Page 25 of 31
PE24.22-23 | Emergency Communication and Consent — SDL Guide (Part 2)
Obtaining Informed Consent in Paediatric Emergencies
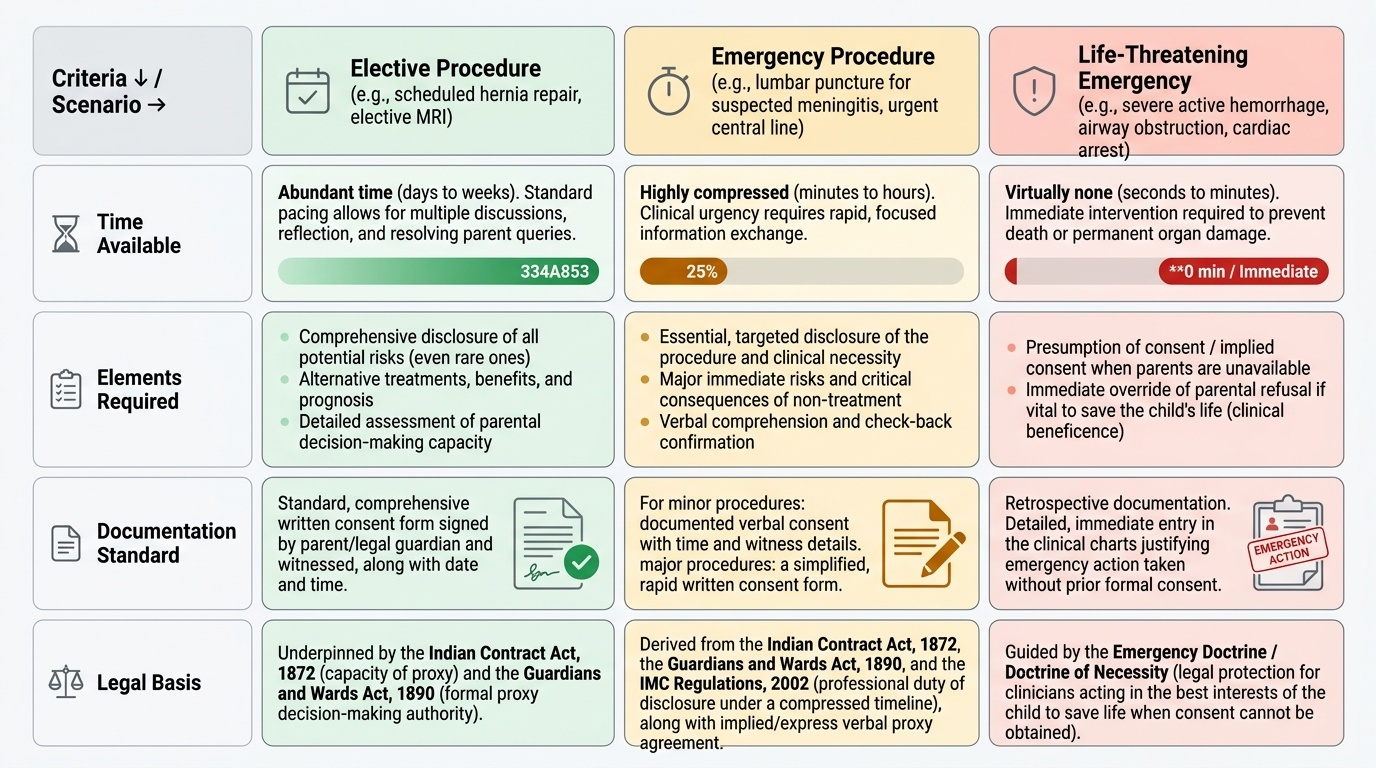
Obtaining consent in a paediatric emergency differs from elective consent in pace, depth, and sometimes in legal basis. The clinical urgency compresses the time available for information exchange, the parent's emotional state may impair comprehension, and the clinician must simultaneously assess what information is genuinely essential to disclose versus what is excessive detail that increases anxiety without aiding decision-making. The legal standard for emergency consent in India is not formally codified in a single statute, but derives from the Indian Contract Act 1872 (capacity and validity of agreement), the Guardians and Wards Act 1890 (proxy authority), and the IMC Regulations 2002 (professional duty of disclosure). Understanding this framework allows the clinician to act both ethically and legally.
