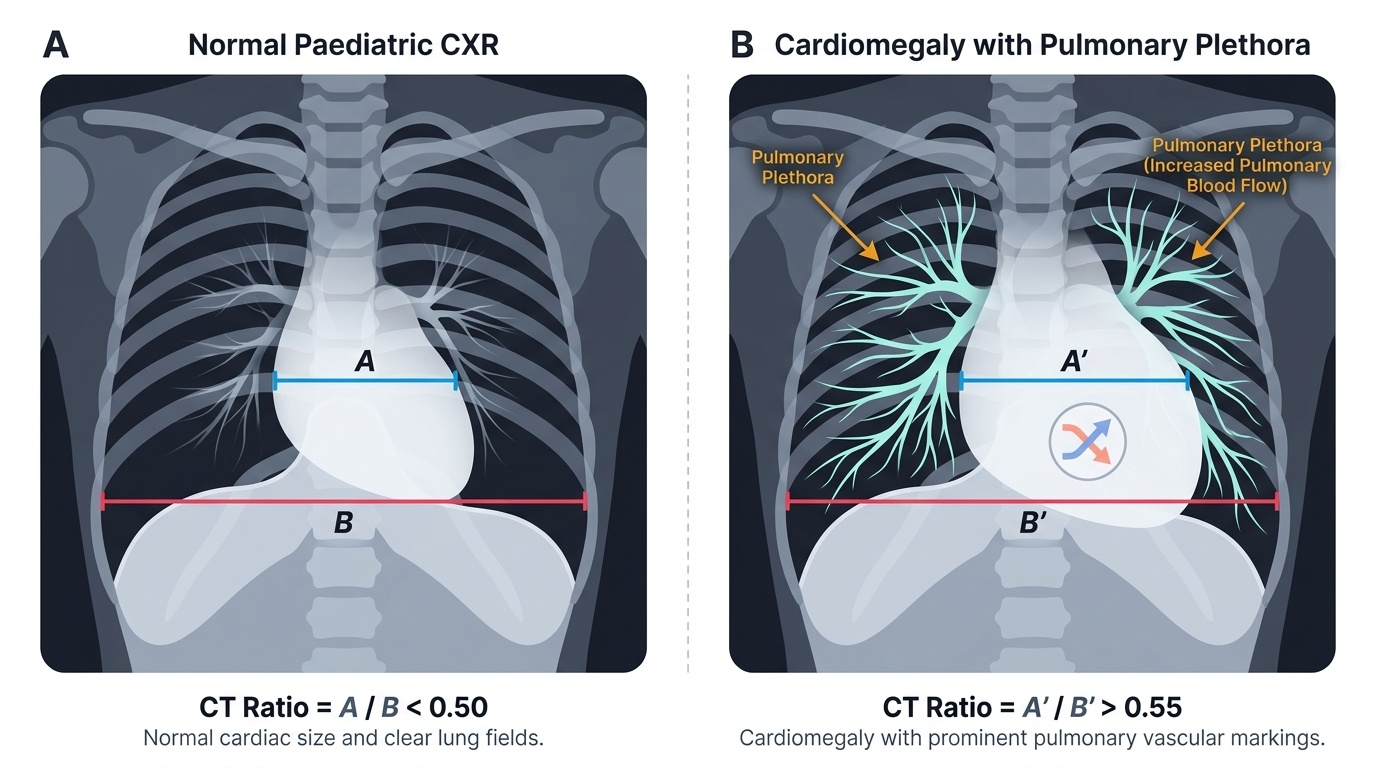
Cardiomegaly is defined as a cardiothoracic (CT) ratio >0.55 on an adequate inspiratory PA chest X-ray in children older than 2 years, or >0.60 on an AP film in infants. However, the CT ratio is a screen — it reflects total cardiac shadow width, not which chamber is enlarged. Specific chamber enlargement patterns are identified by analysing which cardiac border is abnormally prominent.
Provided image
CT ratio calculation:
Measure the widest horizontal diameter of the cardiac shadow (from the most rightward point of the right cardiac border to the most leftward point of the left cardiac border). Measure the widest internal thoracic diameter (inner to inner) at the same level. Divide: CT ratio = cardiac diameter ÷ thoracic diameter. A CT ratio >0.55 in a good inspiratory PA film in a child >2 years = cardiomegaly requiring further evaluation.
