Page 5 of 42
PE23.2 | Constipation — SDL Guide (Part 2)
Management of Constipation in Children
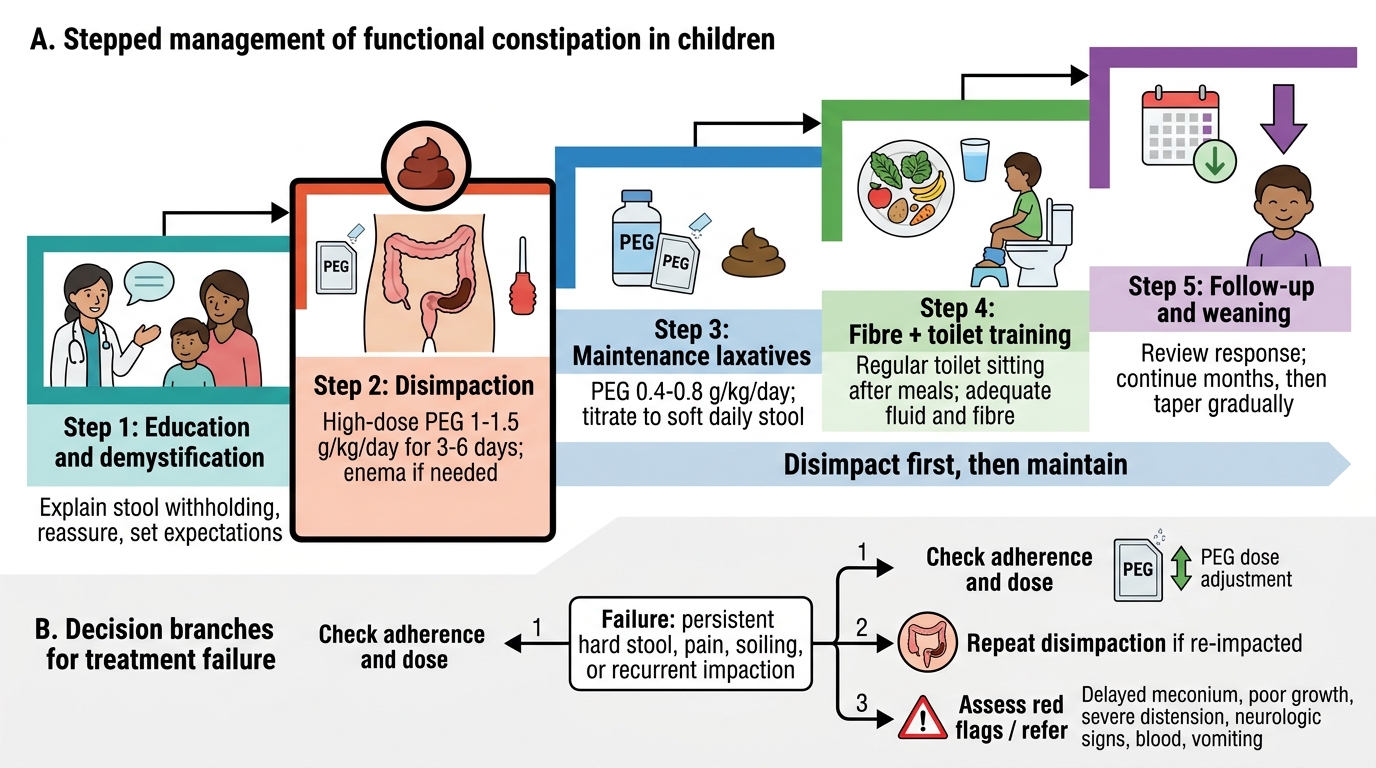
The management of functional constipation in children follows a structured step-wise approach guided by ESPGHAN/NASPGHAN guidelines. The critical rule that underlies all pharmacological therapy is: never start maintenance laxatives on a full rectum — disimpaction must come first. Attempting maintenance therapy without clearing the loaded bowel simply adds more stool to an already impacted system and fails. Parental education and demystification are as important as the pharmacology — families need to understand the physiology of withholding, that soiling is involuntary overflow, and that treatment takes months not days.
