Page 4 of 42
PE23.2 | Constipation — SDL Guide
Learning Objectives
- Define constipation in children using ROME IV criteria and distinguish functional from organic causes
- Describe the pathophysiology of functional constipation and the stool-withholding cycle
- Recognise red-flag features that suggest organic causes, especially Hirschsprung's disease
- Outline a structured approach to evaluation including targeted investigations
- Apply the step-wise management of functional constipation: education, disimpaction, and maintenance therapy
INSTRUCTIONS
Constipation is among the most common gastrointestinal complaints in children, affecting up to 30% of paediatric outpatients at some point. The vast majority have functional constipation — no organic cause is found. Yet every paediatric clinician must know the red flags that point to Hirschsprung's disease, the most important organic cause, because missing it in a neonate can be fatal. This module builds the clinical framework to tell the common apart from the dangerous — and to manage both effectively.
References
- Ghai Essential Pediatrics, 9th edition, Ch 16 (Gastrointestinal system) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 367 (Motility disorders) (textbook)
- ESPGHAN/NASPGHAN Guidelines on Evaluation and Treatment of Functional Constipation in Infants and Children (2014) (guidelines)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A mother brings her 3-year-old son to your clinic. He has been having bowel movements only once every 5–7 days for the past 3 months. Each episode is associated with crying, straining, and passage of large, hard stools. She has noticed him standing on his tiptoes, crossing his legs, and pressing his perineum against furniture — she initially thought he was 'trying to go', but now suspects he is actually 'holding it in'. He has no fever, is eating well, and is growing normally. His abdomen is mildly distended, and a rectal examination reveals a large fecal mass with an explosive release of stool on finger withdrawal.
Compare this with a second child: a 6-day-old neonate who passed meconium on day 3, has had progressive abdominal distension since birth, and is now vomiting bile-stained material. A rectal examination leads to a large explosive release of stool and flatus.
Both children have 'constipation.' Which one needs an urgent biopsy and which one needs a laxative?
WHY THIS MATTERS
Constipation accounts for up to 25–30% of paediatric gastroenterology referrals and is a common cause of recurrent abdominal pain, soiling (encopresis), and school absenteeism. Functional constipation is underdiagnosed and undertreated, leading to years of unnecessary suffering and parental anxiety. On the other side, a missed Hirschsprung's disease in a neonate presents as enterocolitis — a toxic megacolon that can perforate and kill within hours. The ability to differentiate functional from organic constipation, to manage functional constipation with a stepwise approach, and to recognise the neonatal emergency is therefore a core paediatric competency.
RECALL
Recall from Year-1 Physiology that defecation is a coordinated reflex involving the enteric nervous system — the intrinsic nerve plexuses of the gut wall (Auerbach's myenteric plexus and Meissner's submucosal plexus). When faecal material distends the rectum, the rectoanal inhibitory reflex (RAIR) relaxes the internal anal sphincter (smooth muscle, autonomic/involuntary) while the external anal sphincter (striated muscle, pudendal nerve, voluntary) is consciously contracted to defer defecation. This voluntary control develops around age 2–3 years — before this, defecation is largely reflex. Recall also the anatomy of the hindgut: the sigmoid colon, rectum, and anal canal; the role of the myenteric plexus in coordinating colonic peristalsis; and the significance of ganglionic cells in normal propulsive motility.
Clinical Presentation: Defining and Recognising Constipation
Constipation is defined clinically as infrequent, difficult, or painful defecation. In paediatric practice the most widely used diagnostic framework is the ROME IV criteria for functional constipation, which recognise that the frequency and character of stool vary considerably by age. For children under 4 years, the ROME IV criteria require at least two of the following for at least one month: two or fewer defecations per week; history of excessive stool retention (withholding behaviour); history of painful or hard bowel movements; history of large-diameter stools; presence of a large fecal mass in the rectum. For children aged 4 years and older, at least one episode of fecal incontinence per week (overflow soiling/encopresis) is also included. These criteria apply only after excluding organic causes.
