Page 26 of 42
PE23.14 | Fulminant Hepatic Failure — SDL Guide
Learning Objectives
- Define fulminant hepatic failure (FHF) and distinguish it from chronic liver disease
- Enumerate the common causes of FHF in Indian children, with emphasis on viral hepatitis A and E
- Describe the pathophysiology of hepatic encephalopathy and multi-organ involvement
- Grade hepatic encephalopathy using the standard four-grade scale
- Outline the investigation approach including LFTs, coagulation profile, viral markers, and Wilson disease screen
- Describe the management principles: supportive care, N-acetylcysteine, and indications for liver transplant referral
INSTRUCTIONS
Fulminant hepatic failure (FHF) is a paediatric emergency with high mortality if not recognised and managed swiftly. In India, viral hepatitis A and E account for the majority of paediatric FHF cases, but Wilson disease presenting as FHF in older children and adolescents must not be missed — it is treatable and progresses rapidly to death without liver transplant. This module equips you to define FHF precisely (encephalopathy + coagulopathy within 8 weeks, no pre-existing liver disease), grade encephalopathy clinically, identify aetiology systematically, and prioritise life-saving interventions. Understanding the FHF cascade also deepens your comprehension of liver physiology, coagulation, and ammonia metabolism from your Year 1 preclinical base.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 18 — Diseases of Liver and Biliary System (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 385 — Acute Liver Failure (textbook)
- Pediatric Acute Liver Failure Study Group (PALF) — diagnostic criteria and outcomes (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old boy is brought to the emergency department with 5 days of jaundice that has been worsening rapidly. Over the past 24 hours, his parents noticed that he is unusually sleepy, confused about where he is, and has been picking at his bedsheets. On examination he is deeply icteric, his liver is no longer palpable (shrinking, a worrying sign), and he has a liver flap (asterixis). His INR is 3.8 and his serum bilirubin is 18 mg/dL. Anti-HAV IgM returns positive. What is happening, and what needs to be done urgently?
WHY THIS MATTERS
Fulminant hepatic failure is one of the few true hepatological emergencies in paediatrics. It kills through cerebral oedema, uncontrolled bleeding, and sepsis within days of onset. Knowing how to recognise it early — before the child slips into deep coma — directly changes outcomes: timely lactulose prevents HE progression; timely N-acetylcysteine protects residual hepatocytes; timely referral for transplant evaluation can mean the difference between survival and death. In India, hepatitis A (a vaccine-preventable disease) remains a common trigger, making FHF also a public-health teachable moment. This module applies directly to emergency paediatric rotations and postgraduate MCQ examinations.
RECALL
Before proceeding, activate your prior knowledge:
- Bilirubin metabolism (from PY): unconjugated bilirubin is fat-soluble and neurotoxic; the liver conjugates it to water-soluble glucuronides for biliary excretion. In hepatocellular disease, both fractions rise.
- Coagulation factors (from PY/MI): factors II, VII, IX, X (the vitamin-K-dependent factors) are synthesised exclusively in the liver. A damaged liver cannot make them, so PT/INR rises early and sensitively — this is why INR is a cornerstone of the FHF definition.
- Ammonia metabolism (from BI): the urea cycle (predominantly hepatic) converts toxic ammonia to urea. Liver failure means ammonia accumulates and crosses the blood-brain barrier.
- Hepatitis A and E (from MI): both are faeco-orally transmitted RNA viruses causing self-limiting hepatitis in most people; a small proportion progress to FHF, predominantly children and pregnant women (Hep E).
Definition and Clinical Presentation of FHF
Fulminant hepatic failure (FHF) is defined as the development of hepatic encephalopathy and coagulopathy (INR >1.5) within 8 weeks of the onset of liver illness, in a patient with no pre-existing liver disease. This precise definition, adopted by the Pediatric Acute Liver Failure Study Group (PALF), distinguishes FHF from acute-on-chronic liver failure (where underlying cirrhosis exists) and from chronic liver disease presenting acutely. The 8-week time window and the absence of prior liver disease are both essential diagnostic criteria — if a child has underlying Wilson disease in its chronic form, an acute decompensation is classified differently. The term 'fulminant' historically implied a very short onset-to-encephalopathy interval (hyperacute <7 days, acute 7–21 days, subacute 21 days–8 weeks), but clinically the management principles are the same across subtypes.