Right ventricular enlargement: upturned cardiac apex; loss of the concavity of the pulmonary artery segment (prominent bulge on the left heart border in the position of the pulmonary artery); left parasternal heave on clinical examination. Seen in pulmonary hypertension, ASD, large VSD, pulmonary stenosis.
Left ventricular enlargement: the cardiac apex is displaced downward and to the left; the left cardiac border becomes more convex. Seen in large VSD with volume overload, aortic stenosis, dilated cardiomyopathy, aortic regurgitation.
Left atrial enlargement: in severe cases, the left atrial appendage bulges below the pulmonary artery segment on the left heart border; on the right side, a double cardiac shadow (right atrial border appears doubled) indicates a large left atrium projecting beyond the right atrium. In a lateral CXR, the oesophagus is displaced posteriorly by an enlarged left atrium. Classic cause: mitral stenosis from rheumatic heart disease.
Specific silhouette patterns in congenital heart disease:
- Tetralogy of Fallot: 'boot-shaped' heart (coeur en sabot) — upturned apex (RV hypertrophy), concave pulmonary artery segment (small pulmonary artery), normal/slightly small cardiac size, decreased pulmonary vascularity (pulmonary oligaemia).
- Transposition of the great arteries (TGA): 'egg-on-string' or 'egg-on-side' appearance — narrow superior mediastinum (because aorta is anterior and pulmonary artery posterior, giving a narrow mediastinal shadow at the base), increased pulmonary vascularity.
- Total Anomalous Pulmonary Venous Connection (TAPVC) — supracardiac type: 'snowman' or 'figure-of-eight' appearance — a large vertical vein ascending on the left and the SVC on the right form the 'head' of the snowman; the cardiac shadow forms the 'body'.
- Ebstein's anomaly: massive cardiomegaly with a box-shaped or 'wall-to-wall' heart — the right atrium is hugely dilated; decreased pulmonary vascularity.
Pulmonary vascular patterns as a diagnostic tool:
Increased pulmonary vascularity (plethora) + cardiomegaly = large left-to-right shunt (VSD, ASD, PDA, AVSD). If this combination exists without cyanosis, the shunt is left-to-right and pulmonary hypertension may develop over time (Eisenmenger syndrome — when the shunt eventually reverses).
CLINICAL PEARL
The 'boot-shaped heart' of Tetralogy of Fallot with decreased pulmonary vascularity is one of the most tested CXR patterns in paediatric cardiology. Remember: in Fallot, the cardiac silhouette is NOT necessarily enlarged — the hallmark is the shape (upturned apex from RV hypertrophy, concave pulmonary bay from small pulmonary artery) combined with REDUCED pulmonary vascularity. This is the opposite of a left-to-right shunt, which gives INCREASED vascularity and cardiomegaly. Memorise the pairings: increased vascularity + cardiomegaly = left-to-right shunt; decreased vascularity + right-sided shape = right-to-left shunt (cyanotic CHD). On the ECG side: a normal T wave in V1 is actually ABNORMAL in neonates — T wave should be inverted in V1 before age 8. An upright T in V1 in a neonate suggests right ventricular hypertrophy or ischaemia.
Paediatric ECG — Normal Variants and Interpretation Framework
The paediatric ECG has age-specific normal values that differ substantially from adult norms, and several findings that would prompt urgent investigation in an adult are entirely normal and expected in a neonate or young infant. The most important conceptual framework is that the neonatal right ventricle is physiologically dominant — it has been working against high pulmonary vascular resistance during foetal life, so it is thicker and generates greater electrical voltage than the left ventricle at birth. This dominance gradually reverses as pulmonary vascular resistance falls after birth, and the ECG progressively shifts towards left ventricular dominance over the first years of life. A student who applies adult ECG criteria to a neonatal trace will over-diagnose pathology; a student who does not recognise when the 'normal neonatal pattern' should have resolved will miss real disease.
