Page 25 of 31
PE22.9-10 | Cardiovascular Investigations — SDL Guide (Part 3)
Applied Practice — Integrated CXR and ECG Reading
Integrating CXR and ECG findings with clinical examination creates a powerful diagnostic picture. The three investigations are complementary: clinical examination identifies symptoms and signs; CXR assesses structural size and pulmonary vascularity; ECG assesses electrical function, hypertrophy voltages, and rhythm. When all three are concordant, the diagnostic probability rises dramatically.
Provided image
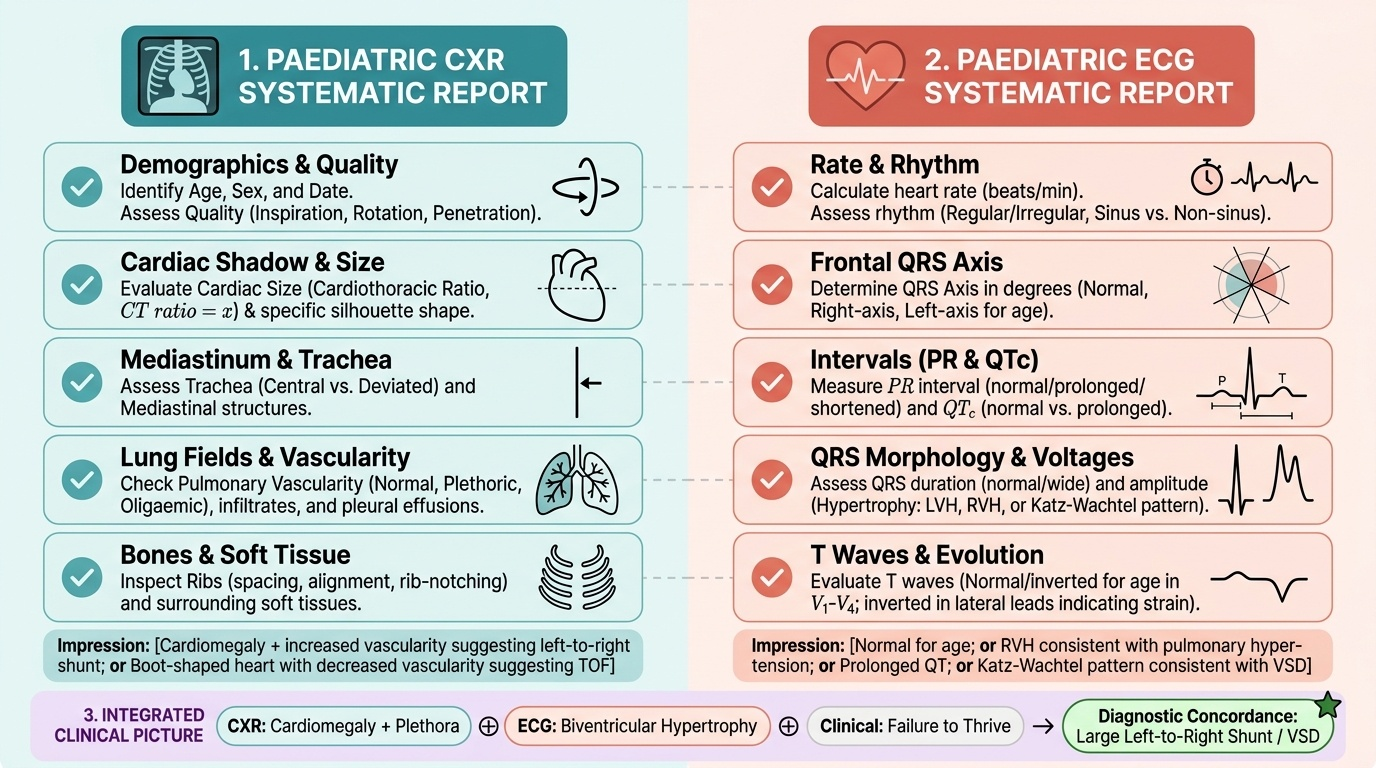
Structured reporting framework (OSCE-standard): When interpreting a paediatric CXR or ECG in an examination or clinical setting, always provide a structured report:
For a CXR: 'This is an [AP/PA] chest X-ray of a [age/sex] child, taken on [date if known]. Quality: [adequate/rotated/expiratory]. Cardiac shadow: [normal size / CT ratio = X, cardiomegaly], [normal shape / specific silhouette]. Mediastinum: trachea [central/deviated]. Lung fields: pulmonary vascularity [normal/plethoric/oligaemic], no/bilateral infiltrates/pleural effusion. Bones: ribs [normal/notching]. Impression: [cardiomegaly + increased vascularity suggesting left-to-right shunt; or boot-shaped heart with decreased vascularity suggesting tetralogy of Fallot; etc.]'
