Page 24 of 31
PE24.22-23 | Emergency Communication and Consent — SDL Guide
Learning Objectives
- Counsel parents of a dangerously ill or terminally ill child using a structured breaking-bad-news framework (SPIKES)
- Obtain informed consent for paediatric emergency procedures, including explaining the emergency exception doctrine
- Describe the legal and ethical basis for proxy consent by parents/guardians for children under 18 years
- Respond appropriately to parental grief, denial, anger, and refusal during a paediatric emergency
INSTRUCTIONS
Communication and consent are not softer skills supplementary to clinical competence — they are clinical competencies in their own right, with direct consequences for patient outcomes and medicolegal standing. In a paediatric emergency, the clinician is simultaneously managing a critically ill child and communicating with terrified parents who are experiencing one of the worst moments of their lives. Getting this right — being clear, compassionate, and legally sound — is as important as getting the drug dose right. This module provides a structured framework for both breaking bad news and obtaining emergency consent in the paediatric context.
References
- Ghai Essential Pediatrics, 9th edition, Ch 27 (Ethical and Legal Aspects of Paediatric Care) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 4 (Ethics in Paediatric Practice) (textbook)
- Indian Medical Council (Professional Conduct, Etiquette and Ethics) Regulations 2002 (guideline)
- Parikh's Textbook of Medical Jurisprudence and Toxicology, 7th edition, Ch 2 (Medical Ethics and Consent) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 3 AM. An 8-year-old boy with bacterial meningitis has been in the emergency department for 45 minutes. His GCS has dropped from 12 to 8. He needs an urgent lumbar puncture and IV antibiotics. His father, who just arrived from a three-hour journey, grabs your arm: 'Don't touch my son until you tell me exactly what is happening and get my permission.' You have three minutes. What do you say, and how do you handle the consent?
WHY THIS MATTERS
Communication breakdowns in paediatric emergencies are among the leading causes of complaints, litigation, and — most importantly — poor outcomes. A parent who does not understand what is happening to their child cannot give meaningful consent, cannot participate in decisions about aggressive versus palliative care, and cannot prepare themselves and their family for the possibility of loss. Equally, a clinician who proceeds without consent in a non-emergency situation, or who delays treatment in a genuine emergency waiting for unreachable parents, has made a serious ethical and legal error. These skills — structured bad-news communication and legally valid emergency consent — are testable in the MBBS examination and are the foundation of every subsequent clinical interaction involving a critically ill child and a frightened family.
RECALL
Recall from your forensic medicine and professional ethics training:
• Informed consent requires five elements: disclosure (adequate information), understanding (patient comprehends), voluntariness (no coercion), capacity (ability to decide), and authorisation (explicit agreement).
• Capacity — the ability to understand, retain, weigh, and communicate a decision — is assessed at the time of each decision, not permanently assigned. In adults, it can be temporarily lost and regained (unconsciousness, sedation).
• Age of majority in India is 18 years. Children below 18 lack legal capacity to consent for medical treatment independently; a parent or legal guardian provides proxy consent.
• Therapeutic privilege (withholding information because it might upset the patient) is generally considered unethical in modern medical practice — it denies autonomy. The duty to disclose is the default.
• The Guardians and Wards Act 1890 governs guardianship of minors in India; a parent is the natural guardian and primary proxy decision-maker for a child's medical care.
Why Communication and Consent Are Emergency Skills in Paediatric Care
Communication and consent are described as 'soft skills' in some curricula, but this framing misrepresents their clinical and legal significance. In the paediatric emergency context, communication failures carry measurable consequences: parents who receive inadequate information about their child's prognosis make poorly informed decisions about interventions; parents who are not adequately counselled after a child's death are more likely to develop complicated grief and to initiate litigation; and clinicians who proceed without consent for non-emergency procedures expose themselves to allegations of assault regardless of the quality of the clinical care delivered. The inverse is equally true: a clinician who communicates clearly, compassionately, and transparently under pressure builds trust with families that sustains the clinical relationship through crisis.