Step 1 — Education and demystification:
Explain the withholding cycle clearly to the child and family. Reassure that constipation is functional, not a disease of 'laziness' or 'bad behaviour'. Set realistic expectations — recovery typically takes 6–24 months. Provide a stool diary to monitor frequency and consistency (Bristol Stool Scale).
Step 2 — Disimpaction (if fecal impaction is present):
- Oral disimpaction (preferred): Polyethylene glycol (PEG/macrogol, e.g. Forlax/Movicol) 1–1.5 g/kg/day for 3–6 days — escalate dose until disimpaction is achieved. PEG is the most evidence-based laxative in children.
- Rectal disimpaction (if oral fails or child refuses): Glycerine suppository (young infants/toddlers); sodium phosphate enema (older children) — use cautiously, risk of hyperphosphataemia in young infants.
- Disimpaction is complete when the child is passing soft, unformed stool without effort and no fecal mass is palpable.
Step 3 — Maintenance laxatives (to prevent re-accumulation):
- Polyethylene glycol (PEG): First-line, 0.4–0.8 g/kg/day in divided doses. Adjust to achieve one soft stool per day. Continue for at least 6 months (often 12–24 months); do not stop abruptly.
- Lactulose: 1–2 mL/kg twice daily — safe, well-tolerated in infants; causes osmotic retention of water in the colon. Second-line to PEG. Side effects: bloating, flatulence.
- Stimulant laxatives (senna, bisacodyl): Reserved for short-term use or if osmotic agents fail; not for long-term maintenance in young children.
- Mineral oil (liquid paraffin): Used in some settings; aspirated mineral oil pneumonia is a rare risk in young or cognitively impaired children — use with caution.
Step 4 — Dietary and behavioural measures:
- Increase dietary fibre (age + 5 grams/day as a rough guide); adequate fluid intake
- Reduce excessive cow's milk (>500 mL/day in toddlers may worsen constipation)
- Toilet training: Regular scheduled sitting on the toilet for 5–10 minutes after each main meal (gastrocolic reflex); feet supported on a footstool for optimal defecation posture (anorectal angle opens with hip flexion). Use a reward/star chart for positive reinforcement.
Hirschsprung's disease — surgical management:
- Definitive treatment is surgery: Pull-through procedure (Swenson, Soave, Duhamel) — the aganglionic segment is resected and normally innervated bowel is pulled through and anastomosed to the anus. Performed in specialist centres.
- Bridge to surgery: Colostomy in the normally innervated bowel to relieve obstruction, then definitive pull-through.
- Post-operative complications: Hirschsprung's enterocolitis (the most serious), anastomotic stricture, soiling, constipation relapse.
Functional Constipation in Children: Stepwise Management
SELF-CHECK
A 4-year-old girl with functional constipation presents with fecal impaction. She has not passed stool in 10 days and a large hard fecal mass is palpable in her lower abdomen. What is the CORRECT sequence of management?
A. Start maintenance PEG 0.4 g/kg/day immediately, then add dietary fibre
B. Disimpaction with high-dose PEG 1-1.5 g/kg/day first, then switch to maintenance PEG 0.4-0.8 g/kg/day
C. Sodium phosphate enema daily for 2 weeks, then maintenance lactulose
D. Dietary changes and toilet training only — avoid laxatives in young children
Reveal Answer
Answer: B. Disimpaction with high-dose PEG 1-1.5 g/kg/day first, then switch to maintenance PEG 0.4-0.8 g/kg/day
The critical principle in managing constipation with fecal impaction is 'disimpact first, then maintain'. Starting maintenance-dose laxatives on a rectum full of hard impacted stool simply adds softer stool to the already packed system and produces overflow soiling without clearing the impaction. High-dose PEG (macrogol) at 1-1.5 g/kg/day for 3-6 days is the evidence-based first-line oral disimpaction strategy in children. Once the bowel is clear (child passing soft unformed stool), the dose is reduced to maintenance levels (0.4-0.8 g/kg/day) for a prolonged period of at least 6 months to prevent re-accumulation while the child undergoes toilet training and behavioural retraining.
Self-Assessment: Applied Scenarios
Work through these scenarios before reviewing the discussions. Apply the red-flag checklist and the management algorithm.
