Page 19 of 31
PE24.16 | Severe Dehydration — SDL Guide (Part 2)
Treatment Plans A, B and C: Matching Fluid Strategy to Severity
The IMNCI treatment plans translate the dehydration classification directly into a fluid management strategy. Each plan has a specific fluid, volume, route, and duration — and the child must be reassessed after the prescribed treatment to reclassify before the next plan is chosen. This iterative reassessment principle prevents both under-treatment (missing residual dehydration) and over-treatment (continuing IV fluids when the child has responded and can transition to oral rehydration).
Plan A — No dehydration (home management):
The caregiver is counselled to give ORS after each loose stool: 50–100 mL for a child under 2, 100–200 mL for a child 2–10 years, and as much as the child wants for older children. Continue breastfeeding or usual feeding. Signs to return immediately: three or more watery stools in one hour, repeated vomiting, marked thirst, sunken eyes, reduced urine, blood in stool.
Plan B — Some dehydration (supervised ORS, 4 hours in facility):
Administer reduced-osmolarity ORS 75 mL/kg over 4 hours in the health facility. The caregiver gives ORS by spoon or cup (not bottle) in small, frequent amounts to reduce vomiting. If the child vomits, wait 10 minutes then resume slowly. Reassess after 4 hours: if no signs of dehydration → Plan A; if some dehydration persists → repeat Plan B; if severe dehydration develops → Plan C.
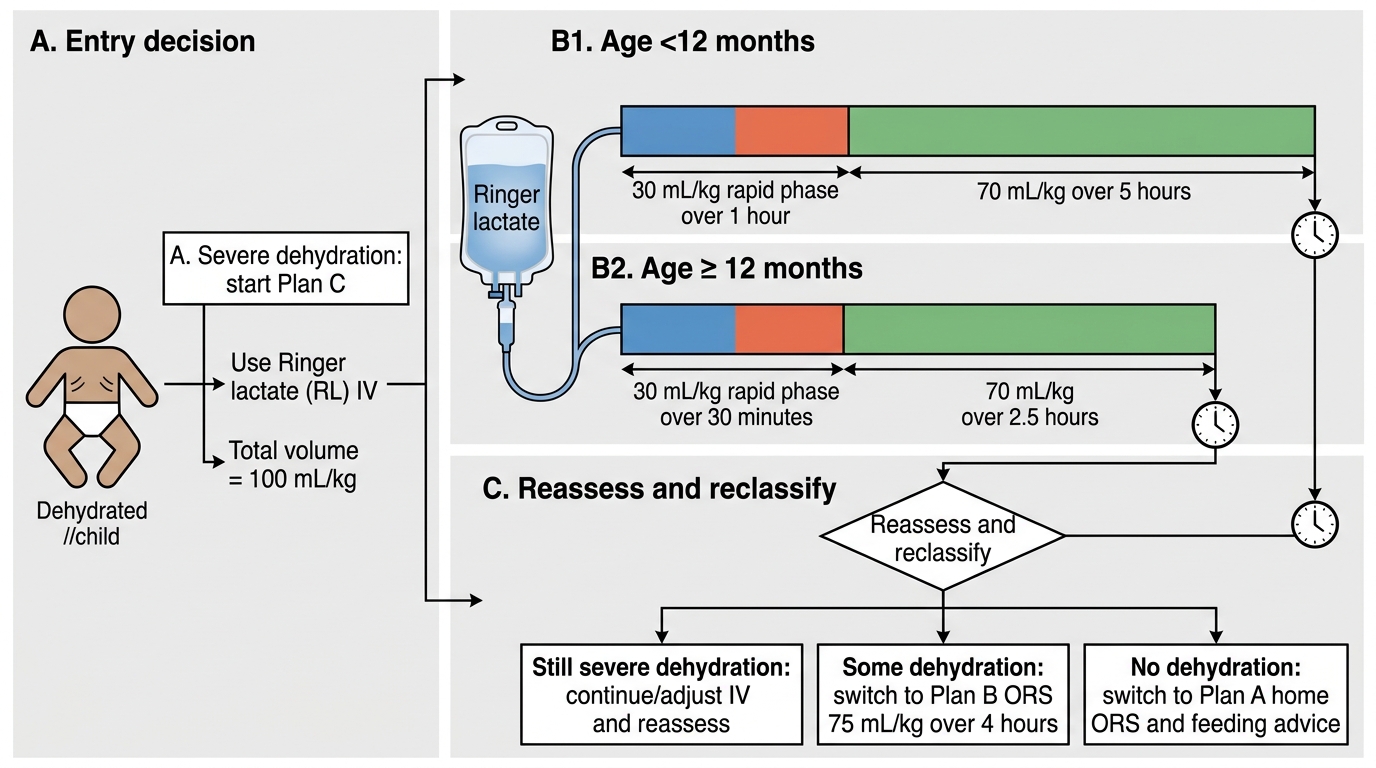
Plan C — Severe dehydration (IV rehydration with Ringer's lactate):
Administer RL 100 mL/kg IV in two phases:
Phase 1 (rapid/bolus phase — 30 mL/kg):
• Infants under 12 months: give 30 mL/kg over 1 hour
• Children 12 months and older: give 30 mL/kg over 30 minutes
Phase 2 (maintenance/replacement phase — 70 mL/kg):
• Infants under 12 months: give 70 mL/kg over 5 hours
• Children 12 months and older: give 70 mL/kg over 2.5 hours
Reassessment after Phase 1: If the child still has severe dehydration signs → repeat Phase 1 (30 mL/kg rapid infusion). If improved → proceed to Phase 2. If the child can drink → also begin ORS 5 mL/kg/hour alongside the IV.
Transition: When Phase 2 is complete and the child shows no dehydration signs → transition to Plan A ORS; if some dehydration remains → Plan B.
Special consideration — if IV not possible in severe dehydration:
If IV access cannot be established within 2 attempts, a nasogastric tube (NGT) route for ORS is acceptable for children who are not vomiting persistently: 20 mL/kg/hour ORS via NGT for 6 hours while arranging urgent transfer for IV access.
