Page 7 of 42
PE23.3 | Abdominal Pain — SDL Guide
Learning Objectives
- Classify abdominal pain in children as acute versus chronic/recurrent and identify red-flag features of surgical emergencies
- Describe the pathophysiology of visceral versus somatic abdominal pain and the age-based differential diagnosis
- Conduct a structured clinical evaluation including physical examination signs specific to appendicitis
- Apply the Alvarado scoring system for risk-stratification of appendicitis
- Outline the management of acute surgical abdomen, common medical causes, and functional abdominal pain in children
INSTRUCTIONS
Abdominal pain is one of the most frequent reasons a child is brought to a doctor, and the differential diagnosis spans from the benign and self-limiting to the immediately life-threatening. The paediatric clinician's task is to rapidly and reliably distinguish the child who needs a surgeon right now from the one who needs reassurance and follow-up. This module builds the systematic clinical reasoning framework to do that — from the character of the pain to the examination findings, from the Alvarado score to the ultrasound, from appendicitis to functional abdominal pain disorder.
References
- Ghai Essential Pediatrics, 9th edition, Ch 16 (Gastrointestinal system) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 340 (Acute abdomen) and Ch 371 (Appendicitis) (textbook)
- ROME IV Diagnostic Criteria for Functional Gastrointestinal Disorders (Children, 2016) (guidelines)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 10-year-old boy comes to the paediatric emergency room at 11 PM with a 12-hour history of abdominal pain that started around the umbilicus and has now settled in the right lower abdomen. He has vomited once and refused his dinner. His temperature is 38.2°C. He flinches when you press at McBurney's point and lets out a sharp cry when you suddenly release the pressure.
Compare this with a different 10-year-old girl who has been coming to your clinic for the third time this year with central abdominal pain. It comes on at school, particularly before examinations or in the morning. There is no fever, no vomiting, she eats normally, is growing well, and her examination is unremarkable. Her mother says 'every time we take her to the hospital they do tests and find nothing.'
Both children have abdominal pain. One is 6 hours from perforation. The other needs a very different kind of medicine. Can you tell them apart — and give each what they need?
WHY THIS MATTERS
Abdominal pain accounts for up to 10% of all paediatric emergency department visits and is a leading cause of paediatric surgical admissions in India. Appendicitis, the most common surgical emergency in children beyond infancy, has a perforation rate of 30–50% in children under 5 years because the diagnosis is delayed — atypical presentations, inability to localise pain, and rare conditions like retrocaecal appendicitis frustrate clinical diagnosis. Equally important is the recognition of functional abdominal pain disorder, which affects 10–15% of school-age children, causes significant school absenteeism, and must be diagnosed positively rather than by repeated investigations. Mastering the clinical approach to abdominal pain in children is essential for every MBBS graduate entering clinical practice.
RECALL
Recall from your Anatomy course the position of the appendix — it arises from the caecum at the convergence of the three taeniae coli, approximately 2 cm below the ileocaecal valve. Its position varies: retrocaecal (most common, 65%), pelvic/paracolic, or pre/post-ileal. This variation explains why appendicitis can present with flank pain (retrocaecal) or pelvic/suprapubic pain (pelvic). Recall also from Physiology the distinction between visceral pain (diffuse, poorly localised, periumbilical, from stretch/distension/ischaemia of viscera — carried by C-fibres via sympathetic afferents) and somatic pain (well-localised, sharp, from parietal peritoneal irritation — carried by Aδ-fibres via spinal nerves). This dichotomy underlies the classic migration of appendicitis pain: visceral periumbilical → somatic right iliac fossa as inflammation reaches the parietal peritoneum.
Clinical Presentation: Character and Red Flags
The first and most important clinical task is to classify abdominal pain along two axes: duration (acute vs chronic/recurrent) and urgency (surgical emergency vs medical vs functional). These two axes drive the entire management approach, and establishing them in the first minute of the encounter is the foundation of safe clinical reasoning.
