Page 4 of 31
PE24.{2,6-11} | Respiratory Distress Emergency — SDL Guide
Learning Objectives
- Describe the aetio-pathogenesis and clinical recognition of respiratory distress in children
- Identify IMNCI danger signs and the triangle of assessment features indicating severe respiratory distress
- Explain the indications for and technique of oxygen therapy in paediatric emergencies, including selection of delivery device and flow rate
- Demonstrate correct airway positioning for infants and children in respiratory distress
- Perform bag-valve-mask ventilation correctly in a simulated setting
- Interpret clinical and oximetric monitoring to assess response to oxygen therapy and identify deterioration
INSTRUCTIONS
Respiratory distress is the most common life-threatening emergency in paediatric practice and the most frequent precipitant of cardiorespiratory arrest in children. Prompt recognition — distinguishing compensated distress from decompensating respiratory failure — and the immediate institution of appropriate oxygen therapy and airway positioning are skills that every final-year student must master before their paediatric posting. This module covers the recognition, pathophysiology, oxygen therapy technique, airway positioning, and bag-valve-mask ventilation required to manage a child in acute respiratory distress.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 27 — Paediatric Emergencies (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 77 — Respiratory Distress and Failure (textbook)
- WHO IMNCI Chart Booklet — Assess and Classify the Sick Child (guideline)
- IAP Guidelines on Oxygen Therapy in Paediatric Practice (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-month-old child is brought to the emergency department by her mother. The child is visibly distressed — breathing rapidly with visible subcostal and intercostal retractions, nasal flaring, and grunting with each expiration. Her lips are dusky. SpO₂ is 84% on room air. She is not crying — she is silent and limp in her mother's arms. You are the first doctor to see her. What is your immediate assessment, and what do you reach for first?
WHY THIS MATTERS
Acute respiratory distress is the leading cause of paediatric emergency presentations worldwide and is the most common pathway to cardiorespiratory arrest in children. The window between compensated respiratory distress and irreversible respiratory failure can be as short as minutes, particularly in infants whose respiratory muscles fatigue rapidly. Timely recognition of severity, immediate oxygen delivery, correct airway positioning, and bag-valve-mask ventilation when needed are the four skills that save lives before any advanced intervention arrives. These competencies are directly assessed in MBBS OSCEs, postgraduate entrance examinations, and are among the first skills expected of an intern in a paediatric ward or emergency room — particularly at primary and secondary health facilities in India where a senior paediatrician may not be immediately available.
RECALL
Before proceeding, recall the following:
• Normal respiratory rates by age (approximate): newborn/infant 30–60/min; 1–5 years 24–40/min; 5–12 years 18–30/min; >12 years 12–20/min. Tachypnoea is the earliest and most sensitive sign of respiratory distress.
• Gas exchange: oxygen crosses the alveolar-capillary membrane by passive diffusion down a concentration gradient; increasing FiO₂ drives more oxygen into the blood. Supplemental oxygen primarily corrects ventilation-perfusion mismatch; it does not correct hypoventilation (CO₂ retention) — that requires ventilation.
• Airway anatomy: the infant larynx is at C3-4 (higher than adult C4-5); the tongue fills the oral cavity proportionally; the cricoid ring is the narrowest point in the child's airway.
• IMNCI classification: WHO/Government of India IMNCI classifies children 2 months–5 years for respiratory conditions as: no pneumonia (fast breathing only), pneumonia (fast breathing + chest indrawing), and severe pneumonia/very severe disease (danger signs present — cannot drink, convulsions, unconscious, stridor at rest, central cyanosis, severe chest indrawing with grunting).
Clinical Indication: Recognising Respiratory Distress in Children
Respiratory distress is the physiological state in which increased work of breathing is required to maintain adequate gas exchange. It manifests as a spectrum from mild compensated distress (tachypnoea alone) through progressive decompensation (accessory muscle use, intercostal retractions, grunting) to respiratory failure (inadequate gas exchange despite maximal effort) and arrest (absent effort). The crucial clinical task is to identify children who have moved, or are moving, beyond the compensated phase — because respiratory failure and arrest can follow within minutes. Critically, the aetiological cause of respiratory distress cannot be treated without first stabilising the child: all immediate management steps — oxygen, positioning, BVM ventilation — are temporising measures applied simultaneously while the cause is being sought and treated. This 'treat the physiology first, identify the cause second' principle underpins all paediatric emergency management.