Provided image
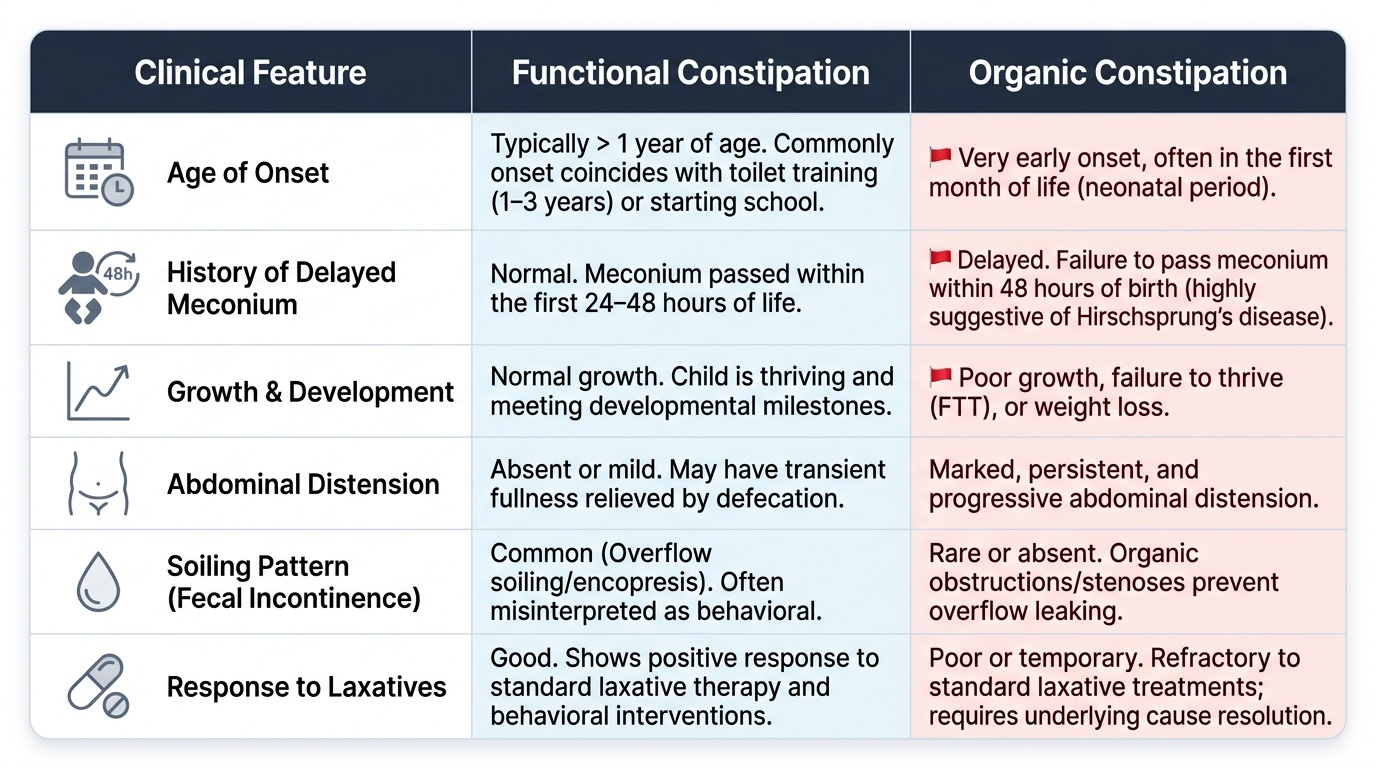
Age-specific presentation:
- Neonates: Normal term neonates pass meconium within the first 24–48 hours of life. Failure to pass meconium beyond 48 hours is a red flag for Hirschsprung's disease or anorectal malformation.
- Infants (<1 year): Straining and grunting during stool passage is common and does not necessarily represent constipation ('infant dyschezia' — a functional condition that resolves spontaneously). True constipation in infancy warrants organic workup.
- Toddlers (1–3 years): The most common age of onset for functional constipation, coinciding with toilet training. Withholding behaviour is characteristic — the child consciously contracts the external anal sphincter to avoid the pain of defecation, worsening the cycle.
- School-age children: Soiling (fecal incontinence/encopresis) due to overflow around a fecal impaction causes significant psychosocial distress and is often misinterpreted by parents as laziness or behavioural disorder.