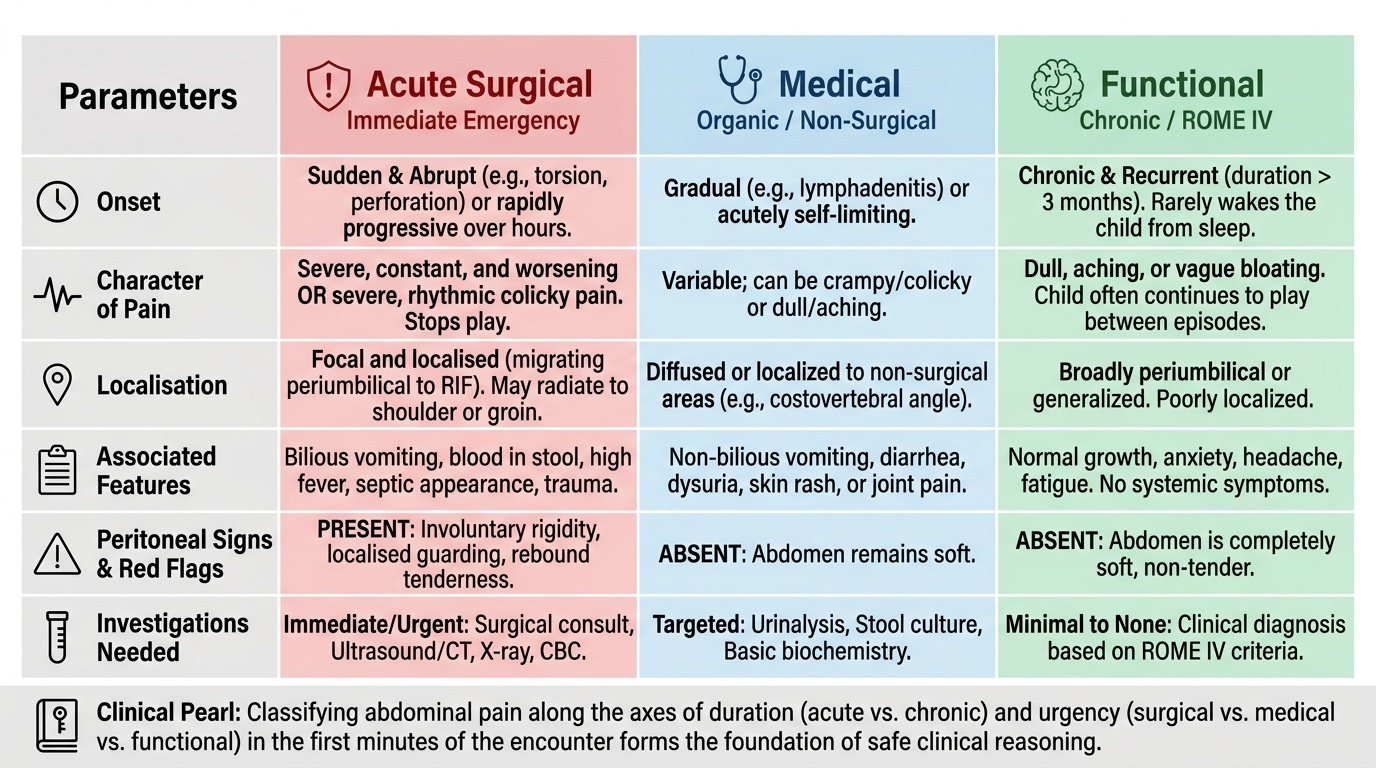
Provided image
Acute abdominal pain (onset within hours to days) demands immediate triage. The key question is: does this child have peritoneal irritation? Signs of peritoneal irritation — guarding, rigidity, rebound tenderness, and pain worsening with movement — indicate surgical disease until proven otherwise and require urgent surgical assessment. Chronic or recurrent abdominal pain is defined as at least 3 episodes of pain over at least 3 months (traditional definition) or by ROME IV criteria for functional abdominal pain disorders.
