Page 5 of 31
PE24.{2,6-11} | Respiratory Distress Emergency — SDL Guide (Part 2)
Airway Assessment and Positioning
Systematic airway and breathing assessment uses the structured look-listen-feel approach, performed in sequence over ≤10 seconds. This assessment must be performed BEFORE any intervention except calling for help, because the findings determine the intervention: a child who is breathing adequately but hypoxaemic needs oxygen; a child who is not breathing needs airway opening and BVM ventilation.
Provided image
Look: respiratory rate (count for 30 seconds, multiply by 2 — in a distressed infant, count carefully as rate may be irregular); chest shape and symmetry; chest wall movement (equal bilaterally?); retractions (intercostal, subcostal, supraclavicular, suprasternal — each additional site indicates increasing severity); use of accessory muscles; see-saw or paradoxical movement (abdominal protrusion when chest collapses on inspiration = severe distress or airway obstruction).
Listen: stridor (inspiratory = supraglottic/glottic obstruction; biphasic = subglottic/tracheal; expiratory = lower airway); wheeze (expiratory predominant, lower airway obstruction); grunting (partially closed glottis against which the child expires to maintain PEEP and prevent alveolar collapse); absent breath sounds (complete obstruction, massive effusion, or consolidation).
Feel: trachea (midline or deviated — tension pneumothorax deviation away from the side of collapse); chest expansion (equal or reduced on one side); subcutaneous emphysema (crepitus on palpation — pneumothorax or pneumomediastinum).
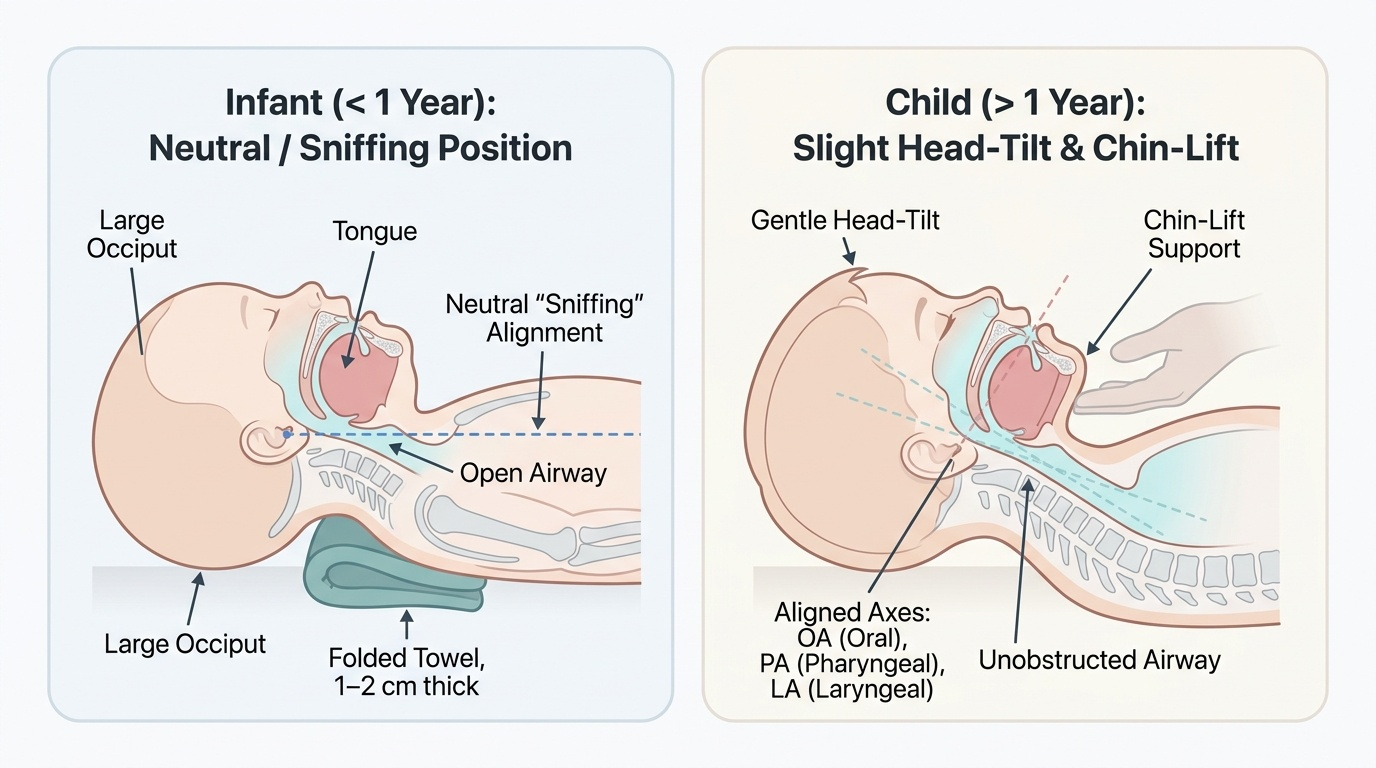
Airway positioning — the single most important, zero-cost, immediately available intervention:
Infants (<1 year — sniffing/neutral position): the large occiput causes passive neck flexion when the infant lies flat, pushing the tongue against the posterior pharynx. Correct this by placing a folded towel (1-2 cm thick) under the infant's shoulders — this brings the head to a neutral 'sniffing' position where the external auditory meatus is in line with the sternal notch when viewed from the side. Do NOT hyperextend the neck in infants — this narrows the trachea.
Children (>1 year — slight head-tilt): the sniffing position is modified to a gentle head-tilt (less extreme than adult head-tilt) to align the oral, pharyngeal, and laryngeal axes. Support the chin with chin-lift to prevent the tongue falling back.