Red flag features that suggest organic constipation:
- Onset in the first month of life
- Delayed meconium passage >48 hours (Hirschsprung's disease)
- Ribbon-like or 'pencil-thin' stools (anorectal stenosis, Hirschsprung's)
- Absence of soiling (organic obstruction does not overflow; functional constipation almost always has some soiling)
- Poor growth / failure to thrive
- Bloody diarrhoea alternating with constipation (Hirschsprung's enterocolitis)
- Neurological signs (sacral agenesis, spinal cord tethering)
- Abdominal distension disproportionate to age
- Empty rectum on examination despite obvious obstruction (Hirschsprung's — aganglionic rectum is empty, distension is proximal)
Pathophysiology and Aetiology
Functional constipation arises from a self-perpetuating cycle that begins with a single painful or frightening defecation experience — a hard stool, an anal fissure, or forced toilet training. Once defecation becomes associated with pain, the child voluntarily contracts the external anal sphincter and pelvic floor muscles to prevent stool passage. This withholding behaviour allows stool to accumulate and harden in the rectum. Harder stools cause more pain at the next attempt, reinforcing the avoidance. Over weeks to months, the rectum becomes chronically distended and the sensory threshold for the defecation urge rises — the child no longer feels the normal urge to defecate even when the rectum is full (rectal hyposensitivity). Watery stool from above leaks around the impacted mass, appearing as soiling — this is overflow fecal incontinence/encopresis, not a bowel control problem in the usual sense.
Pathophysiology of Hirschsprung's disease:
Hirschsprung's disease (congenital aganglionic megacolon) results from failure of neural crest cell migration into the hindgut wall during weeks 5–12 of gestation. The consequence is an aganglionic segment — a length of bowel (most commonly the rectosigmoid) that lacks ganglion cells in both the myenteric (Auerbach's) plexus and the submucosal (Meissner's) plexus. Without