SOCRATES pain history — essential elements:
- Site: Periumbilical → RIF migration (appendicitis); central colicky (intussusception, obstruction); suprapubic (UTI, pelvic appendix); generalised (gastroenteritis, peritonitis, functional)
- Onset: Sudden (torsion, perforation, intussusception) vs gradual (appendicitis, UTI, mesenteric lymphadenitis)
- Character: Colicky/crampy (obstruction, intussusception, colic) vs constant (appendicitis progressing to peritonitis) vs dull/aching (functional, UTI)
- Radiation: Right shoulder (subphrenic irritation — rare); groin (testicular torsion, referred from ureter)
- Associated features: Fever (infection, surgical), vomiting (obstruction, surgical), dysuria (UTI), blood PR (intussusception, Meckel's, mesenteric ischaemia), jaundice (hepatitis, biliary), skin rash (Henoch-Schönlein purpura), joint pain (HSP, inflammatory bowel disease)
- Timing: Does pain wake child from sleep? (organic > functional — functional pain rarely wakes from sleep)
- Severity: Severe enough to stop play/activity; curling up in agony (surgical) vs continuing to play between episodes (functional)
Red flag features demanding urgent surgical evaluation:
- Localised tenderness with guarding or rebound
- Involuntary rigidity ('board-like abdomen')
- Pain worsening progressively over hours
- Bile-stained vomiting
- Blood in stool ('currant-jelly')
- Septic appearance (high fever, tachycardia, hypotension, pallor)
- Trauma
- Scrotal pain/swelling in adolescent males (testicular torsion — urological emergency, 6-hour window)
Pathophysiology and Aetiology
Understanding the pathophysiology of abdominal pain requires integrating the distinction between visceral and somatic nociception with the age-based pattern of disease. Visceral pain arises from distension, ischaemia, or spasm of hollow organs and is mediated by slow, unmyelinated C-fibres travelling with sympathetic nerves to the spinal cord. It is perceived as dull, crampy, and periumbilical regardless of which organ is involved — because all abdominal visceral afferents converge in the same dorsal horn segments (T8-L1). This is why the early pain of appendicitis is periumbilical. Somatic pain arises when the parietal peritoneum is inflamed (by purulent or chemical content leaking from a perforated organ) — it is sharp, well-localised, and mediated by Aδ-fibres in the spinal nerves supplying the specific dermatome. This explains the shift from periumbilical to right iliac fossa pain as appendicitis progresses.
Age-based differential diagnosis:
Infants and toddlers (under 2 years):
- Intussusception (peak 6–18 months): Telescoping of the ileum into the caecum causes paroxysmal colicky pain with intermittent well periods (the child appears pale and limp during episodes), vomiting, and eventually currant-jelly bloody stool. A sausage-shaped mass may be palpable.
- Incarcerated hernia: Inguinal hernia is common in male infants; incarceration presents with inconsolable crying, groin mass, and signs of obstruction.
- Volvulus (malrotation): Bilious vomiting + abdominal pain = surgical emergency
School-age children (5–12 years):
- Appendicitis (most common surgical cause): Classic periumbilical → RIF migration, anorexia, low-grade fever, vomiting. Children <5 years often present atypically with high fever, diffuse tenderness, and early perforation.
- Mesenteric lymphadenitis: Reactive lymph node enlargement following URTI; presents exactly like early appendicitis; diagnosed by ultrasound (enlarged mesenteric nodes, no appendix pathology); self-limiting.
- Urinary tract infection: Dysuria, frequency, suprapubic or flank pain; fever; UA shows leucocytes and nitrites.
- Constipation: A palpable fecal mass, left-sided or central pain, responds to laxatives. Often overlooked as a cause of chronic abdominal pain.
