Page 18 of 31
PE24.16 | Severe Dehydration — SDL Guide
Learning Objectives
- Assess a child for signs of dehydration using the IMNCI framework (skin pinch, sunken eyes, drinking ability, level of consciousness)
- Classify dehydration severity as no dehydration, some dehydration, or severe dehydration
- Select and calculate the appropriate treatment plan (A, B, or C) based on dehydration classification
- Calculate Plan C fluid volumes (Ringer's lactate 100 mL/kg) with correct age-based phase timing for infants and children
INSTRUCTIONS
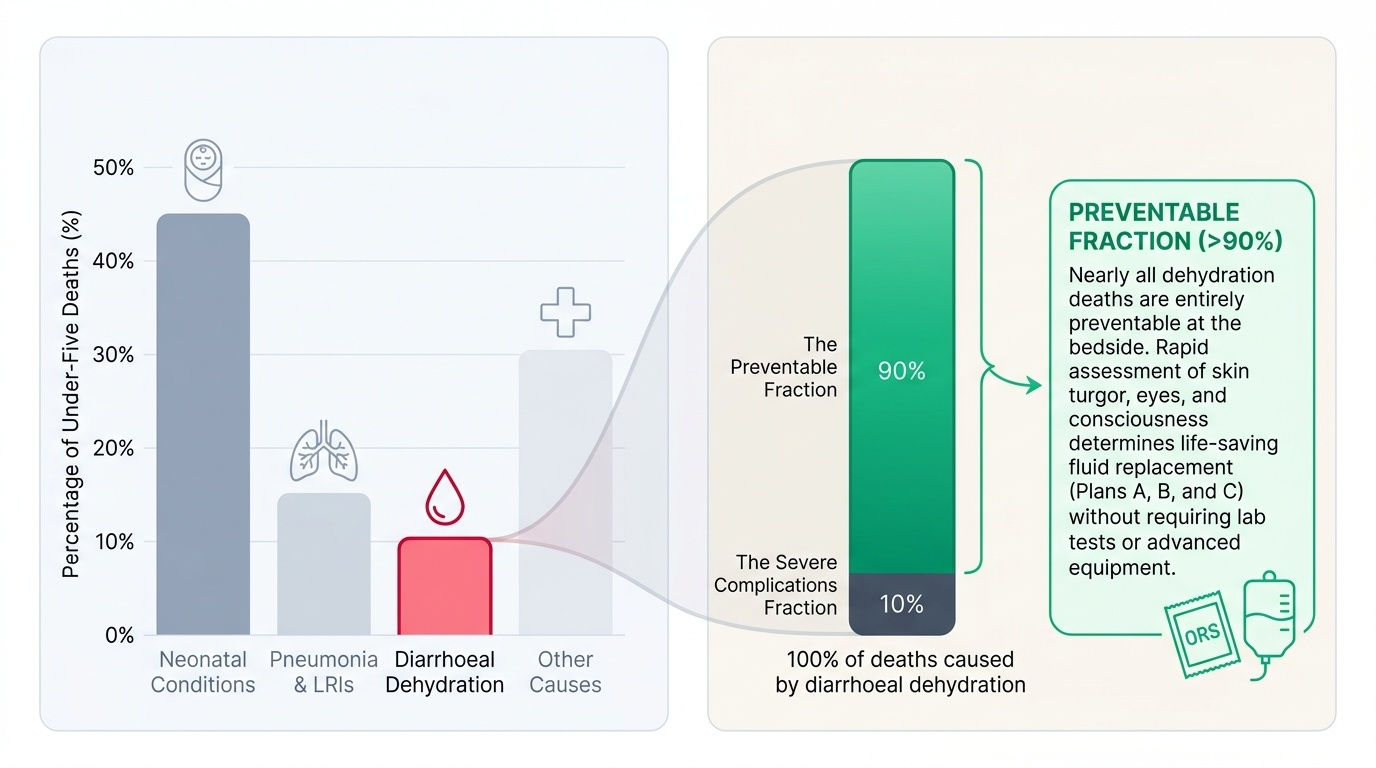
Diarrhoeal disease kills more children under five globally than almost any other cause, and the vast majority of those deaths are from dehydration that was either unrecognised or inadequately treated. The IMNCI dehydration assessment is a structured clinical skill that can be performed in under two minutes at the bedside and directly determines the treatment plan. This module teaches you to perform that assessment accurately and to translate findings into correct fluid management, including intravenous Plan C rehydration.