IMNCI Plan C IV Rehydration Algorithm
CLINICAL PEARL
The Plan C split is age-dependent — not weight-dependent. The timing changes at 12 months of age: infants get the rapid phase over 1 hour (slower, because their cardiovascular system is less tolerant of rapid volume loading), while children 12 months and older get it over 30 minutes. The volume (30 mL/kg rapid + 70 mL/kg maintenance) is the same for all ages — only the infusion rate differs. Getting this backwards — giving an infant the child's 30-minute rapid rate — risks pulmonary oedema. Getting it right is a calculation you will perform in emergencies; practise it now.
SELF-CHECK
An 8-month-old infant weighing 8 kg has severe dehydration. You are starting Plan C. What volume of RL will you give in Phase 1, and over what time period?
A. 30 mL/kg = 240 mL over 30 minutes (infant rate)
B. 30 mL/kg = 240 mL over 1 hour (infant rate)
C. 100 mL/kg = 800 mL over 1 hour
D. 70 mL/kg = 560 mL over 1 hour
Reveal Answer
Answer: B. 30 mL/kg = 240 mL over 1 hour (infant rate)
Phase 1 (rapid phase) = 30 mL/kg = 30 × 8 = 240 mL RL. For infants under 12 months, this is given over 1 hour (not 30 minutes — that is the rate for children ≥12 months). Total Plan C = 100 mL/kg = 800 mL; Phase 2 (70 mL/kg = 560 mL) is then given over 5 hours in an infant.
Interpreting Assessment Findings and Monitoring Response
Dehydration assessment is not a one-time event — it is a repeated clinical skill applied before, during, and after rehydration to guide ongoing treatment decisions. The ability to interpret the direction of change (improving vs deteriorating) is as important as the initial classification, because a child who started Plan C must be evaluated after Phase 1 to determine whether Phase 2 should continue or whether the rapid phase needs to be repeated.
Reassessment after Phase 1 of Plan C:
After 30 mL/kg RL has been infused over the prescribed time, reassess all four IMNCI signs. The expected response to successful Phase 1 is: level of consciousness improves (from lethargic toward alert/irritable), eyes become less sunken, skin pinch recoils faster, and the child is able to accept oral fluids. If these improvements are present → proceed to Phase 2. If severe dehydration signs persist → repeat Phase 1 (another 30 mL/kg over 1 hour for infants, 30 minutes for older children) and reassess urgently for complications (septic shock, severe acute malnutrition, severe anaemia).