The clinical presentation of FHF in children is characterised by a rapid, multi-system collapse:
• Jaundice — deep icterus developing over days; may be mild early in some aetiologies (e.g. Wilson disease can have haemolytic crisis)
• Encephalopathy — behavioural change, confusion, drowsiness progressing to coma (graded I–IV; see next section)
• Coagulopathy — spontaneous bleeding, petechiae, haematuria; INR >1.5 by definition
• Hypoglycaemia — because glycogen stores are depleted and gluconeogenesis fails; can cause seizures
• Ascites and oedema — from portal hypertension and hypoalbuminaemia
• Hepatomegaly (early) followed by a shrinking liver (late, ominous — indicates massive necrosis)
• Fetor hepaticus — sweet-musty breath from volatile mercaptans
• Hepatorenal syndrome — acute kidney injury without intrinsic renal disease, from renal vasoconstriction in the setting of systemic vasodilation
Signs that indicate impending cerebral herniation (life-threatening emergency) include decerebrate posturing, pupils fixed/dilated, loss of pupillary light reflex, and Cushing's triad (bradycardia, hypertension, irregular respirations).
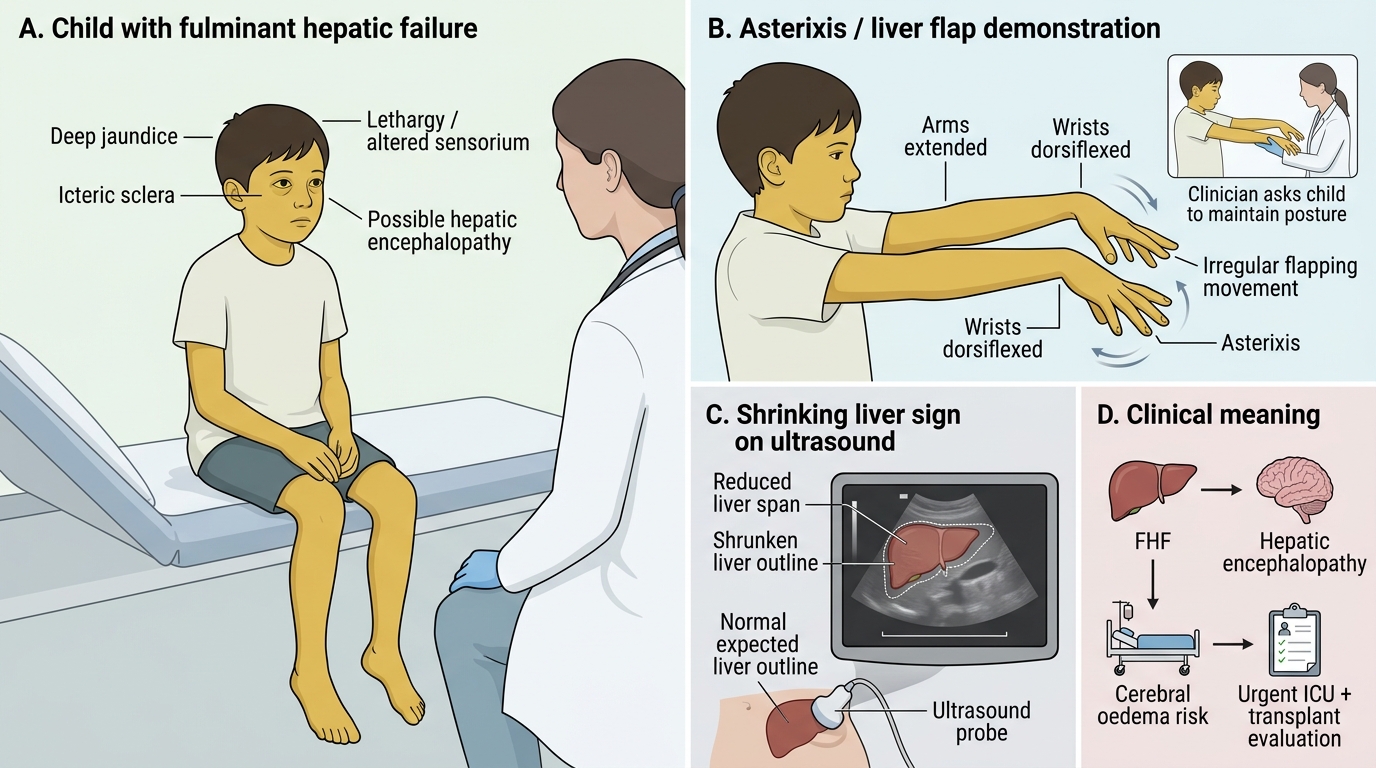
Fulminant Hepatic Failure in a Child
Grading of Hepatic Encephalopathy
Hepatic encephalopathy (HE) in FHF is graded on a four-point scale originally derived from adults but adapted for children — younger children may not display asterixis, and behavioural disturbance or feeding refusal may substitute for the verbal/cognitive features seen in school-age children. Grading is not merely a descriptive exercise: it directly drives clinical decision-making at every step. Grade I and II HE indicate early impairment that may be reversed with lactulose, glucose correction, and removal of precipitants; Grade III–IV HE signals life-threatening cerebral oedema, requires immediate ICU admission, and triggers urgent liver transplant evaluation. The grade assigned at presentation also forms part of prognostic scoring (PALF criteria), so accurate, reproducible grading is a core clinical skill. The West Haven criteria are the most widely used grading system internationally and in Indian practice.