The paediatric emergency setting creates specific communication challenges that do not arise in elective settings. Time is compressed — the window to explain a diagnosis, check understanding, obtain consent, and begin treatment may be measured in minutes rather than the 30-60 minutes available in an outpatient consultation. The parents are not the patient but are the primary decision-makers, creating a triangular communication relationship between clinician, child, and parent. The child's condition is changing rapidly, requiring updated communication at each transition point (from 'serious' to 'critical', from 'curative intent' to 'palliative'). And the emotional intensity is extreme: parents in a resuscitation area may be in acute psychological shock, unable to process complex information delivered in medical language at normal conversational speed.
The two competencies this module addresses — breaking bad news (PE24.22) and obtaining informed consent (PE24.23) — are complementary but distinct skills. Breaking bad news is primarily a communication task: structuring information delivery to maximise comprehension while minimising psychological harm. Obtaining consent is primarily an ethical-legal task: ensuring that the procedure about to be performed on a patient who cannot legally consent for themselves has been authorised by the appropriate proxy in the legally required manner. Both require practice in simulated environments before a real emergency — communication under crisis is a skill, and skills are built through rehearsal, not reading.
Consent Decision Tree in Paediatric Emergencies
Governing Principles: Informed Consent, Capacity, and Proxy Decision-Making
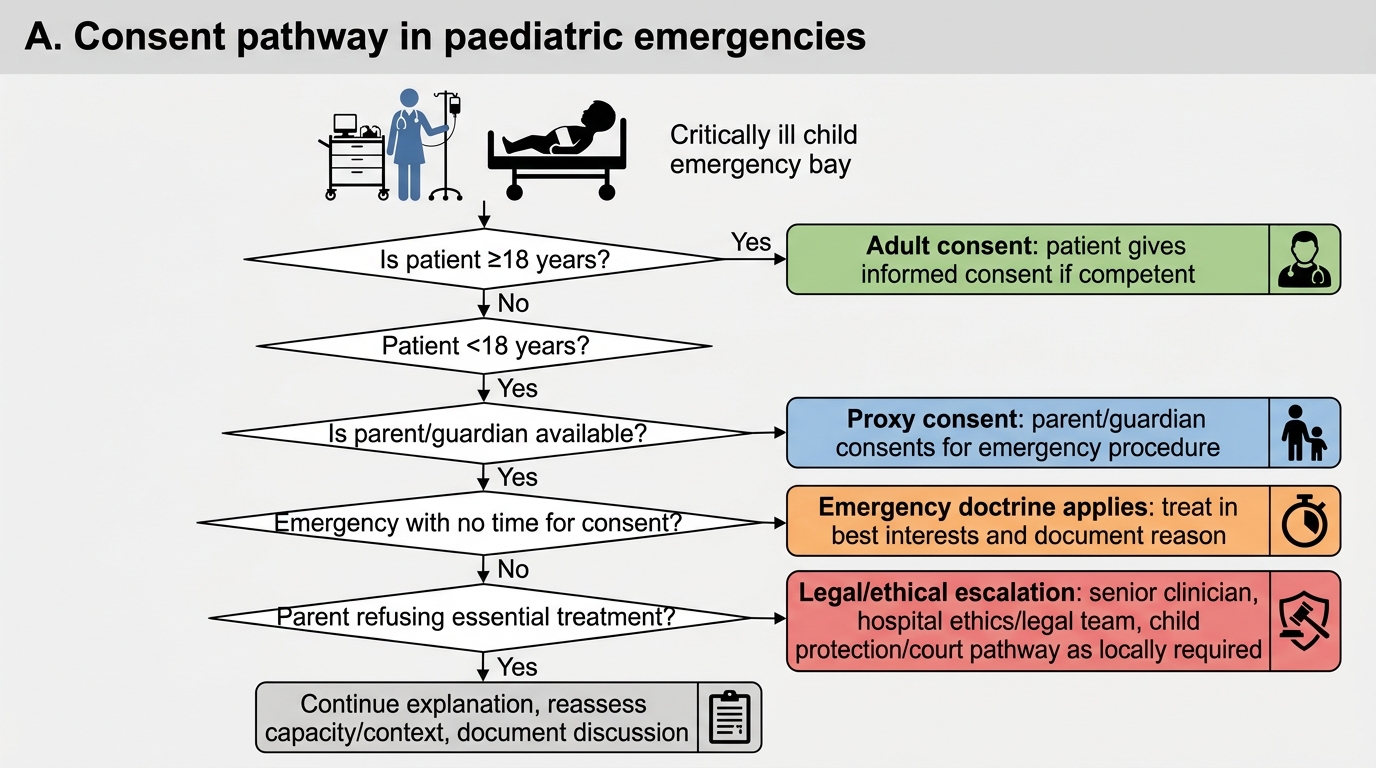
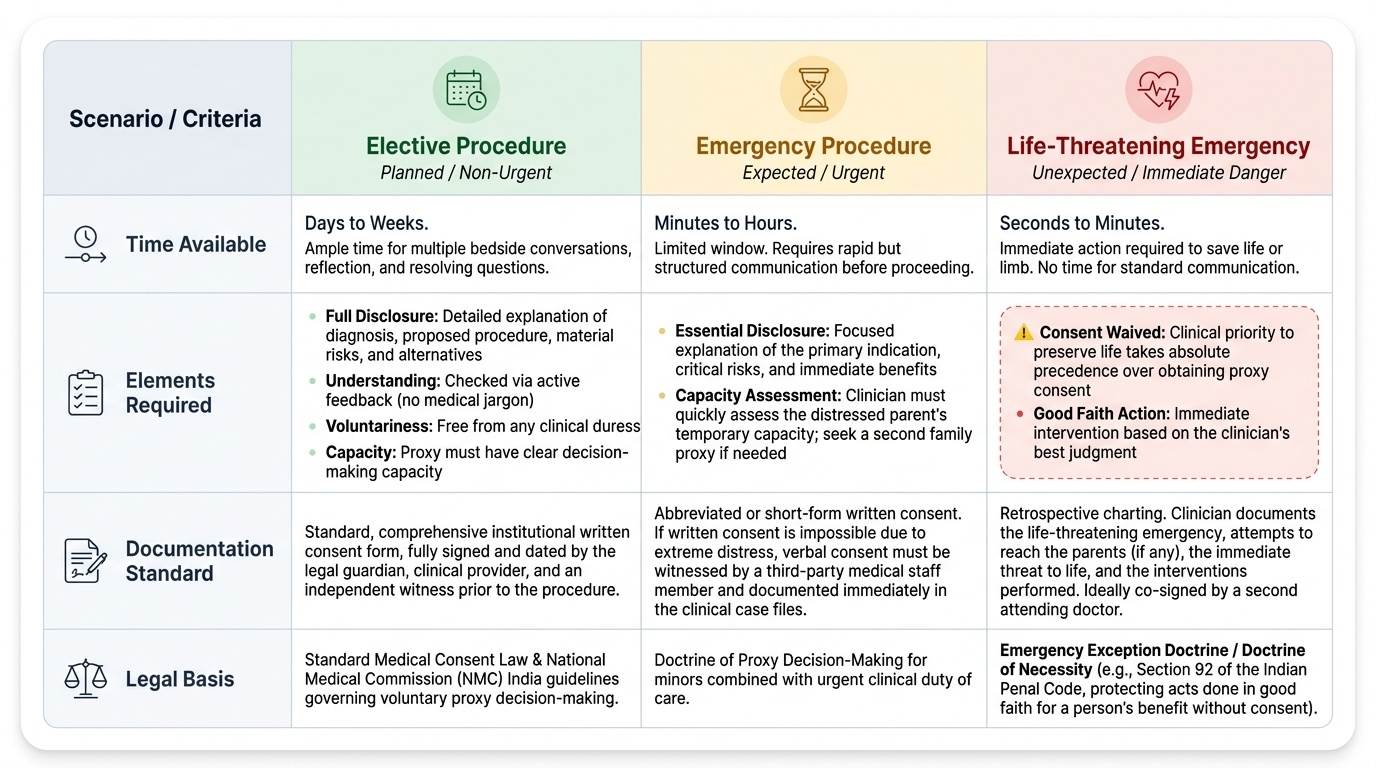
The legal and ethical framework for consent in paediatric emergencies in India rests on the intersection of general medical consent law, child protection law, and the specific clinical doctrine of emergency exception. Understanding this framework allows the clinician to act correctly in each of the three main scenarios: the expected emergency (a procedure that is planned but urgent), the unexpected emergency (a child who deteriorates