ganglion cells, this segment remains in a state of tonic contraction (spasm) and cannot generate coordinated peristaltic waves. Stool cannot pass through the aganglionic segment. The bowel proximal to the obstruction becomes progressively distended (megacolon). The segment from the internal sphincter up to the transition zone is narrow; proximal bowel is dilated. Critically, the rectoanal inhibitory reflex (RAIR) is absent in Hirschsprung's disease — this can be demonstrated on anorectal manometry. Length of aganglionosis varies: short-segment (80%, rectosigmoid), long-segment (15%), and total colonic (5%).
Organic causes of constipation — by system:
- Structural: Hirschsprung's disease; anorectal malformations (imperforated anus, anal stenosis); pelvic mass
- Metabolic/endocrine: Hypothyroidism (most common endocrine cause — constipation + slow relaxation reflexes); hypercalcaemia (renal, malignancy, hyperparathyroidism); hypokalaemia; diabetes insipidus (dehydration)
- Neurological: Spinal cord tethering/sacral agenesis (absent or asymmetric perineal reflexes); cerebral palsy (globally reduced gut motility); Chagas disease (acquired aganglionosis)
- Medication-induced: Opioids; anticholinergic drugs; antacids containing calcium or aluminium; iron supplementation
- Dietary: Insufficient fibre; excess cow's milk protein (especially in toddlers >500 mL/day)
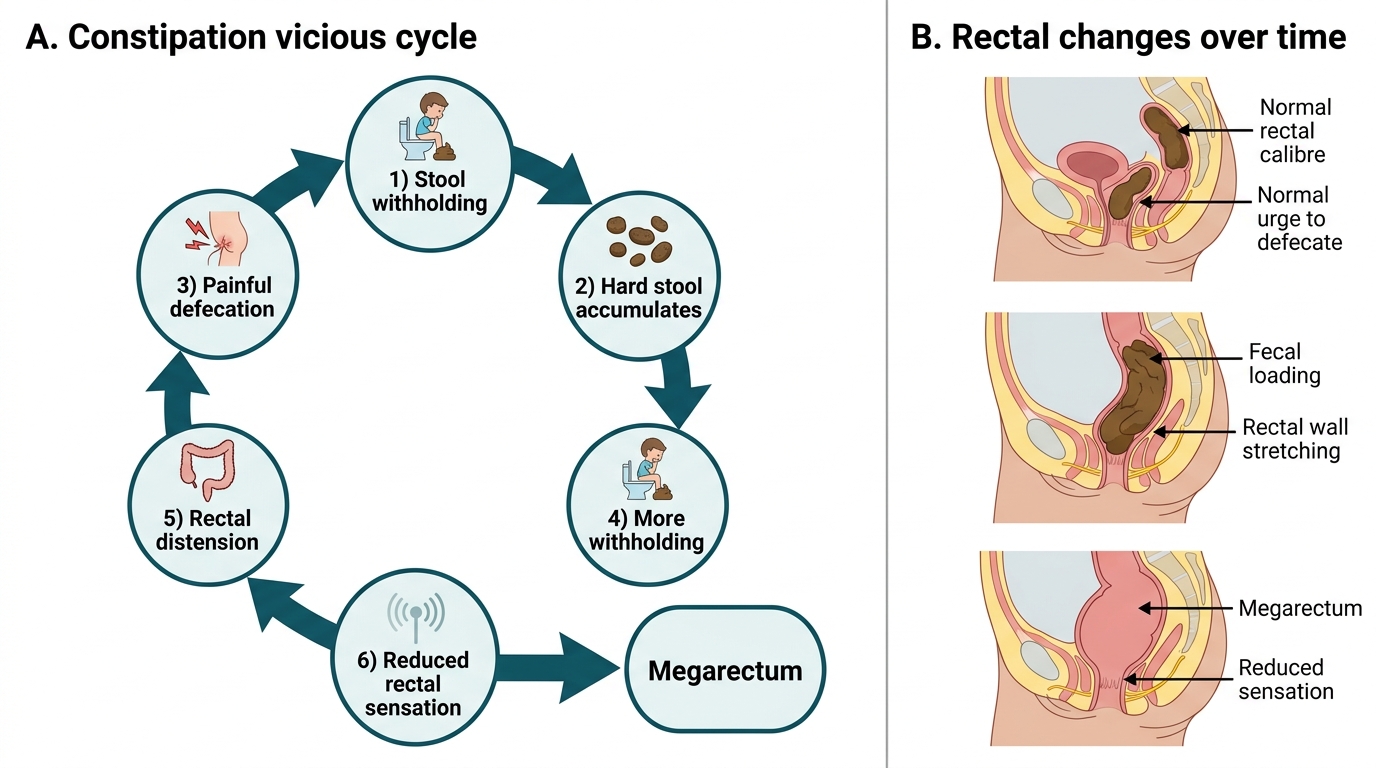
Constipation Vicious Cycle and Megarectum
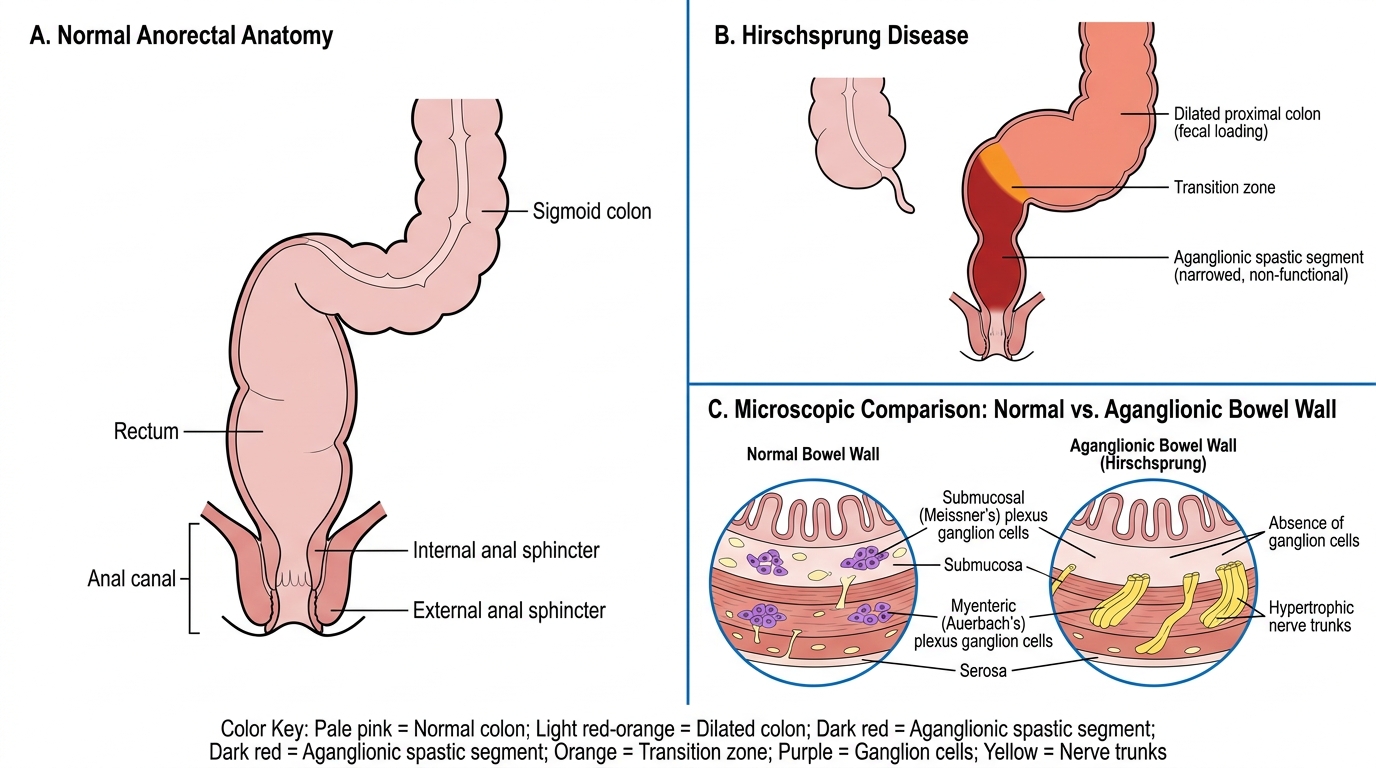
Normal Anorectal Anatomy vs Hirschsprung Disease
SELF-CHECK
A 5-day-old neonate presents with progressive abdominal distension and failure to pass stool since birth. Meconium was first passed on day 3. Rectal examination elicits a large explosive release of stool and gas. Rectal biopsy is performed. Which histological finding is DIAGNOSTIC?
A. Normal number of ganglion cells in the myenteric plexus
B. Absence of ganglion cells in the myenteric and submucosal plexuses
C. Hypertrophy of smooth muscle with intact ganglion cells