Provided image
A structured systematic approach to every paediatric ECG prevents errors:
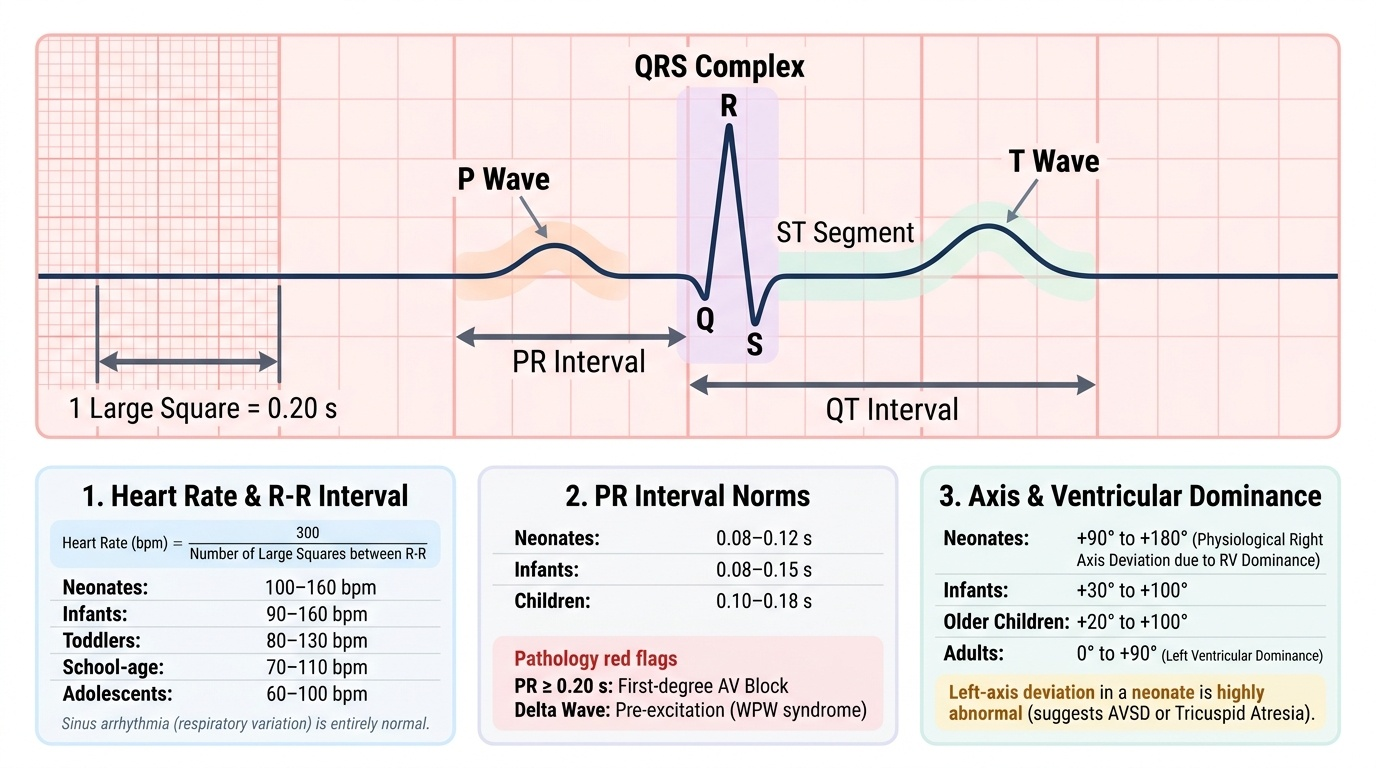
1. Rate: Count the R-R interval (between two consecutive QRS complexes) and calculate heart rate = 300 ÷ number of large squares between two R waves (at standard paper speed 25 mm/s; 1 large square = 0.2 s). Compare against age-specific norms: neonates 100–160/min, infants 90–160/min, toddlers 80–130/min, school-age 70–110/min, adolescents 60–100/min.
2. Rhythm: Is the rhythm regular? Is every P wave followed by a QRS (and is every QRS preceded by a P wave)? Identify the P-wave axis (should be upright in I and II for sinus rhythm). Sinus arrhythmia (rate varies with respiration — faster on inspiration) is normal in children; do not confuse with pathological arrhythmia.
3. Axis: Calculate the mean QRS axis from leads I and aVF. Normal axis varies by age: neonates have right-axis deviation (physiological, due to RV dominance — axis +90 to +180); this shifts progressively left: infants +30 to +100; older children +20 to +100; adults 0 to +90. Left-axis deviation in a neonate is abnormal (suggests tricuspid atresia, AVSD). Right-axis deviation persisting beyond infancy suggests right ventricular hypertrophy.