Jaw thrust (suspected cervical injury): both hands placed at the angles of the mandible, pushing it forward without moving the neck — effective airway opening while maintaining cervical spine alignment.
Lateral recovery position (conscious child, no cervical injury): for a drowsy child who is breathing spontaneously but at risk of aspiration — position on the side with the dependent arm extended forward.
Bag-Valve-Mask Assisted Ventilation
Bag-valve-mask (BVM) ventilation is the most important resuscitation skill in paediatric emergency care. It is indicated when a child has inadequate spontaneous ventilation despite oxygen therapy and positioning — manifested by persistent severe hypoxaemia (SpO₂ <85% despite high-flow oxygen), apnoea, agonal breathing, or respiratory failure with altered consciousness. In the context of respiratory distress (not full arrest), BVM ventilation is used as a bridge to definitive airway management (intubation) while preparing the team and equipment.
The BVM device consists of three components: a self-inflating bag (250 mL for neonates/small infants; 500 mL for infants and young children; 1000 mL for older children and adults), a one-way valve that prevents exhaled air from re-entering the bag, and a transparent face mask with an inflatable rim for seal. An oxygen reservoir tail attached to the bag's inlet valve allows delivery of up to 90% FiO₂ when connected to oxygen at 10–15 L/min.
Mask size selection: the mask must cover the nose and mouth completely without extending over the eyes or below the chin point. Too small a mask leaks air at the chin; too large a mask compresses the eyes and risks corneal abrasion. In infants, a circular (round) mask is preferred; in children, a triangular anatomical mask.
The E-C grip (two-handed technique, one rescuer holds mask, second rescuer squeezes bag): the non-dominant hand forms an 'E' with three fingers (ring, middle, and index) along the bony part of the mandible to perform chin-lift; the thumb and forefinger form a 'C' over the mask to maintain a seal between mask edge and face. The key principle is to lift the face INTO the mask, not press the mask onto the face — pressing compresses the soft submandibular tissues, worsening obstruction.