Provided image
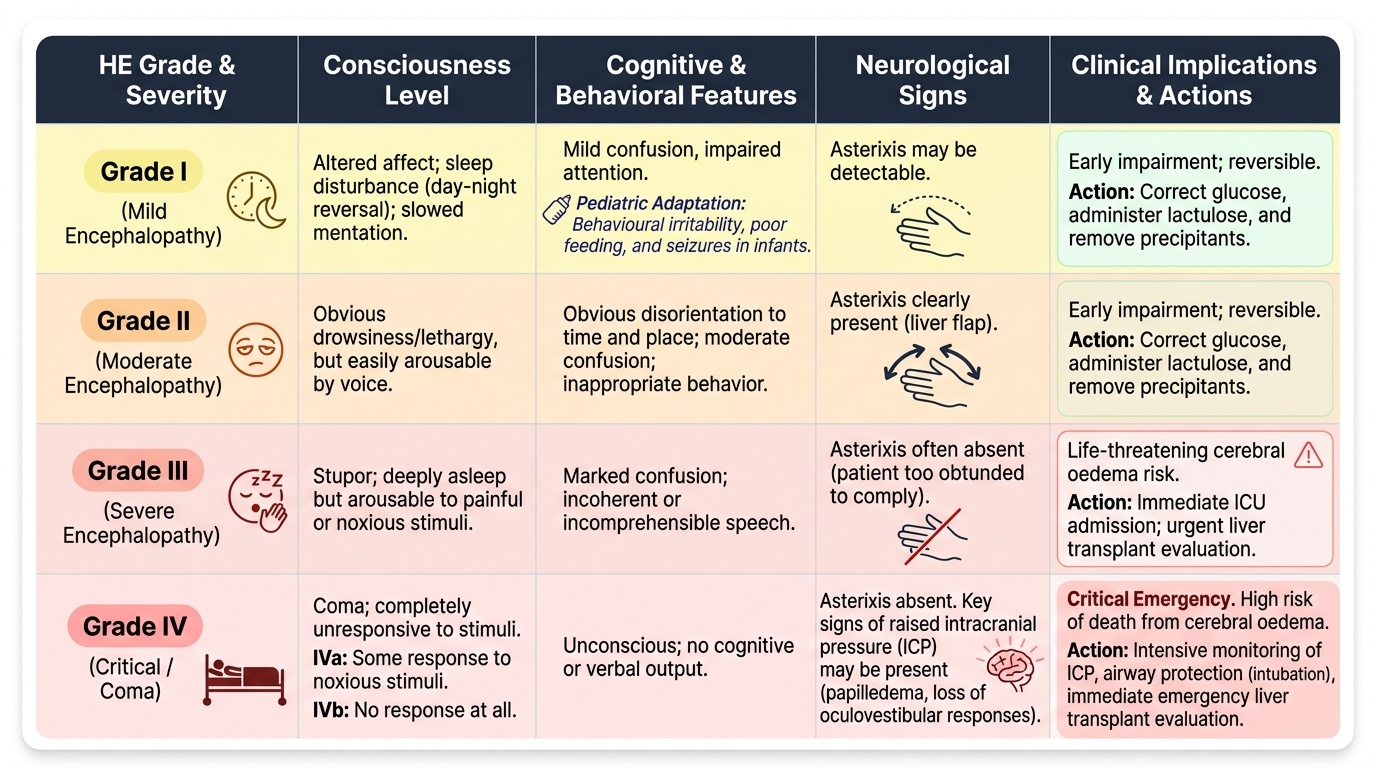
The standard West Haven grading system is:
• Grade I — altered affect, mild confusion, impaired attention, sleep disturbance (day-night reversal), slowed mentation; asterixis may be detectable
• Grade II — obvious disorientation (time and place), moderate confusion, drowsiness but arousable, inappropriate behaviour, asterixis present
• Grade III — marked confusion, stupor, arousable to stimuli/painful stimulation, incoherent speech, asterixis often absent (patient too obtunded to comply)
• Grade IV — coma, no response to stimuli (IVa = some response to noxious stimuli; IVb = no response at all)
Asterixis (liver flap) is tested by asking the child to dorsiflex the wrist with arms outstretched and fingers spread; rhythmic flapping movements at 1–3 Hz indicate Grade I–II encephalopathy. It is absent in Grades III–IV because it requires voluntary motor cooperation.