and needs intervention before parents can be reached), and the contested consent (a parent who refuses treatment that the clinician believes is necessary to save the child's life). A common error among junior clinicians is to treat consent as a form-signing event rather than as a communication process — the signed form is the documentation of a conversation that must have already happened, not a substitute for it. This misunderstanding leads to the practice of presenting a consent form to a distressed parent at the bedside without any prior explanation, which simultaneously fails the ethical requirement for disclosure and the legal requirement for voluntariness (a parent who does not understand what they are signing has not truly consented). Building the habit of treating consent as a structured conversation — with a beginning (identify yourself and the procedure), middle (explain the indication, risks, and alternatives), and end (check understanding, obtain explicit agreement, document) — is the most important single practice change from this module.
Provided image
Elements of valid informed consent (applying to proxy consent for a child):
1. Disclosure — the parent must be given adequate information: the diagnosis, the proposed procedure, its purpose, the material risks, alternatives, and the consequences of not proceeding.
2. Understanding — the information must be given in language the parent can comprehend. Medical jargon without explanation does not constitute valid disclosure.
3. Voluntariness — consent must be given freely, without coercion. A parent who signs a consent form under duress ('sign this or we won't treat your child') has not given valid consent.
4. Capacity — the proxy (parent/guardian) must have capacity to make the decision. Parents in severe psychological distress may temporarily have impaired capacity; in such cases, a second family member or guardian may need to provide consent.
5. Authorisation — explicit verbal or written agreement. For significant procedures, written consent is the standard; for minor procedures (IV cannulation, blood draw), verbal consent is documented in the notes.
Proxy consent and the role of the parent:
In India, a child under 18 years cannot legally consent for medical treatment independently. The natural guardian (mother or father under the Guardians and Wards Act 1890) provides proxy consent. For a child in state care, the legal guardian appointed by the court is the proxy. In everyday practice, either parent may give consent; if parents disagree, both should be engaged and, if the disagreement involves a life-critical decision, the treating team should seek institutional ethics committee guidance.
Assent from older children and adolescents:
While a child under 18 cannot legally consent, the ethical principle of respect for developing autonomy requires that older children be involved in decisions about their own care to the extent of their capacity. A 7-year-old can provide meaningful assent (agreement) to a procedure after a simple explanation; a 14-year-old can participate substantively in a discussion about their treatment options and should be heard, though the parent provides the legal consent. Assent is sought — but its refusal does not have the legal weight of an adult's refusal of consent.
The emergency exception doctrine:
When: (a) a child requires immediate treatment; (b) delay to obtain consent would cause irreversible harm or death; and (c) the proxy decision-maker is unavailable or unable to consent in the time available — treatment may proceed without prior consent under the emergency exception (also called implied or emergency consent). The justification is that a reasonable parent/guardian would consent to life-saving treatment for their child. This exception is not a blank authorisation: it applies to the minimum intervention necessary to stabilise the child; it does not authorise elective or non-urgent procedures; and it requires immediate documentation explaining why the exception was invoked, what intervention was performed, and when parental consent was obtained retrospectively.
SELF-CHECK
A 5-year-old needs urgent IV antibiotics for suspected bacterial meningitis. His parents were contacted 20 minutes ago but live 2 hours away and cannot be reached again. The child's GCS is falling. Under what doctrine may you proceed with treatment, and what must you do immediately after?