Ventilation parameters for non-arrest assisted ventilation (child in respiratory failure, not yet arrested):
• Rate: 20 breaths/min for infants and small children; 15 breaths/min for children — slower than CPR ventilation because these children have spontaneous respiratory effort and are not in arrest
• Volume: squeeze the bag until the chest visibly rises — do NOT use full-bag compression; over-inflation causes gastric inflation, regurgitation, and reduces venous return
• Inspiratory time: approximately 1 second
• Oxygen flow: 10–15 L/min through the reservoir tail for maximum FiO₂
Common BVM errors that reduce effectiveness:
• Inadequate mask seal (most common): air leaks at the lateral mask edge when the mask is pressed instead of the face being lifted
• Head position not optimised: BVM ventilation without first positioning the airway is ineffective
• Over-ventilation: excessive rate or volume causes gastric inflation; consider orogastric tube decompression if BVM is prolonged
• Bag squeezed too forcefully: high-pressure ventilation causes barotrauma and bypasses the one-way valve
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
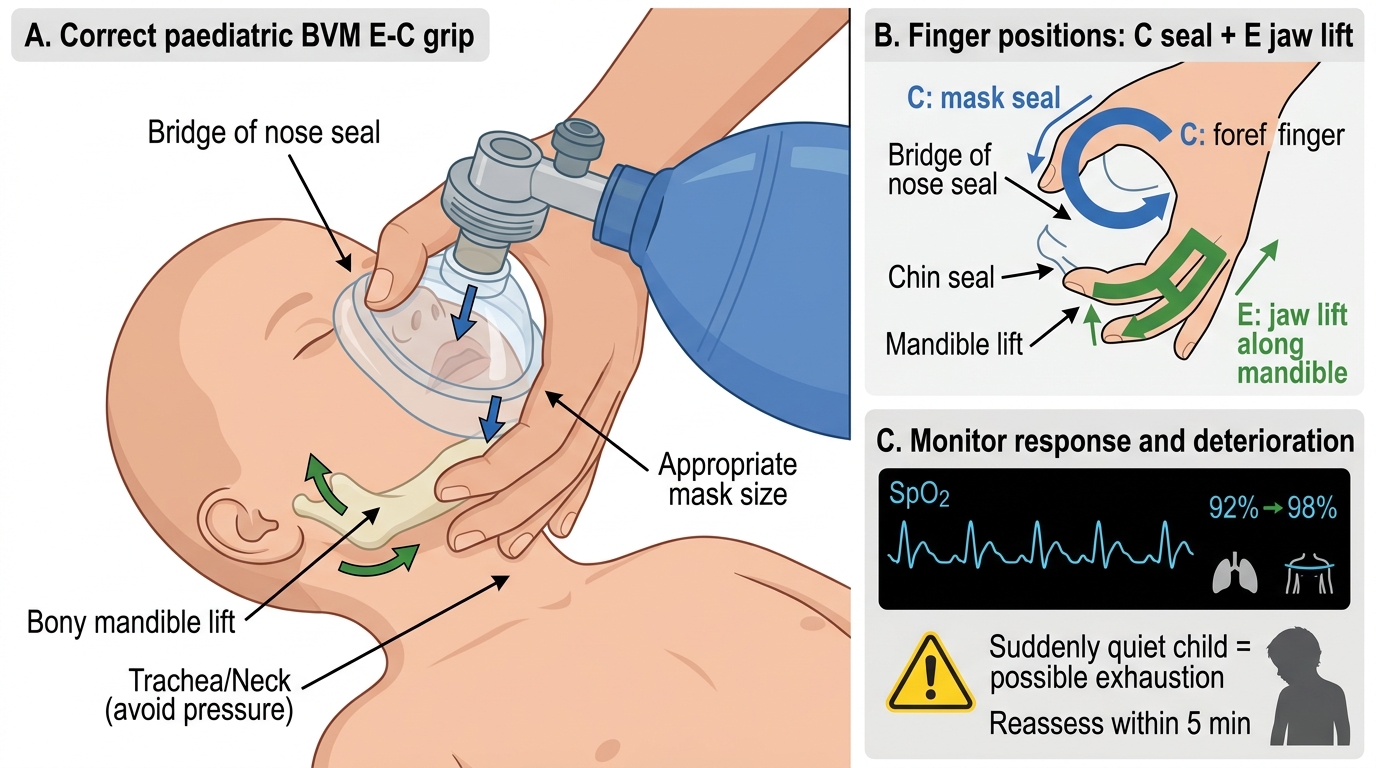
Paediatric BVM E-C Grip Technique
CLINICAL PEARL
The 'quiet child' is not a recovering child. A severely distressed child who becomes suddenly quiet and stops fighting is not improving — they are exhausted and approaching respiratory arrest. The loss of audible grunting (which was auto-PEEP maintaining FRC) is an ominous sign of decompensation. Escalate immediately: switch to BVM, call the paediatric team, and prepare for intubation.