Monitoring parameters during IV rehydration:
• Pulse rate and volume (should improve — tachycardia reduces as circulating volume is restored)
• Respiratory rate (should improve; worsening suggests fluid overload or metabolic acidosis not correcting)
• Level of consciousness (improving GCS/AVPU is the most reassuring sign)
• Urine output (should resume within 1–2 hours of starting Phase 1; oliguria persisting beyond 2 hours despite IV = possible pre-renal AKI or structural renal injury)
• Skin turgor and eye appearance (improve more slowly than pulse/consciousness)
Special situation — severe dehydration in a child with severe acute malnutrition (SAM):
Children with SAM (weight-for-height <−3 SD or MUAC <11.5 cm) who appear severely dehydrated must be treated with caution. In SAM, skin pinch is unreliable (depleted subcutaneous fat gives falsely prolonged recoil without true dehydration), and the heart cannot tolerate rapid fluid loading (risk of cardiac failure and pulmonary oedema). In SAM with suspected severe dehydration, use a slower IV rate (approximately 15 mL/kg over 1 hour) and reassess; do NOT give the standard Plan C rapid bolus without specialist guidance.
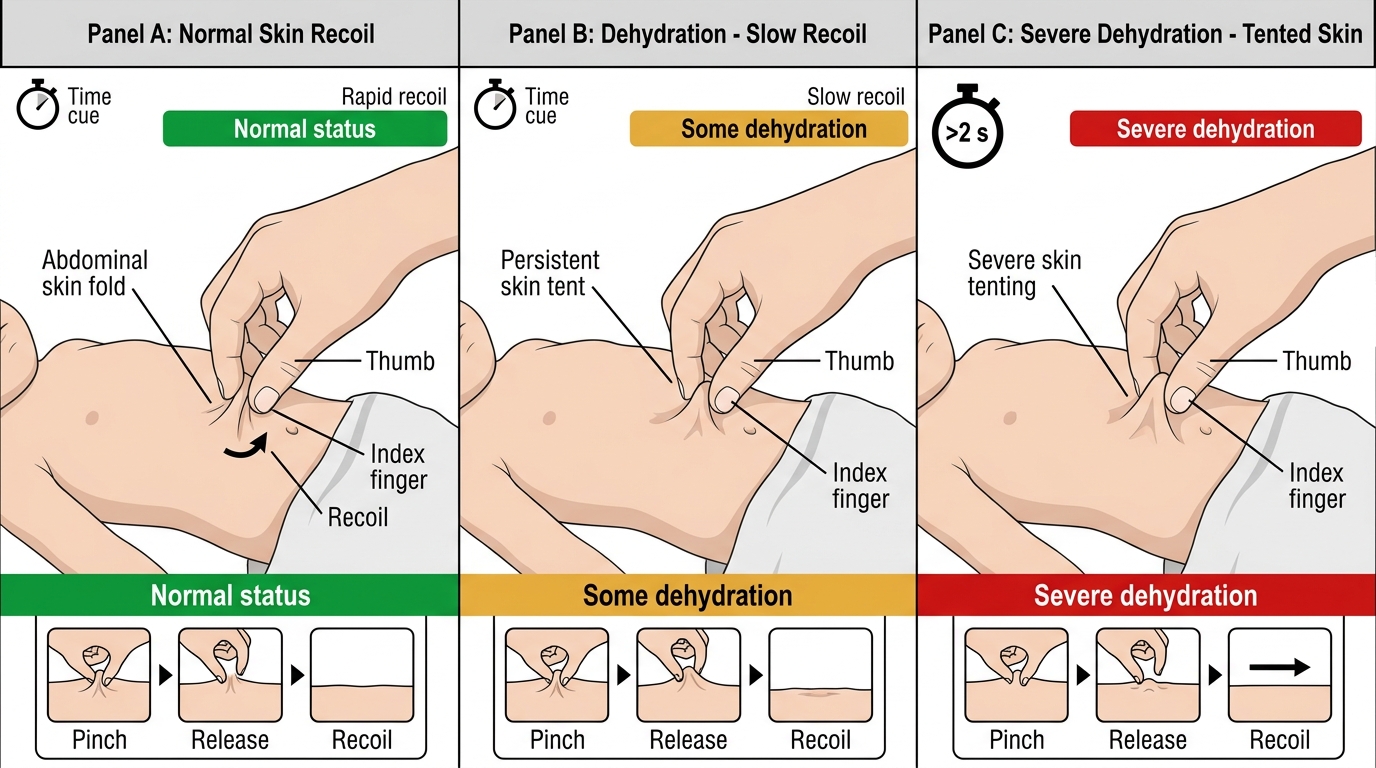
Skin Pinch Test for Pediatric Dehydration
SELF-CHECK
After Phase 1 of Plan C in a 15-month-old (12 kg), reassessment shows: alert, less sunken eyes, skin pinch recoils in 1.5 seconds, drinking some ORS. What is the correct next step?