4. PR interval (normal values by age): Neonates: 0.08–0.12 s; infants: 0.08–0.15 s; children: 0.10–0.18 s. PR > 0.20 s at any age = first-degree AV block. PR shortening with a delta wave (slurred upstroke of QRS) = pre-excitation (Wolff-Parkinson-White syndrome).
5. QRS duration: Shorter in children than adults: <0.08 s in infants; <0.10 s in school-age children. Wide QRS (>0.12 s) = bundle branch block or ventricular rhythm. An rSR' pattern in V1 (partial RBBB) — an RSR' with QRS <0.12 s — is a normal variant in some children but can also indicate ASD.
6. QRS morphology in precordial leads — the key paediatric difference:
In the right precordial leads (V1, V2), the R:S ratio is normally higher in children than adults, reflecting RV dominance:
- Neonates: dominant R wave in V1 (normal — RV dominance)
- By age 3–5: transitional; R:S in V1 should be decreasing
- By school age: S wave becomes dominant in V1 (LV dominance); a tall R in V1 after age 5 suggests right ventricular hypertrophy
7. T wave changes — critical paediatric distinction:
- T wave in V1 is normally INVERTED in neonates and infants (reflects RV dominance and direction of repolarisation)
- T wave in V1 becomes upright between ages 8–10 years (after LV dominance is fully established)
- T wave upright in V1 in a neonate or infant = ABNORMAL — suggests right ventricular hypertrophy, strain, or ischaemia
- T wave inversions in V4–V6 = left ventricular strain; T wave inversions in V1–V4 after age 10 = right ventricular strain
8. QTc interval: QTc = QT (seconds) ÷ √RR (seconds) — Bazett formula. Measure QT from start of QRS to end of T wave (at the point where the T wave meets the isoelectric line). Normal QTc < 0.44 s in children (some centres use <0.45 s for females). QTc 0.44–0.46 s = borderline; QTc > 0.47 s = significant prolongation — risk of torsades de pointes and sudden cardiac death. Long QT syndrome (LQTS) is the most important cause; also seen with hypocalcaemia, hypokalaemia, and QT-prolonging drugs.
| Parameter | Neonate | Infant (1-12mo) | Child (1-8yr) | Older child/Adolescent |
|---|---|---|---|---|
| Heart rate (bpm) | 100-160 | 90-160 | 80-130 | 60-100 |
| PR interval (s) | 0.08-0.12 | 0.08-0.15 | 0.10-0.17 | 0.12-0.20 |
| QRS duration (s) | <0.08 | <0.08 | <0.09 | <0.10 |
| QTc (s) | <0.44 | <0.44 | <0.44 | <0.44 |
| QRS axis | +60 to +180 | +10 to +125 | +20 to +100 | -20 to +100 |
SELF-CHECK
On a neonatal ECG, you observe upright T waves in lead V1. What is the correct interpretation?
A. Normal finding in neonates — T waves in V1 are expected to be upright
B. Abnormal finding — T waves in V1 should be inverted in neonates and infants
C. This indicates left ventricular strain and requires urgent echocardiography
D. T wave morphology in V1 has no significance in neonates
Reveal Answer
Answer: B. Abnormal finding — T waves in V1 should be inverted in neonates and infants
In neonates and infants, T waves in V1 are normally INVERTED. This reflects the physiological right ventricular dominance and the direction of ventricular repolarisation in early life. T waves in V1 normally become upright between ages 8–10 years as left ventricular dominance is established. An upright T wave in V1 in a neonate is therefore ABNORMAL and suggests right ventricular hypertrophy, strain, or ischaemia — requiring further investigation. This is one of the most frequently tested paediatric ECG distinctions.
Recognising Abnormal Paediatric ECG Patterns
Pathological ECG patterns in children are best understood by recognising how they deviate from the age-expected normal baseline described in the previous section. The most clinically important patterns for a final-year student to recognise are ventricular hypertrophy, AV conduction defects, prolonged QT, and pre-excitation. The key principle governing the interpretation of all of these patterns is that the ECG reflects electrical events — not structural anatomy directly — and that the same electrical event can be normal at one age and pathological at another. A neonatal right-axis deviation at +150° is physiological; the same axis in a 12-year-old is right ventricular hypertrophy. A T wave inverted in V1 in a 3-month-old is normal; the same T-wave change in a 14-year-old is right ventricular strain. Every pathological pattern must therefore be evaluated against the age-appropriate baseline, not a single fixed standard. With that foundational principle established, the following patterns are the high-yield clinical findings you must be able to recognise and correctly interpret in a final-year context.