D. Neutrophilic infiltration of the submucosa
Reveal Answer
Answer: B. Absence of ganglion cells in the myenteric and submucosal plexuses
The gold standard for diagnosing Hirschsprung's disease is rectal biopsy demonstrating absence of ganglion cells (aganglionosis) in both the myenteric (Auerbach's) plexus and the submucosal (Meissner's) plexus. The aganglionic segment is always present from the internal sphincter extending proximally to a variable length. The key feature at biopsy is also often the presence of large, hypertrophied nerve trunks (hypertrophic nerve fibres) in the absence of ganglion cells. The explosive release of stool on rectal examination — 'squirt sign' — results from the pressure in the dilated proximal bowel being released past the obstructing aganglionic segment when the examiner's finger disturbs it.
Diagnosis and Investigations
The diagnosis of functional constipation is clinical — based on ROME IV criteria, age, history, and examination. The history must specifically enquire about age of onset (especially neonatal), passage of meconium, bowel habit in infancy, dietary changes, toilet-training history, withholding behaviour, soiling, and any associated symptoms (blood per rectum, weight loss, neurological symptoms). Family history of Hirschsprung's disease is relevant (especially for long-segment disease, which has a stronger familial pattern).
Provided image
Physical examination is crucial. Abdominal examination may reveal a distended, tympanic abdomen with a palpable fecal mass in the left iliac fossa or across the lower abdomen. Rectal examination should be performed in every child with suspected constipation. In functional constipation the rectum is full of stool (a loaded, distended rectum). In Hirschsprung's disease the rectum is classically empty on examination (the aganglionic segment is contracted and empty; all the stool is backed up proximally). The anal tone and perianal sensation should be assessed — reduced tone or absent anal wink reflex suggests a neurological cause.
