Page 8 of 42
PE23.3 | Abdominal Pain — SDL Guide (Part 2)
Management by Cause
Management must follow the diagnosis, and the sequence of clinical reasoning must always flow from 'most dangerous cause excluded first' to 'most common cause treated.' The child who arrives obtunded, rigid, and febrile has peritonitis until proven otherwise — management of such a child begins with resuscitation (IV access, IV fluids, analgesia, nil orally, blood cultures, urgent surgical referral), not investigations. It is a critical error to delay resuscitation while waiting for investigation results when the clinical examination already indicates a surgical emergency. Once the emergency is either confirmed or excluded, the management pathways below apply to each specific cause. Across all causes, adequate analgesia must be provided promptly — withholding pain relief 'to keep the picture clear' is both unethical and unsupported by evidence; appropriate analgesia does not mask peritoneal signs.
Acute appendicitis:
- Appendicectomy (laparoscopic or open) is the definitive treatment. Early laparoscopic appendicectomy is now standard in most centres.
- Pre-operatively: IV access, nil orally, IV antibiotics (cefuroxime + metronidazole, or co-amoxiclav), IV fluid resuscitation if signs of sepsis, analgesia (IV morphine/paracetamol — pain relief does NOT mask clinical signs and should NOT be withheld).
- Complicated appendicitis (perforation, peritonitis, abscess): IV antibiotics for 3-5 days, washout if generalised peritonitis; laparoscopic surgery in most centres.
- Uncomplicated appendicitis in selected cases: Non-operative management with IV antibiotics has been studied in adults and selected paediatric cases, but surgical treatment remains standard.
Intussusception:
- Pneumatic (air) or hydrostatic (saline/water) enema reduction under radiological guidance — first-line, success rate 75–90% if no peritonitis or systemic toxicity.
- Contraindications to enema reduction: Perforation (free air on X-ray), peritonitis, haemodynamic instability.
- If enema fails or contraindicated: Open or laparoscopic surgical reduction. Resection if gangrenous bowel.
- Recurrence after enema reduction: 5–10%; manageable with repeat enema in most cases.
Mesenteric lymphadenitis:
- Conservative management: Analgesia, IV/oral fluids, observation. Resolves spontaneously over 1–3 weeks.
- Antibiotics if bacterial cause identified (e.g. Yersinia enterocolitica — rare); otherwise supportive.
Urinary tract infection:
- Oral antibiotics for uncomplicated lower UTI: Co-trimoxazole or nitrofurantoin for 5–7 days based on local sensitivity patterns.
- IV antibiotics for pyelonephritis or systemic features: Ceftriaxone or cefotaxime until culture sensitivities available.
- Refer all children <5 years with first UTI, all children with recurrent UTI, or any child with febrile UTI for imaging (renal USG + DMSA scan if indicated) to exclude vesicoureteric reflux or renal scarring.
Functional abdominal pain disorder (FAPD):
- Diagnose positively after reasonable exclusion of organic causes — do not pursue exhaustive investigations as this reinforces the 'sick role'.
- Biopsychosocial approach: Explain the brain-gut axis (visceral hypersensitivity, how stress amplifies pain signals); validate the child's pain; avoid secondary gain from school avoidance.
- Reassure parents firmly: 'We have not missed anything dangerous; this is a real pain that the brain and gut create together.'
- Practical interventions: Regular meal times, adequate sleep, reduction of stressors; peppermint oil capsules (evidence base for IBS-type FAPD); cognitive behavioural therapy (CBT) for anxiety-driven FAPD; amitriptyline or cyproheptadine in refractory cases (off-label, specialist supervision).