Provided image
Consent procedure for an emergency paediatric procedure (e.g., lumbar puncture, intubation, central venous access):
1. Identify who is present: are one or both parents present? Is there a legal guardian?
2. Briefly assess the parent's capacity to consent (are they in a state of psychological crisis so severe they cannot process information? — rare but possible).
3. Deliver the essential disclosure: what procedure, why it is needed now, the main risk of the procedure (e.g., 'a small risk of headache or, very rarely, infection'), and the risk of not doing it ('without this, we cannot confirm the diagnosis and start the right antibiotics').
4. Check understanding: 'Does that make sense? Do you have any questions before I ask for your permission?'
5. Obtain explicit agreement: 'Do I have your permission to proceed?' Document verbal consent with time, what was disclosed, and who consented.
6. For significant procedures: a written consent form signed by the parent and witnessed, with the time and date recorded.
Consent for life-saving treatment of a minor:
The most ethically challenging consent scenario in paediatric emergencies is the parent who refuses treatment that the clinician believes is necessary to save the child's life. Common scenarios include: a Jehovah's Witness family refusing blood transfusion for a severely anaemic or bleeding child; a parent refusing a lumbar puncture for a child with suspected meningitis due to fear of the procedure; a parent insisting on discharge against medical advice for a critically ill child. In each case, the legal principle is that parental proxy consent cannot be used to deny a child the treatment necessary to preserve life — the state (and the medical team as agent of the state's parens patriae authority) has an overriding interest in the child's welfare. The clinical steps are: (1) engage additional communication resources (senior colleague, social worker, translator if language barrier); (2) document the refusal; (3) seek institutional ethics committee guidance or, in extremis, court authorisation for treatment; and (4) if the child's condition is immediately life-threatening and there is no time for legal process, treat under the emergency exception and document fully.
Adolescent consent and assent:
For a 16-year-old or mature adolescent who can demonstrate understanding and reasoning capacity, the treating team should respect their expressed preferences while recognising that legal consent still requires the parent/guardian. A 16-year-old's informed refusal of treatment should prompt serious ethical discussion, even though it does not have the absolute legal force of an adult refusal.
SELF-CHECK
Parents of a 3-year-old with severe anaemia (Hb 3.5 g/dL, in respiratory distress) refuse blood transfusion on religious grounds. The child is deteriorating. What is the correct sequence of steps?
A. Respect parental autonomy — do not transfuse without consent under any circumstances
B. Transfuse immediately without further communication since the child is deteriorating
C. Engage senior colleague and attempt further communication; document refusal; seek ethics committee or court order if time permits; if child is immediately life-threatening with no time for legal process, transfuse under emergency doctrine with full documentation
D. Transfer the child to another hospital where the parents may agree
Reveal Answer
Answer: C. Engage senior colleague and attempt further communication; document refusal; seek ethics committee or court order if time permits; if child is immediately life-threatening with no time for legal process, transfuse under emergency doctrine with full documentation
This is the parens patriae scenario — a parent's proxy consent cannot be used to deny a child life-saving treatment. The correct sequence is: (1) engage senior colleague to attempt additional communication; (2) document the refusal in detail; (3) seek ethics committee guidance or court authorisation if time permits; (4) if the child is in immediate danger of death and legal process is impossible in the time available, transfuse under the emergency doctrine with complete documentation of all steps. Option A treats parental autonomy as absolute, which it is not when a child's life is at risk. Option B skips communication steps that are legally and ethically required.