Scenario 1: A 7-day-old neonate is referred with progressive abdominal distension from birth. He passed his first meconium at 36 hours. He is breastfed. On examination, the abdomen is markedly distended and tympanic. Per-rectal examination reveals an empty rectum with explosive passage of gas and greenish stool.
Discussion: Red flags — onset from birth, late meconium passage, empty rectum. This is Hirschsprung's disease until proven otherwise. Investigations: Contrast enema (transition zone), suction rectal biopsy (gold standard = aganglionosis). Management: Nil orally, IV fluids, bowel decompression, urgent surgical referral for pull-through procedure after biopsy confirmation. Note: the 'squirt sign' (explosive decompression on rectal examination) is characteristic but not diagnostic — biopsy is mandatory.
Scenario 2: A 5-year-old male is brought with 18-month history of constipation and daily 'accidents' in his underwear. His mother is convinced he is doing it deliberately. Examination reveals a soft, non-tender abdomen with a palpable fecal mass from left iliac fossa to right. Rectal examination reveals a large, loaded rectum.
Discussion: Classic functional constipation with overflow soiling (encopresis). The loaded rectum distinguishes this from Hirschsprung's. Soiling is involuntary overflow, not wilful misbehaviour — counsel the mother firmly on this point. Management: Education, disimpaction with PEG (1-1.5 g/kg/day × 3-6 days), then maintenance PEG (0.4-0.8 g/kg/day) for 6-24 months, toilet training programme, dietary fibre increase, reduce excess milk.
Scenario 3: An 8-month-old infant has had infrequent stools (every 3-4 days) since starting complementary feeds at 6 months. Stools are firm but not painful. He is growing well and feeding normally. Examination is unremarkable.
Discussion: Most likely dietary/transition-related constipation after complementary feeding introduction. Reassure parents. Increase water intake, ensure adequate fibre in complementary foods, reduce cow's milk if >500 mL/day. Glycerine suppository can be used for acute episodes if needed. No organic workup required in the absence of red flags.
SELF-CHECK
Which feature most strongly suggests ORGANIC rather than FUNCTIONAL constipation in a child?
A. Onset at age 2 years coinciding with toilet training
B. Daily soiling of underwear with soft liquid stool around hard impacted mass
C. Failure to pass meconium in the first 48 hours of life
D. Constipation improving with PEG laxative therapy
Reveal Answer
Answer: C. Failure to pass meconium in the first 48 hours of life
Failure to pass meconium within the first 48 hours of life is the strongest red flag for Hirschsprung's disease — the aganglionic segment prevents normal meconium transit from birth. Onset at age 2 coinciding with toilet training (A) is the typical onset of functional constipation. Daily soiling with overflow (B) is characteristic of functional constipation with fecal impaction (overflow encopresis). Response to PEG (D) is expected in functional constipation and helps confirm the diagnosis. Other organic red flags include: onset in the first month of life, absent soiling (true organic obstruction rarely overflows), ribbon-like stools, and empty rectum on examination.
SELF-CHECK
Which laxative is currently considered FIRST-LINE for maintenance therapy in functional constipation in children per ESPGHAN/NASPGHAN guidelines?
A. Lactulose 1-2 mL/kg twice daily
B. Senna syrup once daily
C. Polyethylene glycol (PEG/macrogol) 0.4-0.8 g/kg/day
D. Mineral oil (liquid paraffin) 1-3 mL/kg/day
Reveal Answer
Answer: C. Polyethylene glycol (PEG/macrogol) 0.4-0.8 g/kg/day
Polyethylene glycol (PEG/macrogol) is the first-line maintenance laxative for functional constipation in children per ESPGHAN/NASPGHAN guidelines, with the strongest evidence base. PEG works as an osmotic laxative, retaining water in the colon to soften stool, is tasteless/odourless (can be mixed in drinks), and is safe for long-term use (at least 12-24 months). Lactulose is acceptable as a second-line option, particularly in infants where PEG formulations are not always available; it causes more bloating. Senna (stimulant) is reserved for short-term or add-on use. Mineral oil has risk of aspiration pneumonia in young/cognitively impaired children.