For a paediatric ECG: 'This is an ECG of a [age/sex] child. Rate: [beats/min]. Rhythm: [regular/irregular], sinus/non-sinus. Axis: [degrees — normal/right-axis/left-axis for age]. PR interval: [seconds — normal/prolonged/shortened]. QRS duration: [seconds — normal/wide]. QRS morphology: [normal/RBBB/LVH/RVH]. T waves: [normal/inverted in V1-V4, normal for age / inverted in lateral leads — strain]. QTc: [seconds — normal/prolonged]. Impression: [normal ECG for age / RVH consistent with pulmonary hypertension / prolonged QT requiring further evaluation / complete heart block with dissociation]'
Integrated Case A: An 8-month-old with recurrent chest infections and failure to thrive. CXR: CT ratio 0.65 (AP view), increased pulmonary vascularity bilaterally, enlarged hila. ECG: right-axis deviation for age (+120°), large R waves in V1 and V2 with large S in V6, biventricular hypertrophy, T waves appropriately inverted in V1.
Integration: CXR shows cardiomegaly + pulmonary plethora = large left-to-right shunt. ECG shows biventricular hypertrophy (Katz-Wachtel pattern) consistent with a large VSD. The infant is volume-loaded; both ventricles are working hard. This child needs urgent cardiology referral and echocardiography. The recurrent chest infections and failure to thrive are classic presentations of haemodynamically significant VSD.
Integrated Case B: A 14-year-old athlete collapses during a 400-metre race but regains consciousness. CXR: normal cardiac size and shape, no pulmonary abnormality. ECG: QTc = 0.52 s, inverted T waves in V4-V5, no delta wave, no block.
Integration: Normal CXR suggests no structural cardiomegaly. ECG shows significantly prolonged QTc (0.52 s >> 0.44 s threshold) with lateral T-wave inversions. This is Long QT Syndrome until proven otherwise — the exertional syncope with a prolonged QTc is a classic presentation. This requires urgent cardiology referral, genetic testing for LQTS mutations, avoidance of competitive sport, and possibly beta-blocker therapy or ICD placement. Do NOT reassure this patient and discharge.
Self-Assessment
Test your understanding with these clinical questions. Work through the reasoning before checking the answer.
Question 1: A CXR shows a CT ratio of 0.68 on a PA view in a 5-year-old. Which chambers might be enlarged? What pulmonary vascular pattern would you look for to differentiate a left-to-right shunt from dilated cardiomyopathy?
Think: CT ratio 0.68 = significant cardiomegaly. A left-to-right shunt (e.g. VSD/ASD) would show INCREASED pulmonary vascularity (plethora) — the extra blood going to the lungs makes vessels more prominent. Dilated cardiomyopathy would show NORMAL or DECREASED vascularity initially, with pulmonary oedema (bilateral haziness, Kerley B lines) developing as systolic function deteriorates. The vascularity pattern is the key discriminator.
Question 2: What ECG finding in a 3-year-old would make you MOST concerned about a prolonged QT syndrome?
Think: QTc > 0.44 s, specifically > 0.47 s, is significantly prolonged and associated with torsades de pointes risk. Also look for: T wave alternans (alternating T wave amplitude — an ominous sign), family history of sudden cardiac death at young age, or history of syncope during exercise or startle. Measure QTc in multiple leads and use the lead with the clearest T-wave endpoint.