Key clinical rules in grading:
1. Grade the HE at the time of presentation (the 'worst grade reached' is the definitive grade for management planning)
2. In infants and young children, behavioural irritability, poor feeding, and seizures may substitute for the verbal/cognitive features seen in older children
3. Cerebral oedema is the principal cause of death in Grade III–IV HE — monitor for signs of raised ICP (papilloedema, loss of oculovestibular responses)
SELF-CHECK
A 9-year-old girl presents with jaundice for 10 days. She is now drowsy, disoriented in time and place, and has asterixis on examination. Her INR is 2.1. She had no prior liver disease. What grade of hepatic encephalopathy does she have, and does this qualify as FHF?
A. Grade I HE; qualifies as FHF because INR >1.5 within 8 weeks with no prior liver disease
B. Grade II HE; qualifies as FHF because INR >1.5 within 8 weeks with no prior liver disease
C. Grade III HE; does not qualify as FHF because the onset was >8 weeks ago
D. Grade II HE; does not qualify as FHF because prior liver disease must be confirmed first
Reveal Answer
Answer: B. Grade II HE; qualifies as FHF because INR >1.5 within 8 weeks with no prior liver disease
Drowsiness and disorientation in time and place with asterixis present is Grade II HE. She qualifies as FHF: encephalopathy present + INR >1.5 (2.1) + onset within 8 weeks + no pre-existing liver disease. Grade III would require stupor arousable only to stimuli; Grade I would be mild confusion with attention impairment but still fully arousable and oriented.
Aetiology in Children
The aetiology of FHF in Indian children differs substantially from Western series, reflecting local epidemiological conditions including sanitation, vaccination coverage, and genetic predispositions. Identifying the aetiology is not merely academic — it is a clinical imperative because some causes have specific, life-saving antidotes or therapies: paracetamol toxicity responds to N-acetylcysteine; Wilson disease requires emergency liver transplant since chelation alone is insufficient and penicillamine can worsen the acute presentation; autoimmune hepatitis may respond to corticosteroids when the diagnosis is confirmed histologically and encephalopathy is not yet advanced. A structured aetiological approach therefore shapes every subsequent management decision, and the workup should proceed simultaneously with supportive care, not after stabilisation. In approximately 30–40% of paediatric FHF cases in India, the aetiology remains indeterminate despite a full screen — these are managed supportively with active transplant evaluation.
Infectious / viral causes (commonest in India):
• Hepatitis A virus (HAV): Most common single cause of paediatric FHF in India. Transmitted faeco-orally; FHF occurs in <1% of HAV infections but is severe. Diagnosed by anti-HAV IgM antibody (serum). Vaccine-preventable.
• Hepatitis E virus (HEV): Second most common; particularly severe in pregnant women (20–30% mortality) but also affects children in epidemic settings. Diagnosed by anti-HEV IgM or HEV RNA.
• Hepatitis B (HBV): Less common in children due to NIS vaccination; FHF from superinfection (HBV + HDV) or reactivation. Check HBsAg, anti-HBc IgM.
• Other viruses: EBV, CMV, herpes simplex (especially neonates and immunocompromised), dengue, adenovirus.
Metabolic / genetic causes:
• Wilson disease: Presents as FHF in children and adolescents (typically 5–35 years). KEY: unlike chronic Wilson, Kayser-Fleischer rings may be absent in acute presentation, but low serum ceruloplasmin (<20 mg/dL), Coombs-negative haemolytic anaemia (from copper release), and markedly elevated urinary copper are clues. Alkaline phosphatase is paradoxically low in Wilson FHF — an important diagnostic pointer. Urgent liver transplant evaluation is essential.