The aetiology of respiratory distress in children is classified by anatomical level:
• Upper airway: croup (laryngotracheobronchitis — inspiratory stridor, barking cough, commonest in 6 months–3 years), epiglottitis (bacterial, dramatic onset, 'muffled voice', drooling, tripod position — decreased since Hib vaccination), foreign-body aspiration (sudden onset choking, often unilateral wheeze or absent breath sounds)
• Lower airway: bronchiolitis (viral, infants <2 years, wheeze + prolonged expiration), asthma (recurrent wheeze in older children, reversible obstruction), pertussis (paroxysmal cough with inspiratory whoop)
• Parenchymal: pneumonia (bacterial or viral, fever + fast breathing + crepitations), pleural effusion / empyema (dullness to percussion, reduced breath sounds)
• Non-pulmonary causes must not be missed: congestive cardiac failure (basal crepitations, cardiomegaly, hepatomegaly), severe anaemia (pallor + tachypnoea without wheeze), metabolic acidosis (Kussmaul breathing — deep sighing respirations in DKA or renal failure), neuromuscular weakness
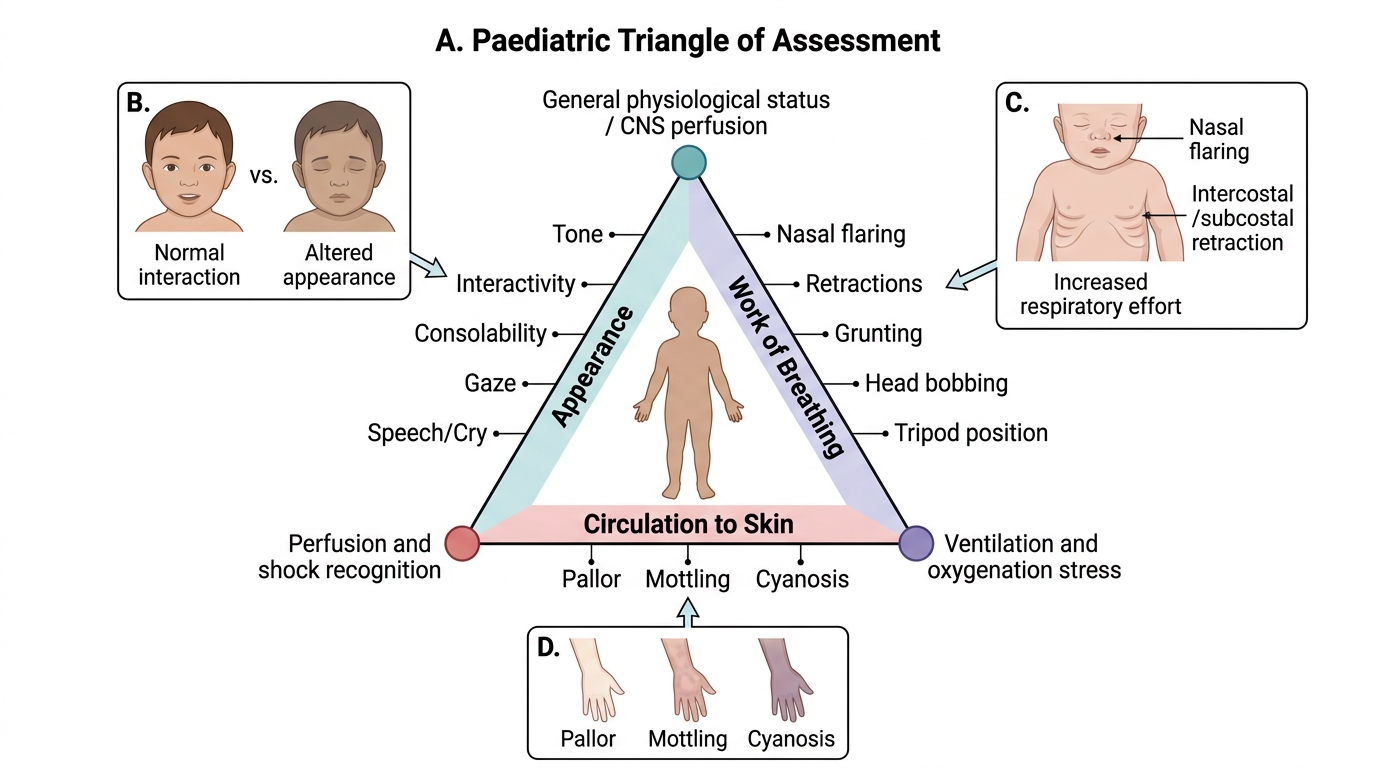
The triangle of assessment is the most rapid clinical screening tool for severity and requires only 30 seconds of visual observation — no equipment needed:
• Appearance (A): is the child alert, interactive, and consolable, or limp, hypotonic, and unresponsive? Abnormal appearance indicates a severely compromised child.