Interpreting and Responding to Family Responses in Crisis
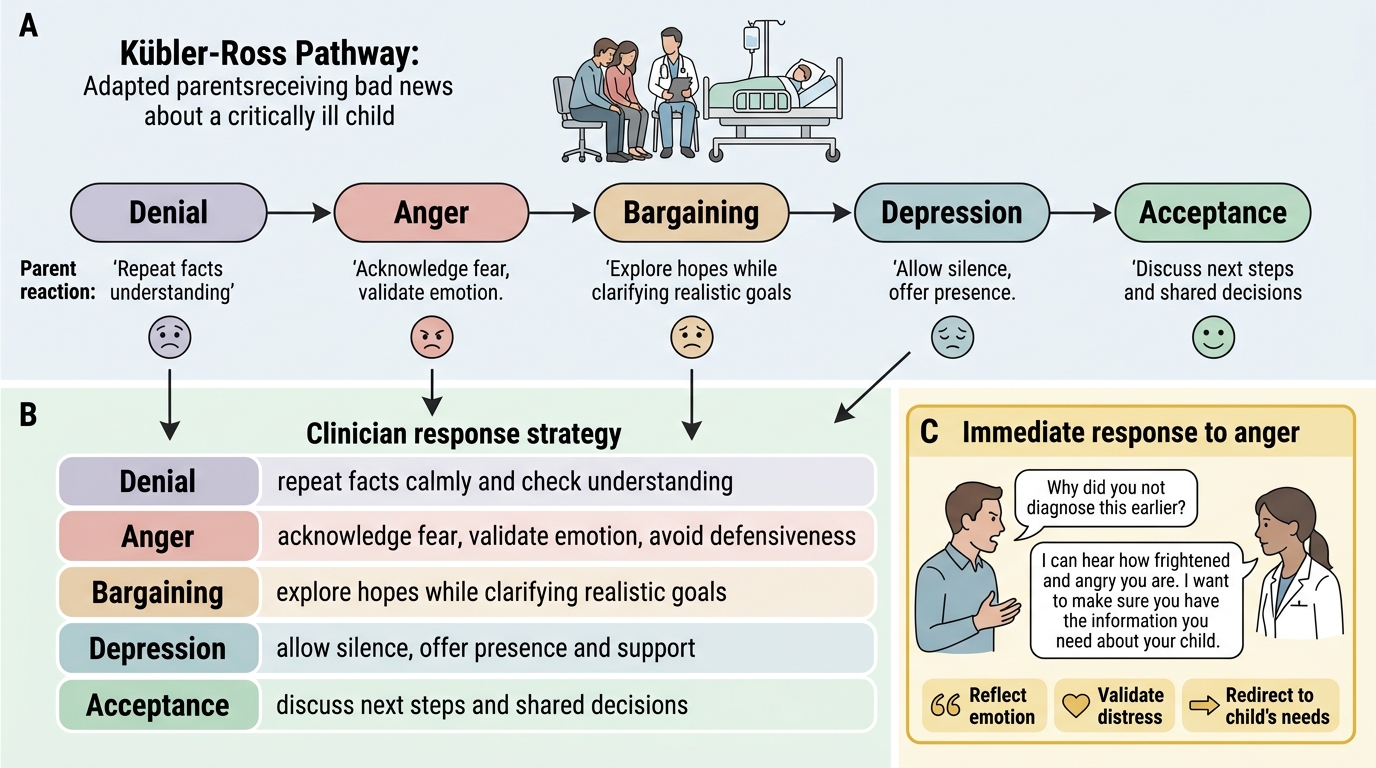
Parents receiving bad news about a critically ill child do not respond uniformly, and the ability to recognise and respond appropriately to different emotional states — grief, denial, anger, bargaining, withdrawal — is a clinical skill that directly determines whether the communication serves the family or inadvertently damages the therapeutic relationship. Understanding the psychological framework of grief responses helps the clinician interpret parental behaviour that might otherwise seem irrational or obstructive as a predictable human response to extreme distress.
The Kübler-Ross stages of grief (denial, anger, bargaining, depression, acceptance), while not a rigid sequential model, describe common emotional positions that parents may occupy during and after a bad-news conversation. A parent who says 'This can't be right — get a second opinion' is not being difficult; they are in denial, a normal protective psychological response. A parent who shouts 'You've done something wrong!' is not necessarily making a complaint; they may be in acute anger from fear and helplessness. Recognising the stage allows the clinician to respond appropriately: denial is met with gentle, patient repetition of clear information (not arguing); anger is met with de-escalation, acknowledging the distress without being defensive; bargaining ('If we do this procedure, will the child be fine?') requires honest, kind handling — neither false reassurance nor brutal bluntness.