Provided image
Right Ventricular Hypertrophy (RVH):
RVH in children beyond the neonatal period is defined as persistence or exaggeration of the neonatal RV-dominant pattern in an age group where LV dominance should be established:
- Tall R wave in V1 beyond the age where it should have regressed (>5 years) — R wave >20 mm in V1 in a school-age child
- Positive T wave in V1 in a child where it should be inverted (before age 8)
- Upright R wave in aVR (normally negative after infancy)
- Right-axis deviation persisting beyond infancy
- Deep S waves in V5-V6 (lateral LV leads show S waves as the RV vector dominates)
- Seen in: pulmonary hypertension, pulmonary stenosis, right-to-left shunts (tetralogy of Fallot), Eisenmenger syndrome
Left Ventricular Hypertrophy (LVH):
- Tall R waves in V5-V6 and/or deep S waves in V1 (Sokolow-Lyon criterion adapted for children: R in V5 or V6 + S in V1 > age-specific threshold)
- T wave inversion in lateral leads (V5-V6, I, aVL) = LV strain pattern
- Left-axis deviation
- Seen in: systemic hypertension, aortic stenosis, dilated cardiomyopathy, coarctation of the aorta
Biventricular Hypertrophy:
- Combined features of both RVH and LVH
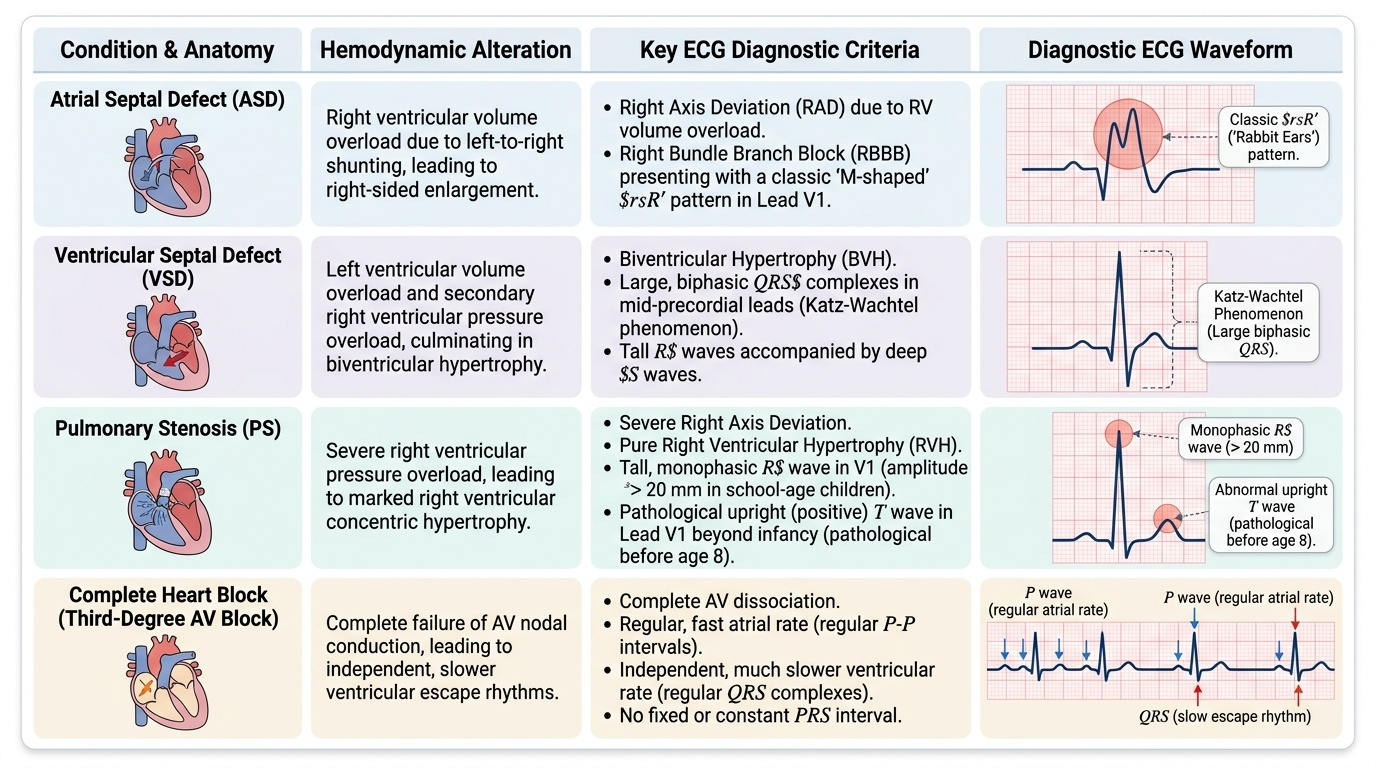
- Seen in large ventricular septal defects (VSD) — both ventricles share the volume overload
- Katz-Wachtel phenomenon: large biphasic RS complexes in the mid-precordial leads (V3-V4) — large R and large S in the same lead
AV Block:
- First-degree AV block: PR interval > 0.20 s (at any age); every P wave conducts. Can be a normal variant, vagal, or a sign of myocarditis/rheumatic carditis.