• Work of breathing (W): look for nasal flaring, intercostal and subcostal retractions, suprasternal retractions, use of accessory muscles (sternomastoid), grunting (auto-PEEP — signifies severe distress), head bobbing (infants — sternomastoid contracts with each breath), see-saw breathing (paradoxical abdominal and chest movement — signifies impending failure), tripod position (older children)
• Circulation to skin (C): central cyanosis (bluish perioral skin, tongue) indicates SpO₂ <85% and is a late and ominous sign; pallor and mottling may indicate reduced perfusion
IMNCI danger signs requiring immediate action: central cyanosis, severe chest indrawing, grunting at rest, inability to drink/breastfeed, stridor at rest, altered consciousness, convulsions.
Paediatric Triangle of Assessment
Anatomy and Pathophysiology of Paediatric Respiratory Failure
The paediatric respiratory system has several anatomical features that make children disproportionately vulnerable to respiratory failure. The chest wall is highly compliant in infants and young children — the ribs are horizontal (not slanted as in adults), the intercostal muscles are immature, and the diaphragm is the primary muscle of respiration. This compliance means that when airway resistance increases (bronchospasm, secretions, oedema), the infant produces greater negative intrathoracic pressure during inspiration — causing the chest wall to draw inward (retractions) rather than expanding the lungs. The visible retractions are therefore both a sign of increased work of breathing AND evidence that tidal volume is being partly wasted on paradoxical chest-wall movement. This is why infants tire so quickly — they are working inefficiently.
The functional residual capacity (FRC) is proportionally lower in infants than in adults, and the closing capacity (the lung volume at which small airways begin to collapse) may exceed FRC during tidal breathing in infants. This means infants spend part of each normal breath below their closing capacity, causing cyclical airway closure and ventilation-perfusion (V/Q) mismatch even at baseline. Any respiratory illness that further reduces FRC (e.g., pneumonia causing alveolar consolidation, bronchiolitis causing airway oedema and mucus plugging) pushes infants into worsening V/Q mismatch rapidly.
The pathophysiological sequence of paediatric respiratory failure follows a predictable trajectory:
1. Increased respiratory drive (tachypnoea, nasal flaring) — hypoxia and hypercapnia stimulate the respiratory centres; work of breathing increases
2. Compensated distress — accessory muscle use, retractions, grunting; gas exchange is still maintained; SpO₂ may be normal or mildly reduced
3. Decompensation — respiratory muscle fatigue develops; tidal volume falls; SpO₂ drops below 94%; CO₂ retention begins
4. Respiratory failure — severe hypoxaemia (SpO₂ <85%), hypercapnia (PaCO₂ rising); altered consciousness, reduced respiratory effort, paradoxical breathing
5. Respiratory arrest → cardiac arrest — apnoea → profound hypoxia → bradycardia → cardiac arrest
The clinical sign that most reliably marks the transition from compensated to decompensated distress is the loss of normal appearance — the child who was fighting and distressed becomes quiet and limp. This 'quiet child' is not improving; they are exhausted and approaching arrest.