References
- Ghai Essential Pediatrics, 9th edition, Ch 16 (Diarrhoeal Diseases and Dehydration) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 55 (Dehydration and Fluid Therapy) (textbook)
- WHO IMNCI Chart Booklet — Assessment and Classification of the Sick Child (guideline)
- IAP Guidelines on Management of Diarrhoea in Children, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 10-month-old girl is brought to the OPD with 3 days of watery diarrhoea and 2 days of vomiting. She has had 10 loose stools today. On examination her eyes look sunken, she is not feeding at the breast, and when you pinch the skin on her abdomen it goes back very slowly — more than 2 seconds. Her mother looks terrified. What classification does this child fall into, and what is your immediate treatment plan?
WHY THIS MATTERS
Diarrhoeal disease remains one of the leading causes of mortality in children under five in India, accounting for approximately 13% of all under-five deaths (NFHS/SRS data). The mechanism of death is almost universally dehydration — a preventable, treatable condition. The IMNCI assessment framework was designed precisely to detect dehydration severity at the point of first contact, whether in a primary health centre or a district hospital, and to match the child's fluid needs to the right treatment plan without laboratory testing. A clinician who can classify dehydration accurately and calculate Plan C fluids correctly has the skill to save a child's life in any resource setting in India. Missing severe dehydration — or misclassifying it as 'some dehydration' — delays IV rehydration and risks hypovolaemic shock.
RECALL
Recall from your preclinical physiology:
• Body water distribution: Total body water is approximately 60% of body weight in older children, higher in neonates (75-80%). Approximately two-thirds is intracellular and one-third extracellular. Diarrhoeal loss is primarily isotonic — it depletes the extracellular compartment (plasma + interstitium) first.
• Holliday-Segar maintenance: 100 mL/kg/day for the first 10 kg, 50 mL/kg/day for the next 10 kg, 20 mL/kg/day for each kilogram above 20 kg. This is daily maintenance; dehydration replacement is additional.
• Reduced-osmolarity ORS: The WHO-recommended ORS has osmolarity 245 mOsm/L (sodium 75, chloride 65, glucose 75, potassium 20, trisodium citrate 10 mmol/L). Its reduced osmolarity versus the original formula reduces stool output and vomiting, and is the current standard.
• Ringer's lactate (RL): The preferred IV fluid for dehydration replacement in IMNCI Plan C — isotonic, contains lactate as a bicarbonate precursor (counteracting metabolic acidosis from diarrhoea), and avoids the hyperchloraemic acidosis associated with large volumes of normal saline.
Clinical Indication: When and Why Dehydration Assessment Is an Emergency Skill
The ability to assess dehydration severity is one of the highest-yield clinical skills in paediatric practice in India because the assessment is rapid, requires no equipment, directly determines life-saving treatment, and is performed by clinicians at every level of the health system — from community health workers using IMNCI algorithms to paediatricians in tertiary hospitals. Unlike most diagnostic skills where findings guide further investigation, the dehydration assessment immediately yields a treatment plan: classify → plan → execute.
Provided image
The epidemiological context in India makes this skill especially critical. Diarrhoea accounts for over 300,000 deaths per year in children under five globally, and India contributes a significant proportion of this burden. The majority of deaths occur not from the diarrhoeal pathogen itself but from the fluid deficit that accumulates when losses exceed intake and are not replaced. Children under two years are disproportionately affected because their total body water is larger relative to metabolic surface area, their renal concentrating capacity is immature, and they depend entirely on caregivers for fluid replacement.
The IMNCI framework operationalises this into a two-minute bedside assessment with four clinical signs — skin turgor (pinch test), eye appearance (sunken or not), drinking ability, and level of consciousness — that together classify the child into one of three severity groups, each with a prescribed treatment plan. The assessment requires no blood tests, no weighing scale for initial classification (though weight is needed for fluid calculation), and no imaging. It is designed to function in a PHC with a torch and a watch.
The clinical imperative is this: a child with severe dehydration is in, or approaching, hypovolaemic shock. Every minute of delay in initiating Plan C IV rehydration worsens perfusion to the kidneys, gut, and brain. Recognition within the first contact is therefore the primary goal, and this module teaches that recognition skill.