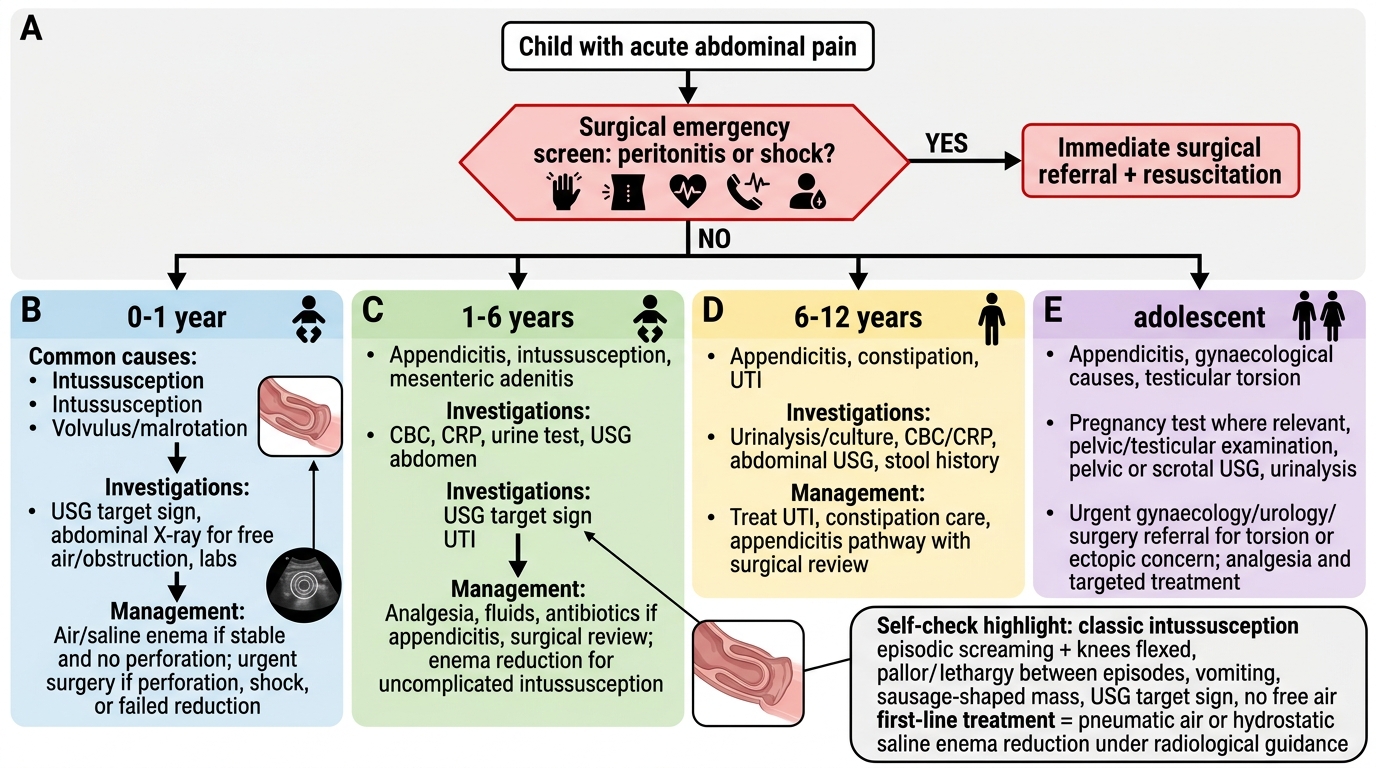
Acute Abdominal Pain in Children: Age-Based Management Algorithm
SELF-CHECK
A 14-month-old boy is brought with episodic screaming and flexing his knees up. Episodes last 3-4 minutes and recur every 15 minutes. Between episodes he is pale and lethargic. There is one episode of vomiting. On examination a sausage-shaped mass is palpable to the right of the umbilicus. Ultrasound confirms the diagnosis. There is no free air on plain X-ray. What is the FIRST-LINE treatment?