Investigations — targeted, not routine:
Investigations are generally NOT required for straightforward functional constipation. They are indicated when:
- Red-flag features suggest organic cause
- Failure to respond to adequate medical management (3–6 months)
- Concern about Hirschsprung's disease
| Investigation | Indication | Key finding |
|---|---|---|
| Plain X-ray abdomen | Assess fecal loading; not required for diagnosis | Faecal shadow in rectum/colon; 'cut-off' sign |
| Thyroid function tests (TSH, T4) | Exclude hypothyroidism | Elevated TSH |
| Serum calcium | Exclude hypercalcaemia | Elevated ionised calcium |
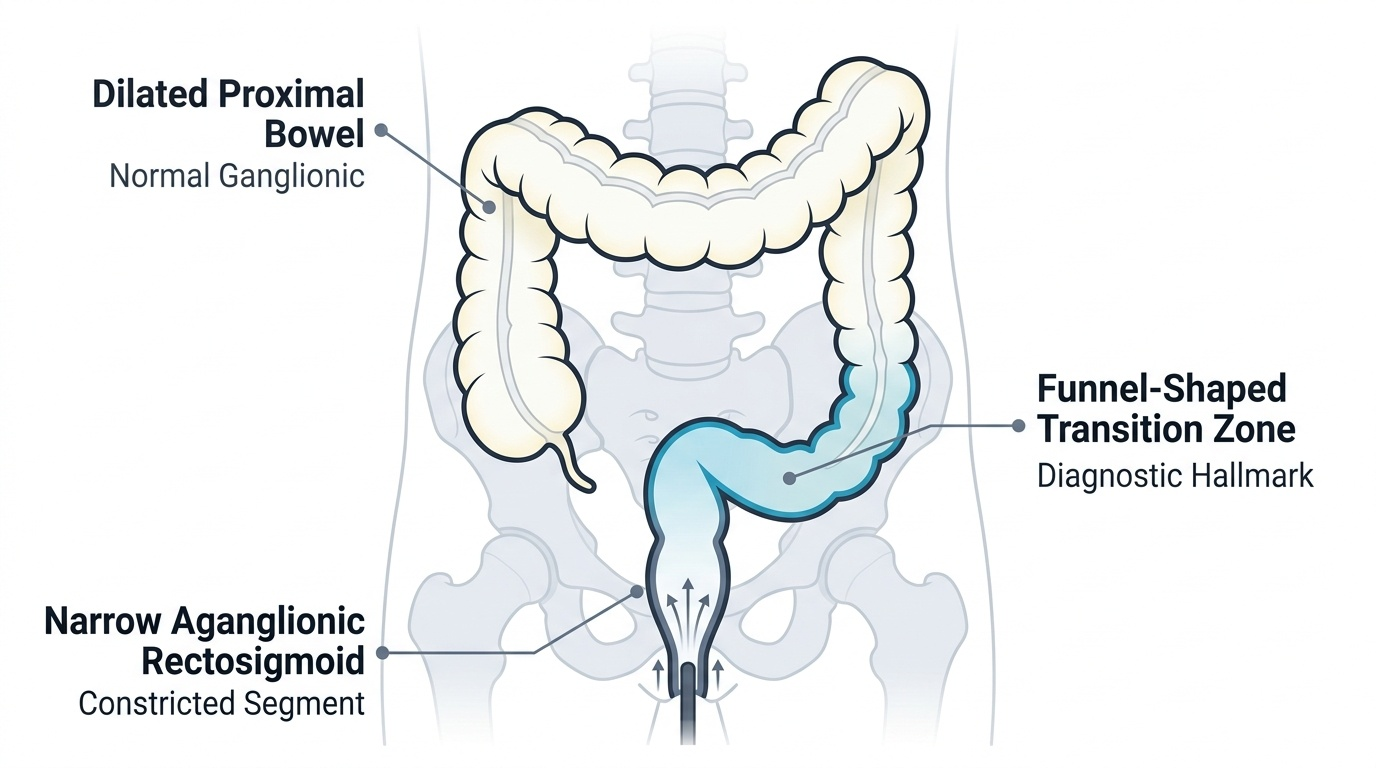
| Barium enema / contrast enema | Suspected Hirschsprung's | Transition zone: narrow aganglionic segment → dilated proximal colon; 24-hour retention of contrast |
| Rectal biopsy (suction) | Gold standard for Hirschsprung's | Absence of ganglion cells in myenteric + submucosal plexuses; hypertrophied nerve trunks |
| Anorectal manometry | Hirschsprung's — RAIR absent | No relaxation of internal anal sphincter with rectal distension |
| Spinal MRI | Suspected sacral agenesis or tethered cord | Sacral deficiency, cord tethering |
CLINICAL PEARL
A loaded rectum on examination = functional constipation; an empty rectum on examination in a child with obvious constipation/distension = think Hirschsprung's disease. This single examination finding is one of the most clinically useful discriminators. The aganglionic rectum in Hirschsprung's disease is contracted and empty — it cannot relax to fill with stool — so the accumulated stool is all proximal to it. In functional constipation, stool collects exactly where the child holds it: in the dilated, hyposensitive rectum. Also remember: Hirschsprung's enterocolitis (explosive bloody diarrhoea + fever + abdominal distension + toxicity) is the most feared complication and can occur even after surgical correction — it is a medical emergency requiring immediate IV fluids, nasogastric decompression, and urgent surgical consultation.