Physiology of Fluid Loss and the Dehydration Cascade
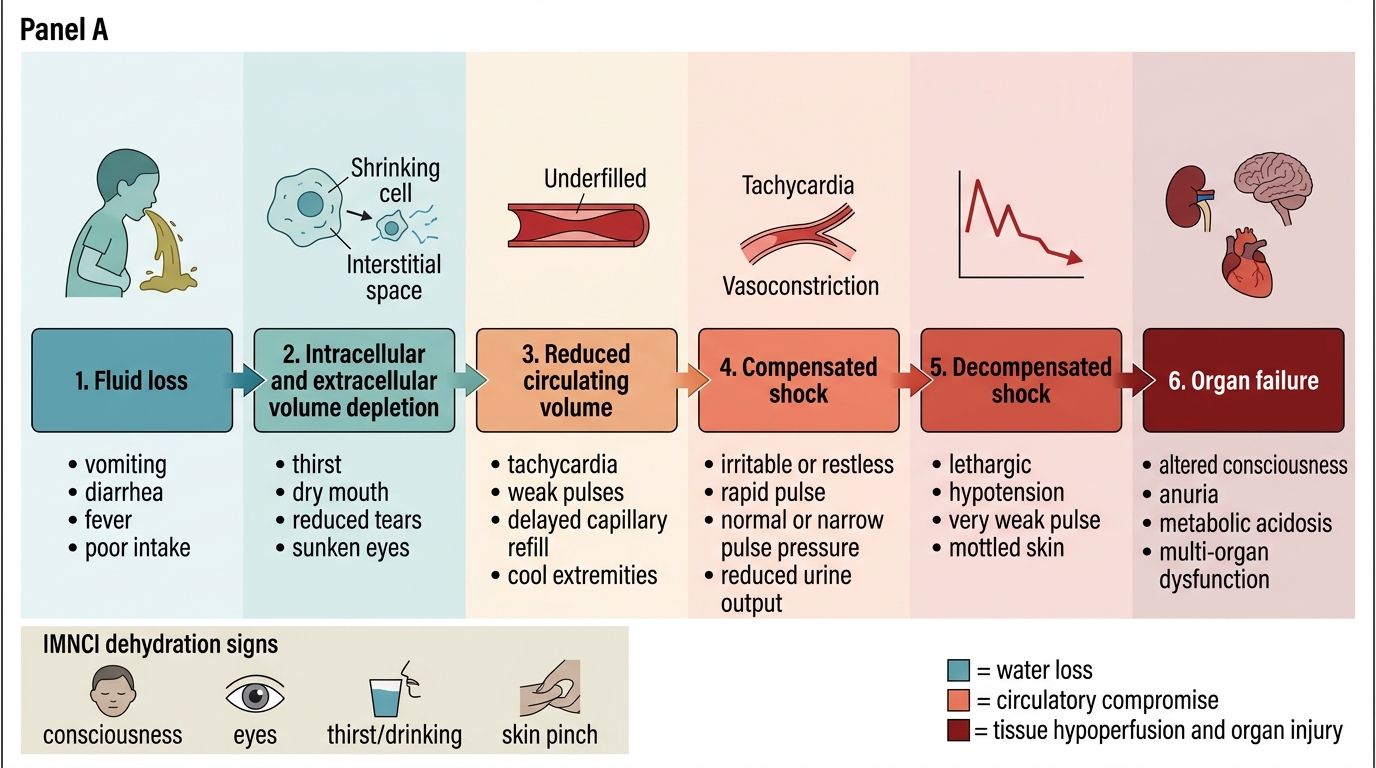
Understanding the physiology of dehydration allows the clinician to predict clinical signs at each stage of severity and to select the correct replacement fluid. The pathophysiology follows a predictable cascade from extracellular volume depletion through compensated shock to decompensated shock and ultimately organ failure — a sequence that in a young child can progress in hours.