Adolescents:
- Appendicitis (peak incidence in teenage years)
- Gynaecological: Dysmenorrhoea, mittelschmerz (mid-cycle ovulation pain), ovarian cyst torsion, pelvic inflammatory disease, ectopic pregnancy (always consider in sexually active females with lower abdominal pain)
- Testicular torsion: Sudden severe lower abdominal/scrotal pain in adolescent males; cremasteric reflex absent; Doppler USG shows absent blood flow; 6-hour surgical window to save the testis
All ages — non-gastrointestinal causes:
- Lower lobe pneumonia: Diaphragmatic irritation causes referred abdominal pain; examine the chest in every child with abdominal pain
- Diabetic ketoacidosis: Abdominal pain can be the presenting feature; check glucose
- Henoch-Schönlein purpura (HSP/IgA vasculitis): Palpable purpura (lower limbs, buttocks) + abdominal pain + arthritis + haematuria; abdominal pain can precede the rash
- Sickle cell disease: Vaso-occlusive pain crises
- Functional abdominal pain disorder (FAPD, ROME IV): Episodic or continuous abdominal pain, ≥4 episodes per month for ≥2 months, not explained by another condition; must also have negative organic workup or, if positive, pain is not attributable to the finding
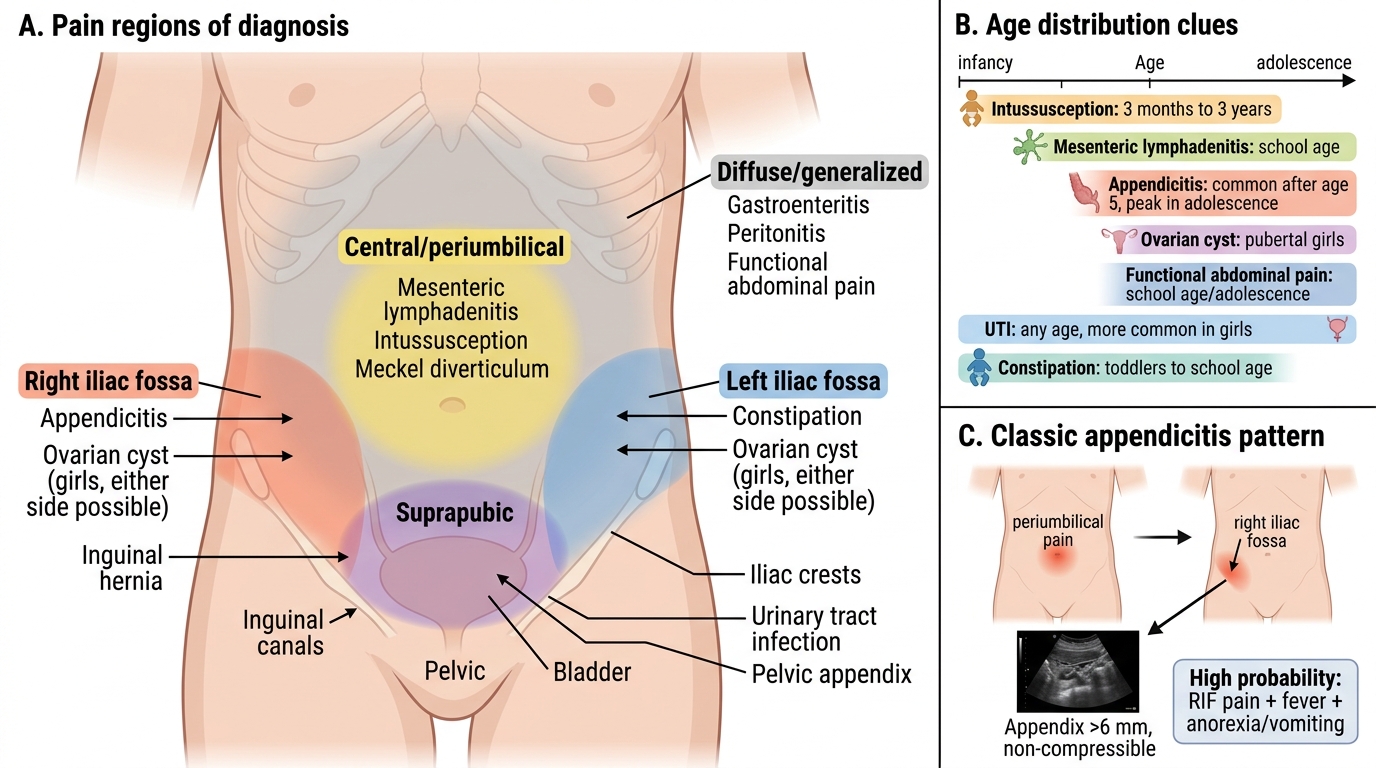
Common Causes of Abdominal Pain by Region in Children
SELF-CHECK
A 9-year-old boy presents with 18-hour history of periumbilical pain that has shifted to the right iliac fossa. He has vomited twice, is anorexic, and has a temperature of 38.5°C. His Alvarado score is 8/10. Ultrasound shows a non-compressible appendix with wall thickness 8 mm. What is the MOST appropriate next step?