Cultural considerations in the Indian paediatric context:
In many Indian family structures, medical communication is directed to a senior male family member (grandfather, uncle, eldest son) as the family spokesperson, rather than directly to the parents. This may create tension when the parents are present but a different family member is acting as decision-maker. The clinician's approach should be: (a) identify who the parents are and ensure they have been spoken to directly, regardless of the family hierarchy; (b) respect the family spokesperson role while ensuring that the legal proxies (parents) are included and informed; (c) avoid using the family spokesperson as an interpreter for complex medical information — translation of medical information by an untrained family member routinely introduces errors.
Non-verbal communication:
In a crisis conversation, non-verbal signals convey as much as words: eye contact (respectful attention), posture (sitting forward, not leaning back or looking at a screen), physical proximity (close enough to feel present, not so close as to invade), and appropriate touch (a hand on the shoulder at a moment of extreme distress is often appropriate, though cultural norms must be respected).
Managing disagreement between family and clinical team:
Disagreement about prognosis or treatment plan is common in paediatric intensive care. The clinician's role is not to win the argument but to ensure the family understands the clinical evidence, to explore the values and fears driving the disagreement, and to find a path that respects both the child's best interests and the family's legitimate role in decision-making. A second opinion, ethics committee involvement, or a palliative care consultation may be needed when disagreements persist.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Parental Grief Responses During Pediatric Bad-News Conversations
SELF-CHECK
During a bad-news conversation, a father becomes angry and shouts: 'You are incompetent — why did you not diagnose this earlier?' What is the most appropriate immediate response?
A. Defend your clinical decisions and explain why the diagnosis could not have been made earlier
B. End the conversation and ask him to leave until he is calm
C. Acknowledge the distress: 'I can hear how frightened and angry you are — that is completely understandable. I want to make sure you have all the information you need about what is happening with your child'
D. Call security in case the situation escalates
Reveal Answer
Answer: C. Acknowledge the distress: 'I can hear how frightened and angry you are — that is completely understandable. I want to make sure you have all the information you need about what is happening with your child'
Anger in a crisis is almost always an expression of fear and helplessness, not a genuine accusation requiring a defence. The correct response is empathic acknowledgement — reflect the emotion, validate it, and redirect to the child's needs. Arguing or defending produces counter-productive escalation; ending the conversation abandons the family at their most vulnerable moment; calling security is a last resort for physical threat, not for verbal anger from a frightened parent. Acknowledging the distress de-escalates the acute anger and allows communication to resume.