Grunting is a PEEP manoeuvre. When a child grunts against a partially closed glottis during expiration, they are generating end-expiratory pressure to prevent alveolar collapse (the same physiology as clinical PEEP on a ventilator). Do NOT try to suppress grunting — it is a life-preserving response. If you apply oxygen via a mask and the child's grunting stops because they have improved, that is good. If grunting stops because the child is too tired to grunt, that is bad — look at the full triangle of assessment.
Interpretation: Monitoring Response to Oxygen and Ventilation
After initiating oxygen therapy or BVM ventilation, structured re-assessment within 5 minutes is essential to determine whether the child is improving, stable, or deteriorating. Monitoring combines continuous pulse oximetry with serial clinical observations. Pulse oximetry is a non-invasive, real-time measure of haemoglobin oxygen saturation (SpO₂) and is the single most valuable monitoring tool in paediatric respiratory distress. However, it has important limitations that the clinician must understand: SpO₂ readings are unreliable when the perfusion waveform is poor (shock, hypothermia, severe peripheral vasoconstriction), SpO₂ does not measure CO₂ (a child can be hyperoxic and hypercapnic simultaneously), and SpO₂ may remain falsely reassuring during early CO₂ retention if the child is breathing supplemental oxygen. For this reason, clinical assessment — respiratory rate, effort, appearance, and skin colour — must always accompany SpO₂ monitoring and must not be replaced by it.
Indicators of improvement (reassuring response to oxygen):
• SpO₂ rising toward ≥94% within 5 minutes
• Respiratory rate decreasing toward normal for age
• Retractions becoming less marked
• Child becoming more alert and interactive (improved appearance)
• Grunting reducing because alveolar recruitment has been achieved
• Colour improving from cyanosed/mottled toward pink
Indicators of deterioration or non-response (requiring escalation):
• SpO₂ not reaching ≥90% despite non-rebreather mask at 15 L/min
• Increasing tachypnoea or slowing respiratory rate with loss of effort (exhaustion)
• Worsening retractions or development of see-saw breathing
• Deteriorating appearance (child becoming limp, unresponsive)
• Bradycardia (HR <100/min in infants, <60/min in any child) — signifies severe hypoxia and is a preterminal sign
Escalation ladder based on response:
1. Room air → nasal cannula (1-2 L/min) → increase to 6 L/min
2. Nasal cannula → simple face mask (6-10 L/min)
3. Simple face mask → non-rebreather mask (10-15 L/min)
4. Non-rebreather mask without improvement → BVM-assisted ventilation + call for senior/PICU support
5. BVM failing or sustained respiratory failure → intubation and mechanical ventilation
The decision to escalate from step 3 to 4 is one of the most critical judgements in paediatric emergency medicine. Key triggers: SpO₂ <90% despite maximal oxygen, rising respiratory rate despite oxygen, bradycardia, altered consciousness, or clinical signs of impending arrest (loss of grunting in a previously grunting child, see-saw breathing, fixed dilated pupils).
SELF-CHECK
A 10-month-old infant with bronchiolitis has been on a non-rebreather mask at 15 L/min for 10 minutes. SpO₂ remains 88%, respiratory rate is 72/min (increasing from 64/min), retractions are worsening, and the infant is becoming limp. What is the most appropriate next step?
A. Increase the non-rebreather mask flow to 20 L/min
B. Switch to a Venturi mask at 40% FiO₂
C. Begin bag-valve-mask assisted ventilation and call for PICU support
D. Administer salbutamol nebulisation and reassess in 20 minutes
Reveal Answer
Answer: C. Begin bag-valve-mask assisted ventilation and call for PICU support
This infant is showing signs of decompensation despite maximal non-invasive oxygen: SpO₂ still <90%, worsening tachypnoea (increasing, not decreasing), worsening retractions, and deteriorating appearance (limp infant). This is the escalation trigger for BVM ventilation. Non-rebreather masks cannot go beyond 15 L/min effectively (already at maximum). A Venturi mask at 40% delivers less FiO₂ than the current NRB — this is a step backward. Salbutamol nebulisation takes 10-15 minutes to act and is not the primary treatment for bronchiolitis; this infant is in impending respiratory arrest and needs immediate ventilatory support.