A. Discharge with analgesia and review in 24 hours
B. Observe for 6 hours, repeat ultrasound, then decide
C. Refer urgently to paediatric surgery for appendicectomy
D. Treat empirically with oral amoxicillin-clavulanate for suspected mesenteric lymphadenitis
Reveal Answer
Answer: C. Refer urgently to paediatric surgery for appendicectomy
This child has acute appendicitis confirmed both clinically (Alvarado score 8/10 = high probability; score ≥7 = high probability) and on ultrasound (non-compressible appendix with wall thickness >6 mm is diagnostic). Urgent referral to paediatric surgery for appendicectomy is the appropriate management. Observation and repeat imaging (B) is appropriate only when the score is intermediate (5-6) and ultrasound is inconclusive. Oral antibiotics for presumed mesenteric lymphadenitis (D) is dangerous when the ultrasound already shows appendiceal pathology. Delay to perforation in a 9-year-old from confirmed appendicitis risks perforation within hours.
Evaluation and Investigations
The clinical evaluation of abdominal pain in a child is systematic and begins at the end of the bed — observing the child's posture (guarding, knees drawn up), willingness to move, and facial expression. A child who lies rigidly still, wincing with the ambulance trolley's every bump, has peritoneal signs. A child who is intermittently playful between crampy episodes is more likely to have an obstructive or functional cause. This gestalt impression, before any formal examination, is clinically useful and should never be skipped — a child who runs into the examination room and jumps onto the couch is very unlikely to have peritonitis. Conversely, a child who refuses to move, holds their breath on the journey, and flinches at the slightest touch of the examination couch warrants immediate surgical review before any investigation. The structured examination that follows should confirm or refute the initial bedside impression.
Physical examination sequence:
1. General: Temperature, pulse, blood pressure, respiratory rate; look for pallor, jaundice, purpura
2. Auscultation before palpation: Absent bowel sounds (peritonitis, paralytic ileus); high-pitched tinkling sounds (obstruction)
3. Abdominal palpation (start away from the painful site, ask the child to point to the worst spot):
- Guarding: Voluntary (patient tenses when approached) vs involuntary (board-like, persists with distraction — the latter is pathological)
- Rebound tenderness (Blumberg's sign): Pain on sudden release of deep pressure — indicates peritoneal irritation. In children, it is often elicited more gently by percussing the abdomen (equivalent tenderness on light percussion)
- McBurney's point: Maximum tenderness at a point one-third of the way from the right anterior superior iliac spine (ASIS) to the umbilicus — the surface marking of the appendix
- Rovsing's sign: Pressure in the left iliac fossa causes pain in the right iliac fossa — positive in appendicitis (referred peritoneal stretch)
- Psoas sign: Pain on passive extension of the right hip (stretches psoas over a retrocaecal appendix)
- Obturator sign: Pain on internal rotation of the flexed right hip (pelvic appendix)
4. Rectal examination: Tenderness on the right pelvic wall (pelvic appendicitis); loaded rectum (constipation); blood on glove (intussusception, Meckel's)
5. Scrotal examination in adolescent males (testicular torsion — absent cremasteric reflex)
6. Chest examination: Lower-lobe pneumonia (referred diaphragmatic pain)
Alvarado (MANTRELS) scoring for appendicitis:
| Feature | Score |
|---|---|
| Migration of pain to right iliac fossa | 2 |
| Anorexia | 1 |
| Nausea/Vomiting | 1 |
| Tenderness in right iliac fossa | 2 |
| Rebound tenderness | 1 |
| Elevated temperature (>37.3°C) | 1 |
| Leucocytosis (>10,000/mm³) | 2 |
| Total | 10 |
Score ≥7 = high probability appendicitis → surgical referral; 5–6 = equivocal → ultrasound + observe; <4 = low probability.