A. Repeat Phase 1 again (30 mL/kg) — child still has signs
B. Proceed to Phase 2: give 70 mL/kg (840 mL) RL over 2.5 hours and begin ORS 5 mL/kg/hour
C. Stop IV fluids entirely — child is no longer severely dehydrated
D. Switch to Plan B ORS only immediately
Reveal Answer
Answer: B. Proceed to Phase 2: give 70 mL/kg (840 mL) RL over 2.5 hours and begin ORS 5 mL/kg/hour
The child has improved from severe to 'some dehydration' signs (skin pinch slow at 1.5 sec, some oral intake, alert). This means Phase 1 worked — proceed to Phase 2: 70 mL/kg = 70 × 12 = 840 mL RL over 2.5 hours (child ≥12 months). Also begin ORS 5 mL/kg/hour alongside the IV. Phase 1 is not repeated unless severe dehydration signs persist at reassessment.
Supervised Practice: Performing Dehydration Assessment and Calculating Plan C
Dehydration assessment is a hands-on clinical skill that requires practice with real patients under supervision before it can be performed reliably and confidently in an emergency. The theoretical knowledge of IMNCI signs and Plan C calculation is necessary but not sufficient — studies of clinical skill acquisition consistently show that motor skills such as the skin pinch technique and speed-based judgements such as the 2-second recoil threshold require at least ten supervised repetitions before they become automatic. A student who has only read about the skin pinch will hesitate and mistime it under the pressure of an emergency; a student who has performed it on fifty children during a paediatric posting will execute it correctly without conscious effort. The same applies to Plan C calculation: a paediatrician does not derive the formula at the bedside — they have performed the calculation often enough that the volumes are retrieved, not computed. The goal of this section is to provide a structured scaffold for building that automaticity, through a standard technique and worked numerical examples that you should rehearse until the numbers are reflexive.
Provided image
Step-by-step dehydration assessment sequence (perform in this order on every sick child with diarrhoea):
1. Observe the child's level of consciousness before touching: alert/normal (no dehydration), restless/irritable (some), lethargic/unconscious (severe).
2. Look at the eyes: normal position or sunken? Ask the mother: 'Do the eyes look different from usual?'
3. Offer water or ORS in a cup: drinks normally (no dehydration), drinks eagerly/thirsty (some), not able to drink/drinks poorly (severe).
4. Pinch the abdominal skin (two-finger technique at umbilical level): <1 second (no dehydration), 1–2 seconds (some), >2 seconds (severe).
5. Classify using the 'two or more signs' rule: if ≥2 severe signs → severe dehydration (Plan C); if ≥2 some-dehydration signs but not severe → some dehydration (Plan B); if fewer → no dehydration (Plan A).