In diarrhoeal illness, fluid loss is primarily isotonic: stool contains sodium at concentrations similar to plasma (though somewhat lower), along with bicarbonate, potassium, and water. The initial loss depletes the extracellular fluid (ECF) compartment — both the plasma and the interstitial fluid. As plasma volume falls, the compensatory response recruits three mechanisms: (1) activation of the renin-angiotensin-aldosterone system to retain sodium and water, increasing tubular reabsorption; (2) increased anti-diuretic hormone (ADH) release, concentrating the urine; and (3) redistribution of blood flow from skin and splanchnic vessels (vasoconstriction) to preserve perfusion of the brain, heart, and kidneys. These compensatory mechanisms explain why blood pressure is preserved even when 5–10% body weight is lost — a child can lose substantial volume before hypotension appears, because vasoconstriction maintains perfusion pressure. However, the peripheral signs (reduced skin turgor, tachycardia, prolonged capillary refill, cool extremities) precede hypotension and are the bedside indicators of early/compensated shock.
When losses exceed approximately 10–15% of body weight, compensatory mechanisms fail. Cardiac output falls, tissue perfusion becomes inadequate, metabolic acidosis develops from anaerobic metabolism, and organ dysfunction begins — first acute kidney injury (oliguria/anuria), then CNS depression (lethargy, unconsciousness), then cardiovascular collapse. At this stage the clinical signs of severe dehydration (sunken eyes, no skin recoil, unable to drink, lethargic/unconscious) reflect not just fluid deficit but impending circulatory failure.
Why Ringer's lactate (RL) is preferred over normal saline for Plan C: RL is isotonic, but contains lactate (28 mEq/L) which is metabolised to bicarbonate, partially correcting the metabolic acidosis that accompanies diarrhoeal dehydration. Normal saline (0.9% NaCl) provides no buffer and, in large volumes, causes hyperchloraemic metabolic acidosis, worsening the pre-existing acidosis. RL is therefore the WHO/IMNCI recommended fluid for Plan C IV rehydration.
Pathophysiology of Severe Dehydration in Children
IMNCI Assessment Technique: Signs of Dehydration and Classification
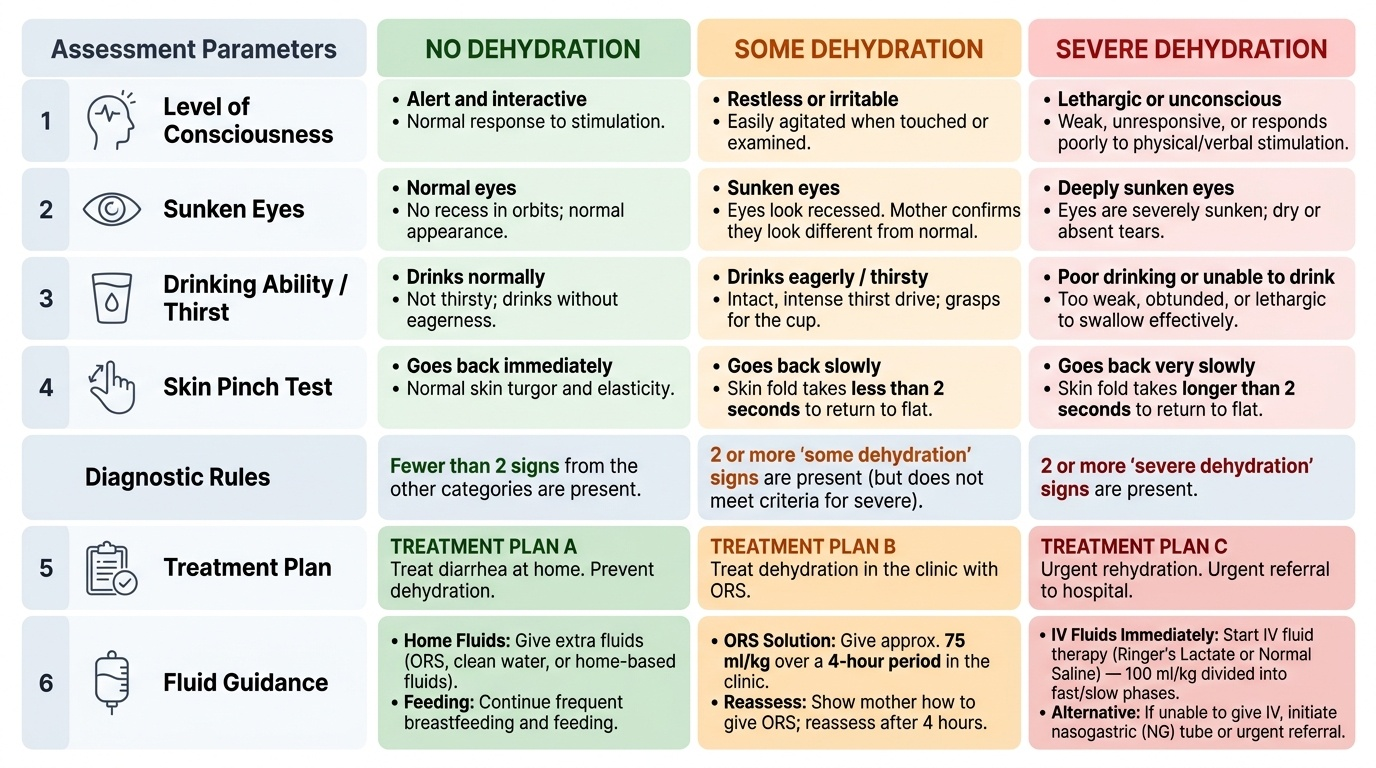
The IMNCI dehydration assessment comprises four clinical signs assessed in a specific sequence. The classification into no dehydration, some dehydration, or severe dehydration is based on the combination of findings. A child is classified as having severe dehydration if two or more severe-dehydration signs are present; some dehydration if two or more some-dehydration signs are present but not all severe; and no dehydration if fewer than two signs from either category are present. The sequential technique ensures reproducibility across different examiners at different levels of the health system.