- Second-degree AV block — Mobitz type I (Wenckebach): PR interval progressively lengthens until a P wave is not followed by a QRS, then the cycle repeats. Often vagal in children.
- Second-degree AV block — Mobitz type II: PR interval is constant, but occasional P waves are not conducted — more serious, may progress to complete block.
- Complete (third-degree) AV block: no relationship between P waves and QRS complexes; P waves and QRS complexes are completely dissociated. The atrial rate and ventricular rate are different. Ventricular rate is slow (junctional or idioventricular escape rhythm). Causes in children: congenital complete heart block (associated with maternal anti-Ro/anti-La antibodies in SLE, structural heart disease), post-cardiac surgery, acquired (myocarditis, Lyme disease).
Prolonged QT (Long QT Syndrome, LQTS):
- QTc > 0.44 s; >0.47 s is significant
- Congenital LQTS (Romano-Ward autosomal dominant, Jervell and Lange-Nielsen autosomal recessive with sensorineural deafness) — mutations in cardiac potassium/sodium channels
- Presentation: syncope during exercise or emotion, sudden cardiac death in young athletes, family history of sudden death
- Acquired LQTS: hypocalcaemia (tetany + prolonged QT in neonates), hypokalaemia, drugs (macrolides, antifungals, quinolones, antipsychotics)
- Dangerous arrhythmia: torsades de pointes → ventricular fibrillation
Wolff-Parkinson-White (WPW) Syndrome:
- Short PR interval (< age-specific lower limit)
- Delta wave: slurred upstroke at the start of the QRS complex
- Wide QRS (due to pre-excitation of the ventricle via the accessory pathway)
- Patients may have paroxysmal supraventricular tachycardia (PSVT) — palpitations, syncope
Atrial Septal Defect (ASD) — typical ECG:
- Right-axis deviation + partial or complete RBBB (rSR' pattern in V1 with narrow QRS)
- Right atrial enlargement (P pulmonale)
- The RBBB in ASD is due to volume overload of the right ventricle causing delayed activation
SELF-CHECK
A 6-year-old child with Down syndrome has an ECG showing left-axis deviation and a prolonged PR interval. What diagnosis should you consider?
A. Tetralogy of Fallot — right-axis deviation and RVH are expected
B. Atrioventricular septal defect (AVSD) — left-axis deviation is the classical ECG finding
C. Wolff-Parkinson-White syndrome — short PR with delta wave is pathognomonic
D. Normal ECG for a child with Down syndrome
Reveal Answer
Answer: B. Atrioventricular septal defect (AVSD) — left-axis deviation is the classical ECG finding
Atrioventricular septal defect (AVSD — also called endocardial cushion defect) is the most common congenital heart disease in children with Down syndrome. Its classical ECG finding is left-axis deviation (or superior axis — axis between -40° and -90°), which is due to the abnormal development of the conduction system and the anatomy of the primum ASD/common AV valve. A prolonged PR interval may also be present. This contrasts with most other congenital lesions where axis is normal or rightward. Left-axis deviation in a child with Down syndrome is AVSD until proven otherwise.