Investigations:
- Complete blood count: Leucocytosis with left shift (appendicitis, peritonitis, severe infection)
- C-reactive protein (CRP): Elevated in appendicitis (>10 mg/L); combined with WBC improves sensitivity
- Urinalysis: Leucocytes + nitrites + bacteria = UTI; trace leucocytes can occur with adjacent appendiceal inflammation
- Ultrasound abdomen: First-line imaging — appendix >6 mm, non-compressible, no compressibility (appendicitis); target sign (intussusception); enlarged mesenteric lymph nodes (lymphadenitis); free fluid (peritonitis). Limitation: operator-dependent, visualisation of appendix poor in obese children
- Plain X-ray abdomen: Faecolith in RIF (5% of appendicitis, specific); free air under diaphragm (perforation); fecal loading (constipation)
- CT abdomen: Not routine — reserve for equivocal cases where USG is inconclusive and clinical suspicion remains high; radiation concern in children
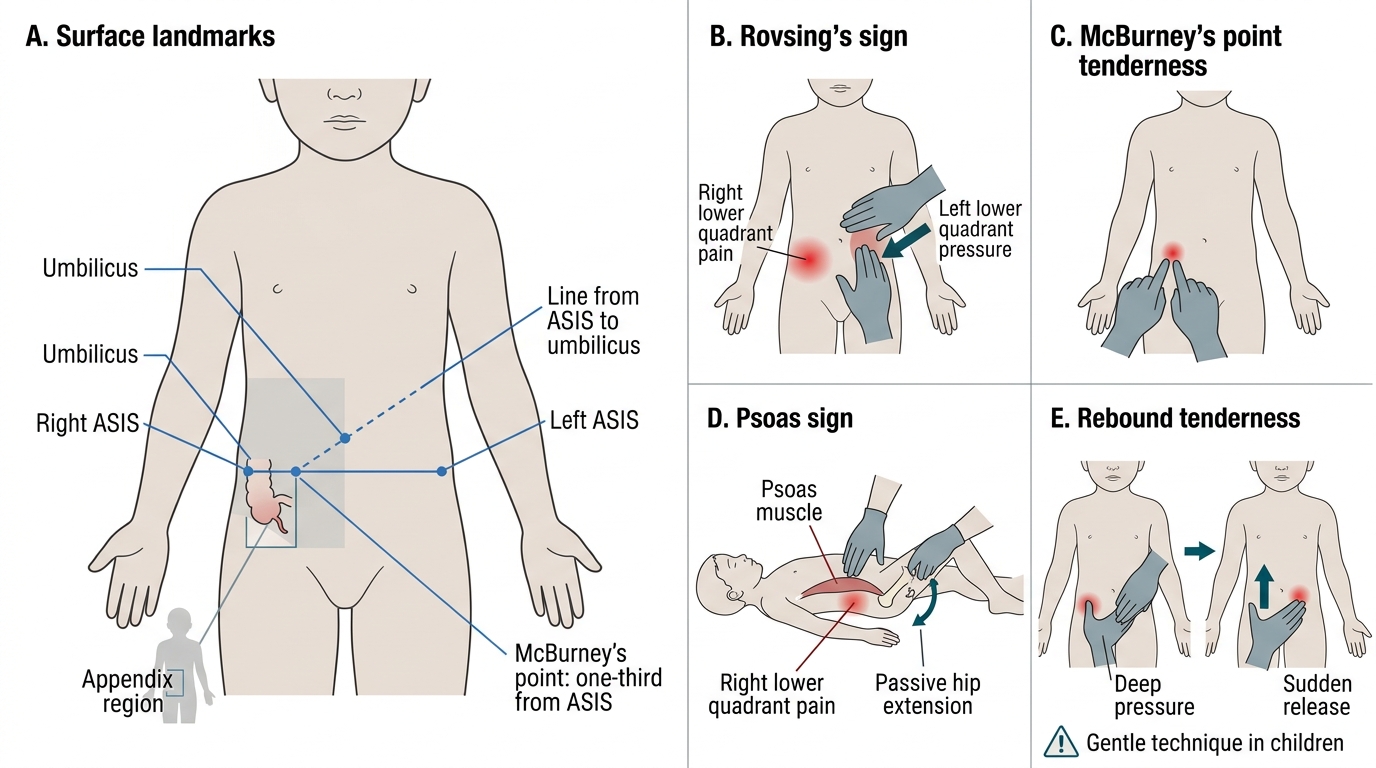
Clinical Signs in Pediatric Appendicitis
CLINICAL PEARL
The Alvarado score is a clinical tool, not a decision-maker. A score of 8 or 9 warrants immediate surgical referral; a score of 2 allows safe discharge with instructions. But a score of 5–6 is the hardest category — these children should be admitted for active observation, serial abdominal examinations every 4 hours, and ultrasound. The appendix can perforate within 24–48 hours of symptom onset in children. Equally important: always look at the scrotum in adolescent males with lower abdominal pain. Testicular torsion presents with lower abdominal rather than scrotal pain in up to 40% of cases, and the cremasteric reflex may be lost before other scrotal changes appear. The 6-hour window for orchidopexy to save the testis is absolute — a missed diagnosis means an unnecessary orchidectomy.