A. Emergency laparotomy and surgical reduction
B. Pneumatic (air) or hydrostatic enema reduction under radiological guidance
C. IV antibiotics and bowel rest for 24 hours before surgical evaluation
D. High-dose IV methylprednisolone to reduce bowel oedema
Reveal Answer
Answer: B. Pneumatic (air) or hydrostatic enema reduction under radiological guidance
This is classic intussusception (paroxysmal colicky pain, pallor, lethargy between episodes, vomiting, sausage-shaped mass). Confirmed on USG (target sign). No evidence of perforation (no free air on X-ray). First-line treatment is pneumatic (air) or hydrostatic (saline) enema reduction under fluoroscopic or ultrasound guidance, with a success rate of 75-90% when performed without evidence of peritonitis or perforation. Surgery is reserved for: failed enema (2 attempts), perforation, peritonitis, or haemodynamic instability. There is no role for IV steroids or conservative management with antibiotics for intussusception.
Self-Assessment: Scenarios and Differentials
Apply the clinical framework to the following three scenarios, working through the diagnosis and management before reading the discussion.
Scenario 1 — The Surgical Emergency:
An 8-year-old girl presents with 36 hours of progressively worsening abdominal pain, now generalised. Temperature 39.1°C, heart rate 128/min, appears toxic. She lies very still, crying. Abdomen is rigid and diffusely tender. Bowel sounds absent. WBC 19,000/mm³, CRP 180 mg/L.
Discussion: Generalised peritonitis, most likely from perforated appendicitis. The rigidity (involuntary guarding), absent bowel sounds, high fever, and systemic toxicity are clinical markers of generalised peritonitis. Management is resuscitation first (IV fluid bolus 20 mL/kg, IV analgesia, IV antibiotics — cefuroxime + metronidazole), then emergency surgical consultation. CT abdomen will confirm perforation and may demonstrate the ruptured appendix and free intra-abdominal fluid/air. Appendicectomy with peritoneal washout is required.
Scenario 2 — The Mimicker:
A 7-year-old boy presents with 24-hour history of right lower abdominal pain, mild fever (37.8°C), and anorexia. Alvarado score = 5. Ultrasound: normal appendix visualised (5 mm diameter, compressible), but multiple enlarged mesenteric lymph nodes (up to 15 mm) in the right iliac fossa. No free fluid.
Discussion: Mesenteric lymphadenitis — reactive enlargement of mesenteric lymph nodes, typically following URTI, presenting with clinical features almost identical to early appendicitis. The key is the ultrasound — visualised normal appendix with enlarged mesenteric nodes. Management is conservative (analgesia, oral fluids, safety-net advice to return if pain worsens or fever rises). Parents must understand it can take 2–3 weeks to fully resolve.
Scenario 3 — The Recurrent Pain:
An 11-year-old girl has had 6 episodes of central abdominal pain over the past 4 months, each lasting 2-3 hours. She misses school frequently. She had a normal physical examination, normal blood count, CRP, ultrasound, and urinalysis on three previous occasions. The pain reliably occurs on school days and never wakes her at night.
Discussion: Classic functional abdominal pain disorder (FAPD). Key positive diagnostic features: episodic, stress-linked, no nocturnal pain, normal growth, normal repeated investigations, school avoidance. Management is psychosocial — explain the brain-gut connection, involve school counsellor, explore examination anxiety or peer issues, ensure regular meals and sleep, consider CBT if available. Avoid further investigations unless a new red flag emerges.
SELF-CHECK
In the evaluation of abdominal pain in children, which finding most reliably distinguishes ORGANIC from FUNCTIONAL pain?
A. Pain severe enough to cause crying
B. Abdominal pain associated with nausea
C. Pain that consistently wakes the child from sleep at night
D. Pain that resolves completely between episodes
Reveal Answer
Answer: C. Pain that consistently wakes the child from sleep at night
Pain that consistently wakes a child from sleep is a strong red flag for an organic cause. Functional abdominal pain characteristically does not wake children from sleep — the central sensitisation and psychosocial factors that drive it are absent during sleep. This is one of the most clinically useful discriminating features. Pain severity (A) is unreliable — functional pain can be severe. Nausea (B) accompanies both organic and functional abdominal pain. Pain-free intervals between episodes (D) are characteristic of BOTH functional pain and paroxysmal surgical conditions like intussusception — they do not discriminate.