Applied Practice: Simulated Breaking-Bad-News and Consent Scenarios
Communication skills — like procedural skills — are built through deliberate practice, not through reading alone. Research consistently shows that medical students who have practised breaking bad news in simulated role-play settings perform measurably better than those who have only studied it, and the benefit persists under the stress of real clinical encounters. The scenarios below provide structured practice frameworks that you should complete during your paediatric clinical posting, ideally with a faculty observer who provides structured feedback.
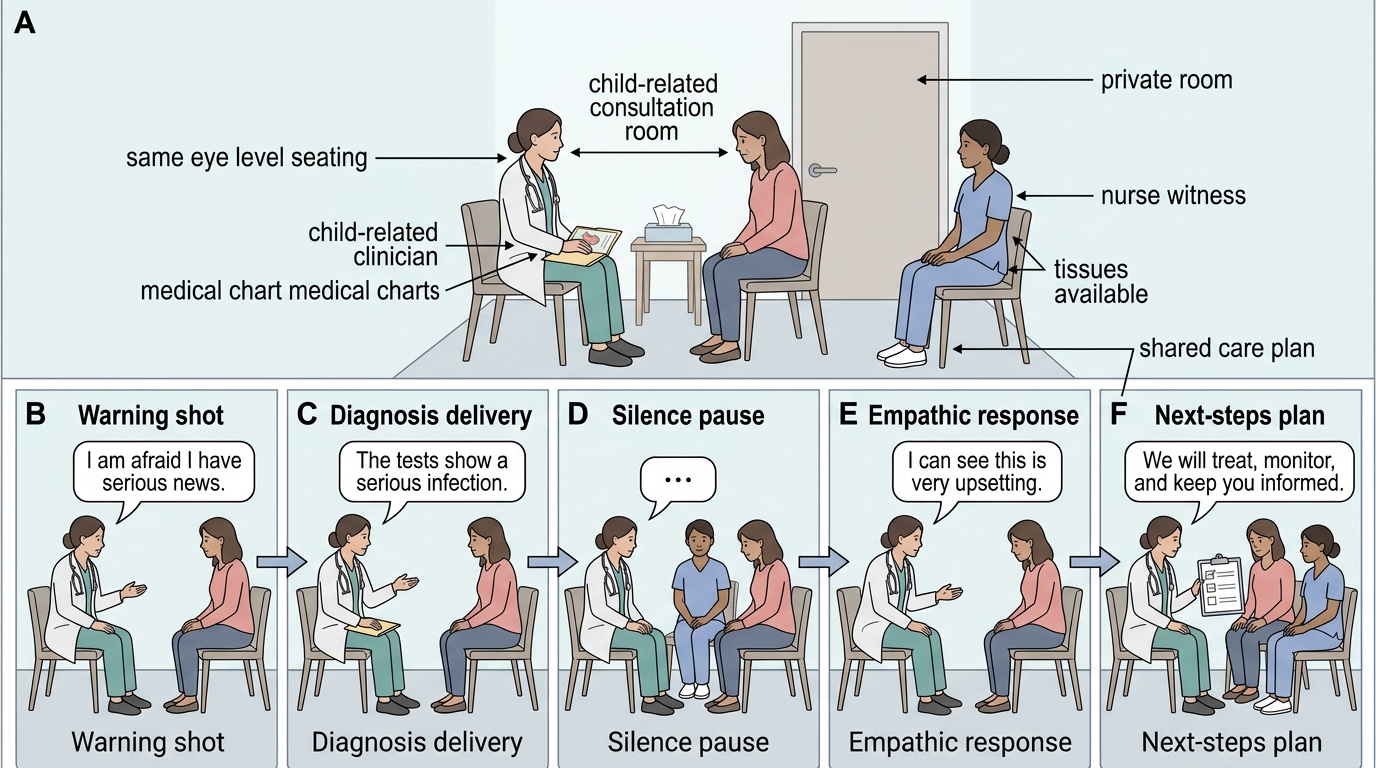
Scenario A — Breaking bad news: critical diagnosis:
Setting: parent waiting room, 3 AM. Your patient is a 7-year-old with bacterial meningitis and a falling GCS. The mother has just arrived. Role-play delivering the diagnosis using SPIKES. Key learning points: use a warning shot before the diagnosis; sit down; use plain language; pause after 'Your child has a very serious infection in the brain'; respond to the emotion before providing the management plan.
Scenario B — Emergency consent for lumbar puncture:
Setting: father present, child with suspected meningitis needs urgent LP. Role-play obtaining consent: identify yourself; explain what LP is and why it is needed now; state the main risk (post-LP headache, very rare infection); state the risk of NOT doing it (unable to confirm diagnosis or identify the organism for antibiotic selection); check understanding; obtain verbal consent and document in notes. Practice stating the time, who was present, what was explained, and the parent's response.
Scenario C — Responding to parental refusal:
Setting: parents of a 2-year-old with critical anaemia refuse blood transfusion on religious grounds. Practice: acknowledge the belief respectfully; explore the specific concern; provide additional medical information; escalate to senior colleague; document the refusal; outline the legal pathway (ethics committee/court order); describe the emergency exception if life is immediately at risk.
Scenario D — Communicating death:
This is the most demanding communication task in paediatrics. Practice the structure: private room, sit down, do not lead with 'I'm sorry to tell you'; say clearly 'We did everything we could, but I'm afraid we could not save your child — your child has died'; pause; respond to the emotion; offer practical next steps (seeing the child, calling family members, support services). The words matter less than the clarity, the presence, and the silence.
Consent documentation template (minimum elements):
Date and time / Patient name and age / Parent/guardian name and relationship / Procedure or treatment / Clinical indication explained / Main risks disclosed / Alternatives discussed / Consequence of refusal explained / Parent's understanding checked (how?) / Parent's response and explicit agreement / Clinician name and signature / Witness if applicable
SPIKES Bad-News Conversation Role-Play