Understanding this trajectory determines the urgency of intervention: a child with SpO₂ of 94-96% and mild retractions requires oxygen and monitoring; a child with SpO₂ <90%, severe retractions, grunting, and abnormal appearance requires immediate oxygen at maximum flow, airway positioning, and preparation for BVM ventilation.
Oxygen Therapy: Modalities and Technique
Supplemental oxygen is the most important immediate intervention for a child in respiratory distress. The therapeutic goal is to correct hypoxaemia and maintain SpO₂ at or above 94% (WHO and IAP guidance for paediatric respiratory emergencies). The choice of oxygen delivery device is determined by the severity of distress and the FiO₂ required. Choosing the wrong device — either too low a flow rate for a severely hypoxaemic child, or unnecessarily high FiO₂ in a stable child — both have adverse consequences. Excessive oxygen in preterm neonates causes retinopathy of prematurity; prolonged hyperoxia in post-resuscitation states worsens cerebral injury; insufficient oxygen prolongs hypoxaemia and risks progression to arrest.
Provided image
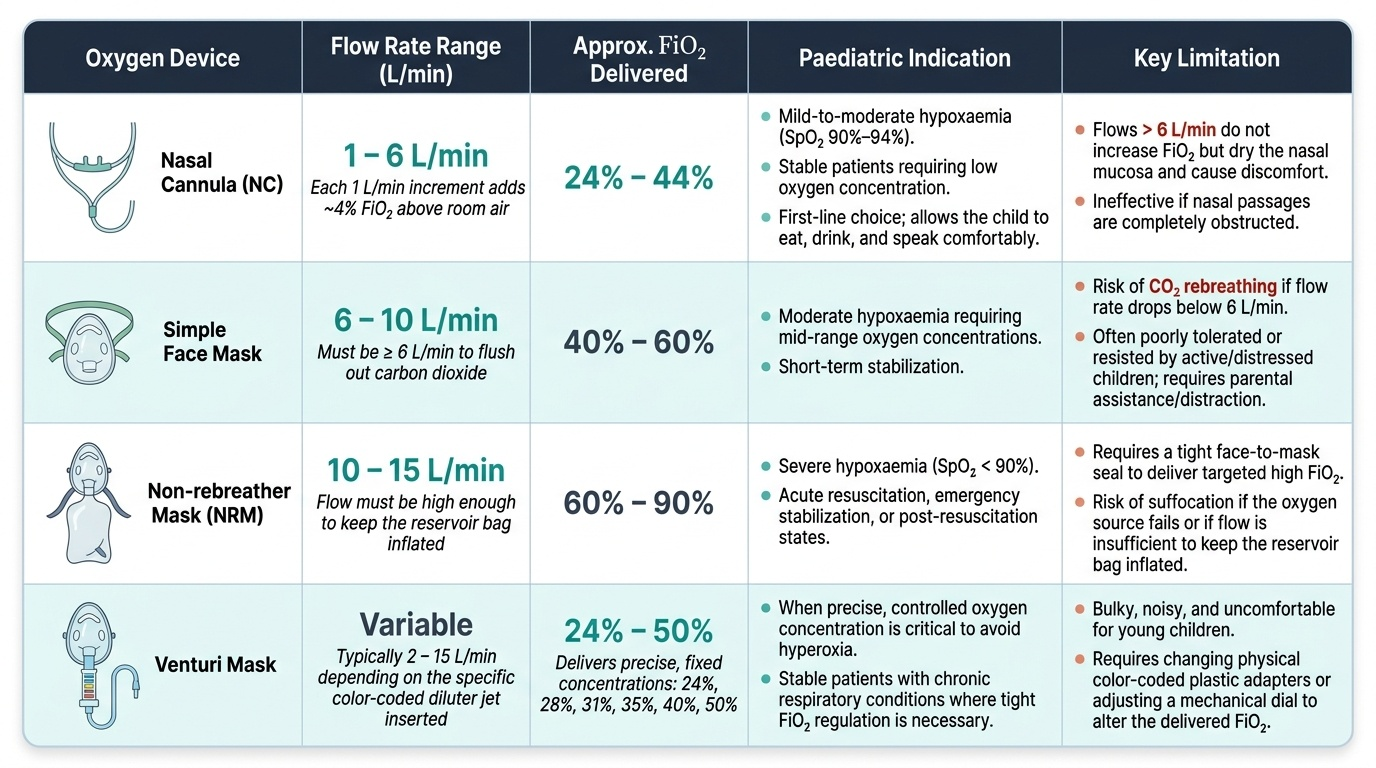
Oxygen delivery devices — a practical hierarchy from low to high FiO₂:
Nasal cannula (NC): delivers 24–44% FiO₂ at flow rates of 1–6 L/min (each 1 L/min increment adds approximately 4% FiO₂ above room air's 21%). The maximum effective flow rate is 6 L/min in children (higher rates are wasteful and dry the mucosa). Nasal cannulae are comfortable, allow the child to eat and speak, and are preferred for stable patients with mild-to-moderate hypoxaemia (SpO₂ 90–94%).