Question 3: A child with Down syndrome has an ECG showing left-axis deviation (-60°) and right atrial enlargement. The CXR shows an increased CT ratio with pulmonary plethora. What is the most likely diagnosis?
Think: This classic combination in Down syndrome = Atrioventricular Septal Defect (AVSD). Left-axis (or superior axis) deviation is pathognomonic of AVSD due to the abnormal conduction system anatomy. Right atrial enlargement and pulmonary plethora on CXR are consistent with the large volume of blood flowing from left to right through the common AV valve and the ASD/VSD components. Echocardiography confirms. AVSD accounts for approximately 40% of cardiac defects in trisomy 21.
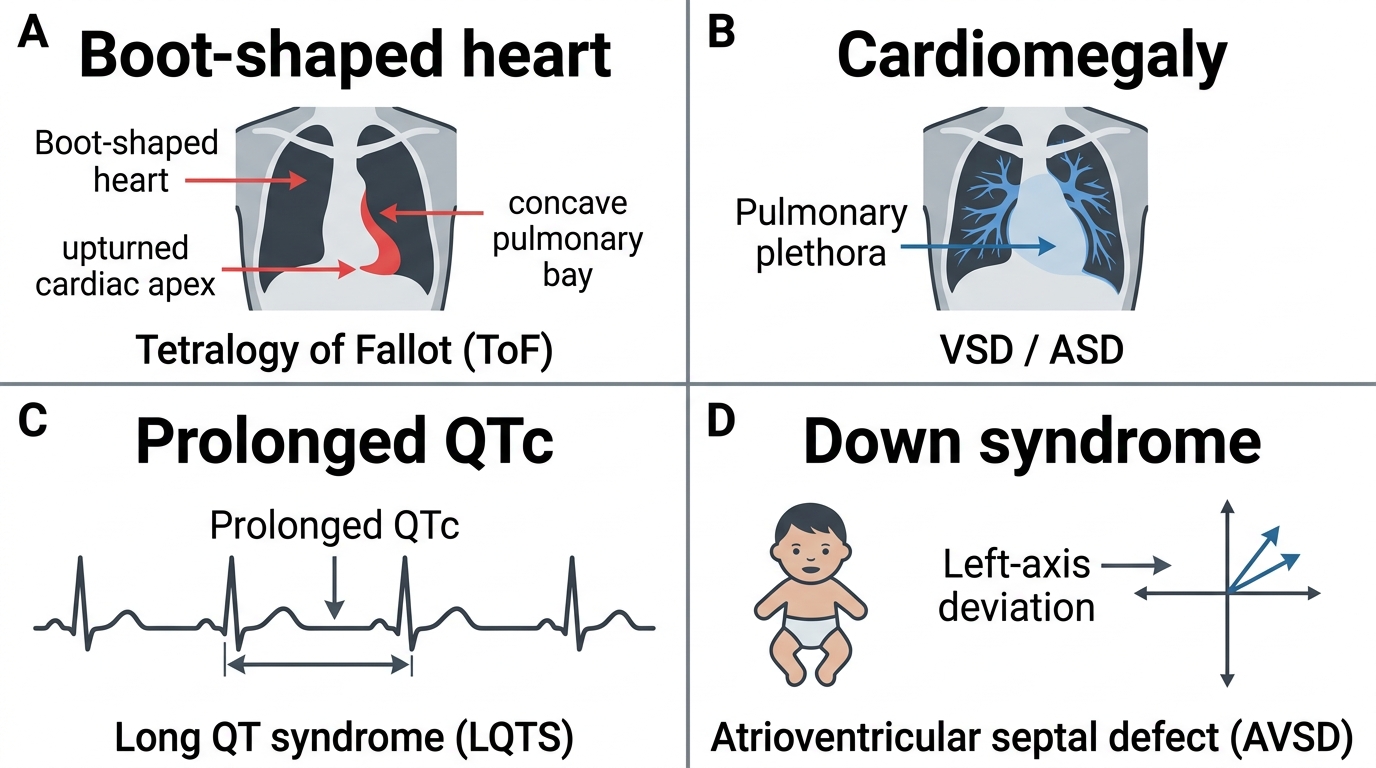
Key CXR and ECG Clues in Congenital Heart Disease