• Neonatal haemochromatosis (gestational alloimmune liver disease): presents in neonates with FHF.
Drug-induced / toxic:
• Paracetamol (acetaminophen) overdose: Commonest drug cause; hepatotoxic at ~150 mg/kg single dose; metabolite NAPQI causes zone 3 hepatocyte necrosis. Treat with N-acetylcysteine (NAC).
• Valproate (anticonvulsant): idiosyncratic hepatotoxicity, especially in young children on polytherapy.
• Isoniazid, halothane, herbal medicines: Less common but recognised causes.
Autoimmune hepatitis (AIH):
• Can present acutely as FHF in children; check ANA, anti-SMA (smooth muscle antibody), anti-LKM1; biopsy shows plasma-cell-rich interface hepatitis. Treatable with immunosuppression if compatible histology.
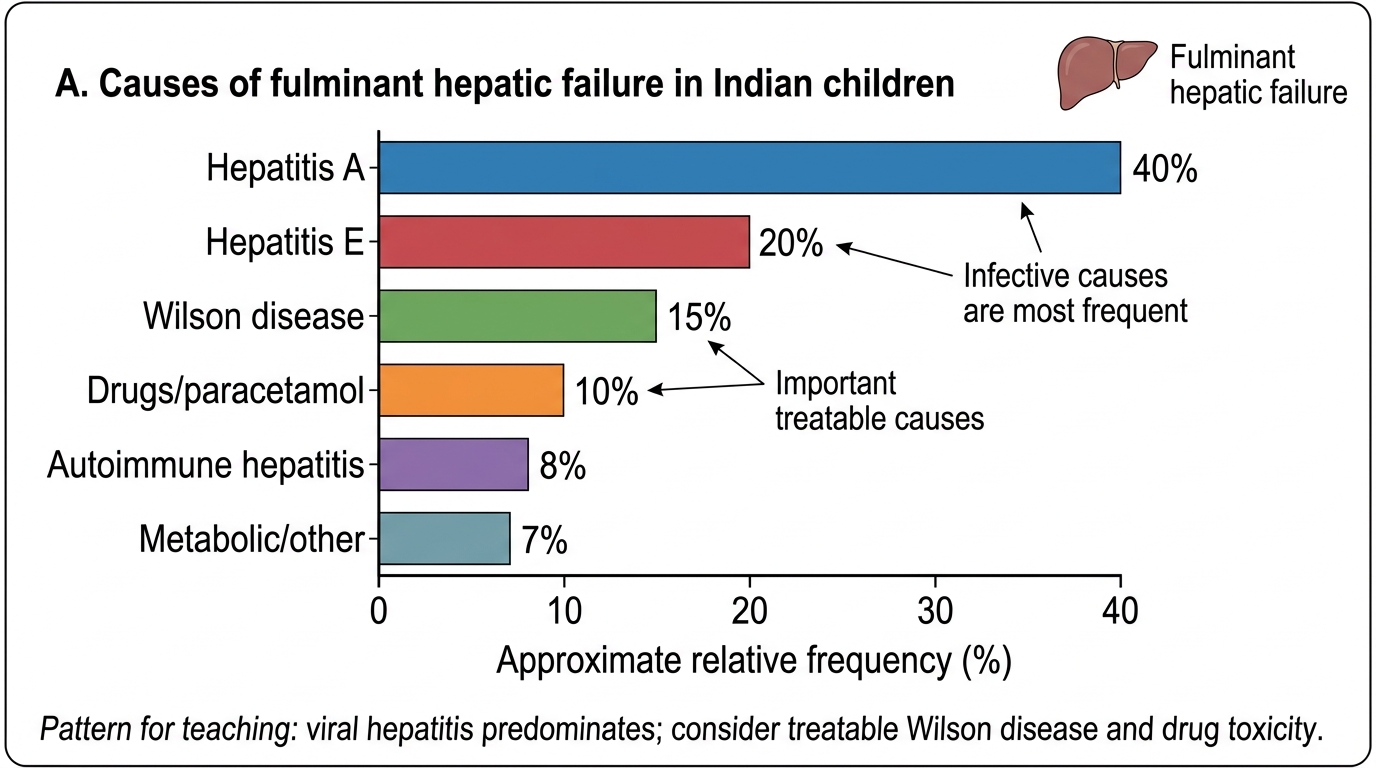
Causes of Fulminant Hepatic Failure in Indian Children