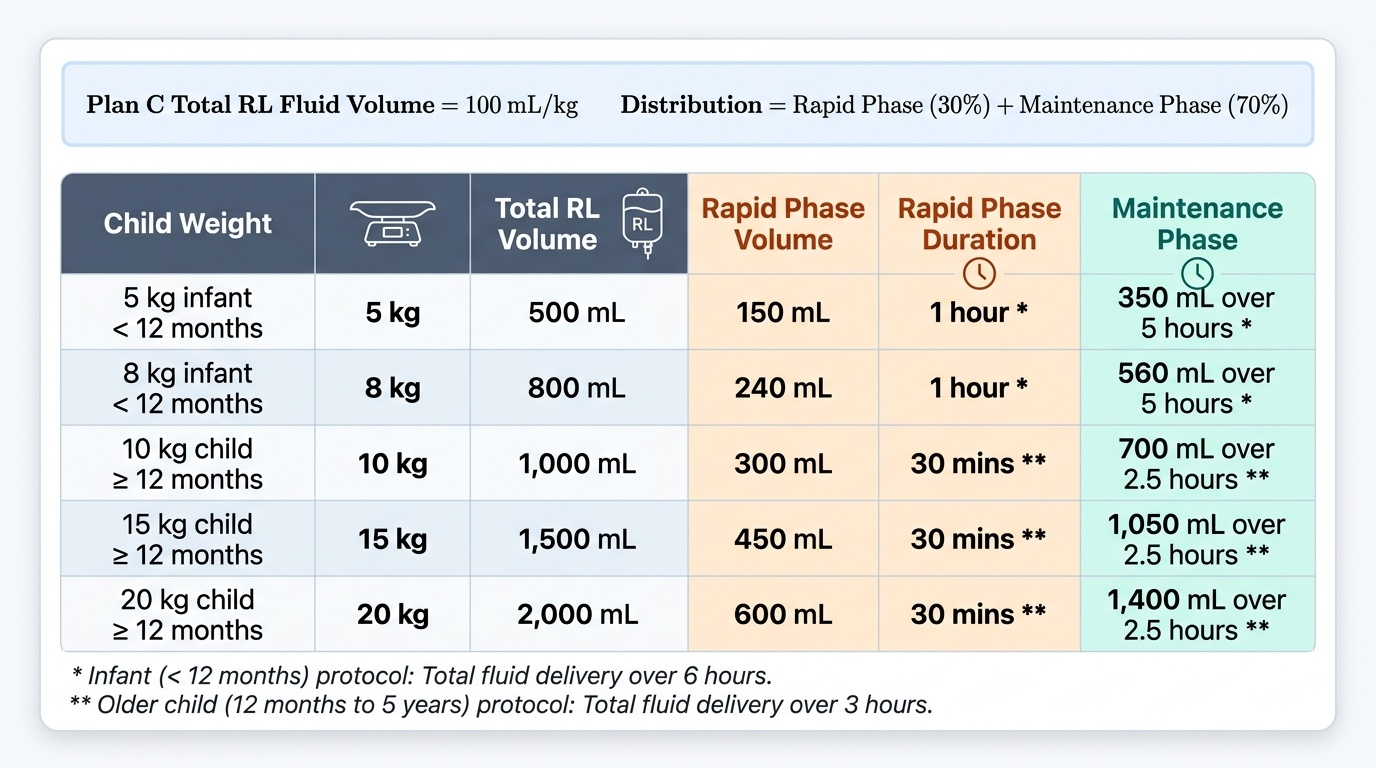
Worked Plan C calculations — practise these until automatic:
Example 1: 9-month-old infant, weight 8 kg, severe dehydration.
• Phase 1: 30 mL/kg = 240 mL RL over 1 hour (infant <12 months)
• Phase 2: 70 mL/kg = 560 mL RL over 5 hours (infant <12 months)
• Total Plan C: 800 mL
Example 2: 2-year-old child, weight 12 kg, severe dehydration.
• Phase 1: 30 mL/kg = 360 mL RL over 30 minutes (child ≥12 months)
• Phase 2: 70 mL/kg = 840 mL RL over 2.5 hours (child ≥12 months)
• Total Plan C: 1,200 mL
Example 3: 11-month-old infant, weight 7.5 kg, severe dehydration.
• Phase 1: 30 mL/kg = 225 mL RL over 1 hour
• Phase 2: 70 mL/kg = 525 mL RL over 5 hours
• Total Plan C: 750 mL
What to document after dehydration assessment:
Classification (no/some/severe), all four IMNCI signs with findings, weight, plan selected, fluid type and volume calculated, start time, Phase 1 completion time, reassessment findings at end of Phase 1.