A. Therapeutic privilege — document that you informed the child instead
B. Emergency exception doctrine — proceed with the minimum essential intervention, then document why consent was bypassed and obtain retrospective consent when the parents arrive
C. You cannot proceed without consent under any circumstances; continue trying to contact the parents
D. Implied consent from the nurse who is present in the room
Reveal Answer
Answer: B. Emergency exception doctrine — proceed with the minimum essential intervention, then document why consent was bypassed and obtain retrospective consent when the parents arrive
The emergency exception (emergency doctrine) permits treatment without prior consent when delay would cause irreversible harm and the proxy is unavailable. The conditions are met: meningitis is life-threatening, parents cannot be reached, and delay risks herniation. The essential steps after proceeding are: (1) document the clinical basis (falling GCS, inability to reach parents, time documented); (2) perform only the minimum essential intervention; (3) obtain retrospective consent and explanation when parents arrive. Therapeutic privilege is for withholding upsetting information, not a consent bypass. A nurse cannot provide proxy consent for a child.
Breaking Bad News: SPIKES Protocol in Paediatric Emergencies
Breaking bad news is one of the most demanding communication tasks in clinical medicine, and it is made harder in paediatric emergencies by the time pressure, the extreme emotional state of the parents, and the distressing nature of childhood illness itself. The SPIKES protocol, originally developed by Buckman and colleagues for oncology settings, provides a structured six-step framework that is widely adapted for paediatric emergency communication. It does not eliminate the distress of a devastating diagnosis — no framework can — but it organises the communication in a way that maximises parental comprehension, minimises preventable additional harm (such as delivering a diagnosis in a public corridor), and gives the clinician a clear sequence to follow under pressure.
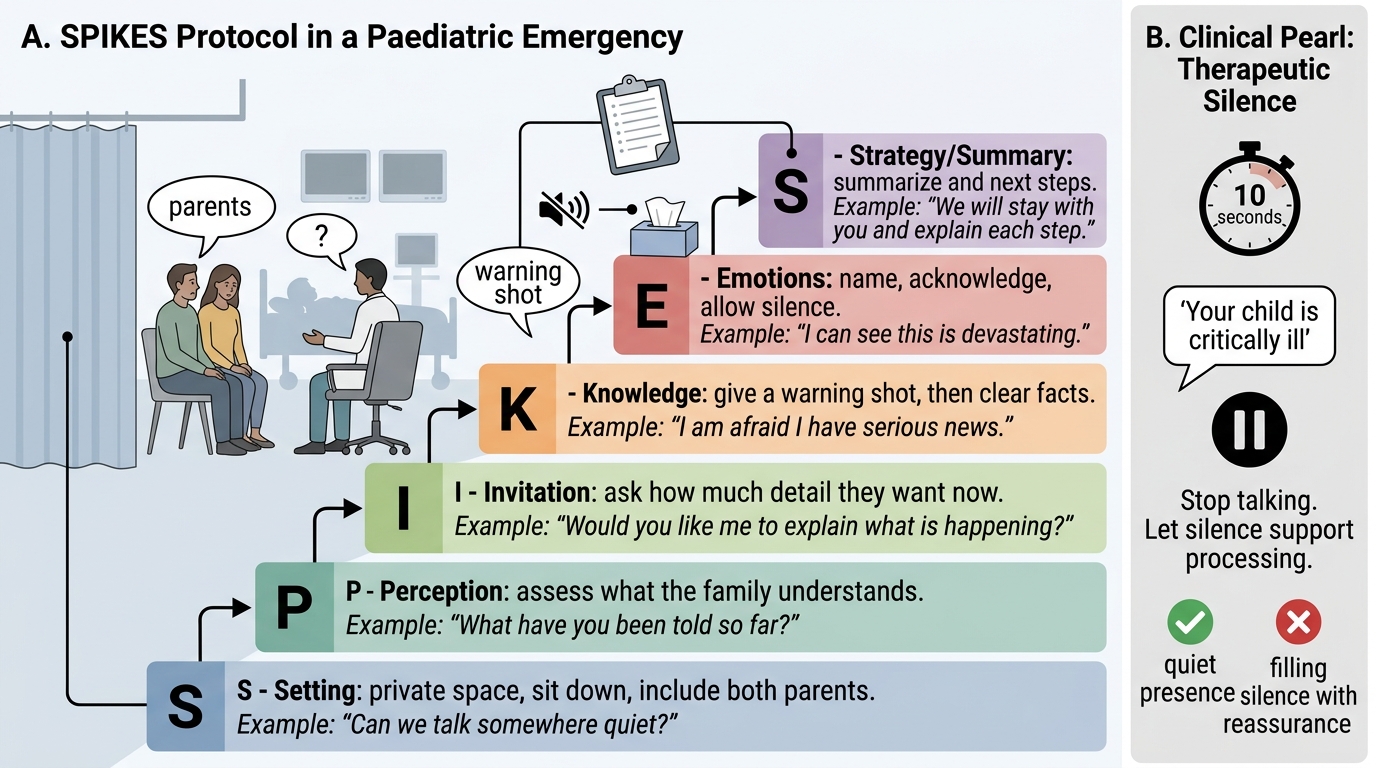
The six steps of SPIKES are:
S — Setting:
Create the right environment for the conversation before it begins. For a paediatric emergency, this means: (a) find a private space, even if it is the family waiting room with the door closed — never break bad news in a busy corridor or in the child's presence without preparation; (b) sit down at the parent's level — standing above a seated parent communicates authority, not partnership; (c) turn off your pager if safe to do so, or hand over to a colleague for 10 minutes; (d) have a nurse or social worker present if available — a witness is both supportive and medicolegally appropriate; (e) begin by introducing yourself: name, role, and that you are responsible for their child's care.
P — Perception:
Before delivering information, find out what the parent already knows: 'What have the doctors told you so far?' or 'What's your understanding of why your child was brought in today?' This accomplishes two things: it prevents you from dramatically re-announcing something the parent already knows, and it calibrates your language to their existing understanding. A parent who already knows their child has meningitis does not need the diagnosis explained from scratch — they need information about severity and treatment plan.
I — Invitation:
Ask permission to share information: 'I have some serious news about your child's condition — are you ready to hear it now, and is there someone you would like to have with you?' This step respects autonomy and gives the parent a brief moment of psychological preparation. Most parents will say yes; the rare parent who says 'not yet' has told you something important about their coping state.
K — Knowledge (delivering the news):
Deliver the information in clear, plain language. Use short sentences. Avoid jargon: say 'infection in the brain's covering' rather than 'bacterial meningitis with meningeal inflammation.' Fire a warning shot ('I'm afraid the news is serious') before the diagnosis to help the parent brace for the information. Pause after the key sentence — the brain needs time to process devastating information, and speaking too continuously prevents absorption. 'Your child has a very serious infection in the brain. This is called meningitis.' Pause. 'We have started treatment, but I need to tell you the next few hours are critical.'
E — Emotions:
Respond to the emotional reaction before continuing with clinical information. Acknowledge the response: 'I can see this is a terrible shock' or 'It's completely understandable to feel frightened.' Do not immediately pivot to treatment logistics — this feels dismissive. An empathic statement ('This must be incredibly hard to hear') is not an empty formula; it signals that the clinician sees the parent as a person, not a barrier to be managed.
S — Strategy and Summary:
Close the conversation with a clear plan: what happens next, what treatment has been started, when you will give the next update, and what the parent can do (stay with the child, contact other family members). A clear 'what happens next' gives the parent something to hold onto when everything else feels out of control. Document the conversation in the notes: time, who was present, what was said, and the parent's response.
SPIKES Protocol for Paediatric Emergency Conversations
CLINICAL PEARL
Silence is a clinical tool. After delivering the critical sentence in a bad-news conversation ('Your child is critically ill' or 'We could not save your child'), stop talking. Resist the impulse to fill the silence with more information, reassurances, or plans. The parent needs the silence to begin processing. Speaking over the silence is not compassionate — it is anxiety management for the clinician, not support for the family. Ten seconds of silence in a breaking-bad-news conversation is the most powerful thing you can offer.