Simple face mask: delivers approximately 40–60% FiO₂ at 6–10 L/min. Must be used at ≥6 L/min to avoid CO₂ rebreathing (the minimum flow to flush the mask). Appropriate for moderate hypoxaemia. Children often resist masks; distraction and parent assistance improve tolerance.
Non-rebreather mask (NRM): delivers 60–90% FiO₂ at 10–15 L/min by combining a reservoir bag with a one-way valve that prevents exhaled air from re-entering the bag. Used for severe hypoxaemia (SpO₂ <90%). The reservoir bag must remain inflated at all times (if it collapses during inspiration, the flow rate is too low).
Venturi mask: the only device that delivers a fixed, reliable FiO₂ regardless of the patient's breathing pattern, by the Venturi principle (high-velocity jet of oxygen entrains room air in a fixed ratio). Available concentrations: 24%, 28%, 31%, 35%, 40%, 60%. Essential when precise FiO₂ control is required (e.g., hypercapnic respiratory failure where excessive oxygen may suppress respiratory drive).
High-flow nasal cannula (HFNC) / CPAP: used in severe respiratory distress not responding to conventional oxygen; delivers heated humidified oxygen at flows up to 2 L/kg/min, generating modest positive pressure (CPAP) that recruits atelectatic alveoli and reduces work of breathing. Requires specialised equipment; primarily used in PICU settings.
Technique of oxygen administration to a child:
• Explain the procedure to the parent; use distraction (toy, phone screen) to improve child's tolerance
• For nasal cannula: prongs curve downward into nares; secure tubing with tape to cheeks to prevent dislodgement
• For masks: select correct size (covers nose and mouth without pressing on eyes or overhanging chin); hold firmly but gently, or secure with elastic headband
• Reassess SpO₂ within 5 minutes of starting oxygen; titrate flow rate up or escalate device if SpO₂ does not reach ≥94%
• Do NOT remove oxygen to 'check' unless SpO₂ is stable ≥96% on low flow for ≥15 minutes
SELF-CHECK
A 2-year-old with severe bronchiolitis has SpO₂ of 88% on room air, with severe chest retractions and grunting. Which oxygen delivery device should you choose first?
A. Nasal cannula at 2 L/min
B. Simple face mask at 4 L/min
C. Non-rebreather mask at 10-15 L/min
D. Venturi mask at 24% FiO₂
Reveal Answer
Answer: C. Non-rebreather mask at 10-15 L/min
SpO₂ of 88% represents severe hypoxaemia requiring the highest immediately available non-invasive FiO₂. A non-rebreather mask at 10-15 L/min delivers 60-90% FiO₂ and is the correct first choice for a severely hypoxaemic child. Nasal cannula at 2 L/min delivers only ~29% FiO₂ — insufficient. Simple mask at 4 L/min is below the minimum safe flow (≥6 L/min required to prevent CO₂ rebreathing) and delivers inadequate FiO₂. A Venturi mask at 24% FiO₂ is barely above room air and is used for precise FiO₂ control in hypercapnic states, not severe hypoxaemia.