Provided image
Sign 1 — Level of consciousness: Assess before touching the child, to avoid stimulating a response. Observe whether the child is alert and interactive, restless/irritable (a sign of 'some dehydration'), or lethargic/unconscious (a sign of 'severe dehydration'). A lethargic child responds poorly to stimulation; an unconscious child does not respond at all.
Sign 2 — Sunken eyes: Look directly at the child's face, at eye level. In dehydration, reduced orbital fat and decreased intra-ocular pressure cause the eyes to appear recessed in the orbits. Sunken eyes are present in both 'some dehydration' and 'severe dehydration'. Ask the mother whether the eyes look different from normal — she often notices this before the clinician.
Sign 3 — Drinking ability: Offer the child water or ORS in a cup. Classify as: 'drinks eagerly/thirsty' (some dehydration — the thirst drive is intact and intense); 'not able to drink or drinks poorly' (severe dehydration — the drive is present but the child is too weak or obtunded to drink effectively). A child who drinks normally and is not especially thirsty has no dehydration.
Sign 4 — Skin pinch (turgor test): Use two fingers (thumb and index) to pinch a fold of abdominal skin at the umbilical level, lifting it 1–2 cm and releasing sharply. Time the recoil:
• Immediate (< 1 second) → normal
• Slowly (1–2 seconds) → some dehydration
• Very slowly (> 2 seconds, fold persists) → severe dehydration
Technical notes: (1) The abdominal skin is the preferred site — avoid the dorsum of the hand, which gives falsely abnormal results in malnourished children due to reduced subcutaneous fat; (2) in severe acute malnutrition (SAM), skin pinch may be falsely slow even without dehydration because of protein depletion — rely more on drinking ability and consciousness in SAM; (3) in obese children, pinch may be falsely fast. Always interpret all four signs together.
SELF-CHECK
A 14-month-old child with diarrhoea is restless and irritable. His eyes appear sunken. He drinks eagerly from a cup but is not unconscious. The skin pinch recoils in 1.5 seconds. How is he classified?
A. No dehydration — reassure and send home with ORS advice
B. Some dehydration — supervised ORS (Plan B), 75 mL/kg over 4 hours
C. Severe dehydration — IV RL Plan C immediately
D. Some dehydration — admit and start IV maintenance fluids
Reveal Answer
Answer: B. Some dehydration — supervised ORS (Plan B), 75 mL/kg over 4 hours
He has two 'some dehydration' signs: restless/irritable + sunken eyes + drinks eagerly + skin pinch slow (1.5 sec). He has NO severe dehydration signs (not lethargic/unconscious; skin pinch not >2 sec; able to drink). Classification = some dehydration → Plan B: supervised ORS 75 mL/kg over 4 hours in health facility, reassess after 4 hours. IV fluids are not indicated at this stage.