Page 8 of 31
PE24.{3,12-14} | Shock Emergency — SDL Guide
Learning Objectives
- Describe the aetio-pathogenesis, clinical recognition, and management of shock in children
- Distinguish compensated from decompensated shock using clinical signs: pulse, capillary refill time, blood pressure, and mental status
- Classify shock as hypovolaemic, distributive, cardiogenic, or obstructive and explain the distinguishing features of each
- Check for clinical signs of shock systematically at the bedside
- Secure intravenous and intraosseous access in a simulated environment
- Choose the appropriate fluid type and calculate the correct fluid volume for resuscitation in paediatric shock
INSTRUCTIONS
Shock is the clinical state of circulatory failure resulting in inadequate oxygen delivery to meet cellular metabolic needs. Children have remarkable compensatory mechanisms that mask hypotension until late — making pulse character, capillary refill time, and mental status the clinically useful early indicators. Timely recognition and fluid resuscitation in the first 'golden hour' are the primary determinants of outcome. This module covers the recognition, classification, vascular access, and fluid resuscitation required for paediatric shock management.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 27 — Paediatric Emergencies (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 79 — Shock (textbook)
- AHA PALS Guidelines 2020 — Recognition and Management of Shock (guideline)
- IAP Guidelines on Paediatric Fluid Resuscitation (post-FEAST trial guidance) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-month-old infant is brought to the emergency department with 3 days of profuse watery diarrhoea and vomiting. On examination: she is lethargic and her eyes are sunken. Heart rate 186/min, respiratory rate 52/min. You check her capillary refill time — it is 4 seconds. Her blood pressure is 88/60 mmHg. Her skin is pale and mottled. Is this child in shock? If so, what type, and what do you give first — and how much?
WHY THIS MATTERS
Paediatric shock is the final common pathway of diverse conditions — gastroenteritis, sepsis, trauma, congenital heart disease — and is among the most common causes of paediatric death at the district hospital level in India. The key reason early shock is missed is that children maintain a normal blood pressure until they have lost approximately 25–30% of their blood volume — by which time decompensation is imminent. Recognising compensated shock (before BP falls) requires a trained eye for subtle signs: tachycardia, prolonged capillary refill, cold extremities, and altered behaviour. Fluid resuscitation with the correct volume of the correct fluid, administered rapidly through a correctly placed IV or IO line, is the intervention that prevents progression to cardiac arrest. Every final-year student and intern must be competent in these skills.
RECALL
Before proceeding, recall the following:
• Cardiac output (CO) = heart rate × stroke volume; stroke volume is determined by preload (venous return), afterload (systemic vascular resistance), and contractility. In shock, CO falls — either because HR drops (rare as primary cause), or because stroke volume falls due to decreased preload (hypovolaemia), impaired contractility (cardiogenic), or excessive afterload change (obstructive/distributive).
• Baroreceptor reflex: hypotension → carotid/aortic baroreceptors → sympathetic activation → tachycardia + vasoconstriction. Children have a vigorous baroreceptor reflex, which is why blood pressure is maintained (at the cost of tachycardia and peripheral shutdown) until circulatory reserve is exhausted.
• Oxygen delivery (DO₂) = CO × haemoglobin concentration × oxygen saturation × 1.34. Shock reduces CO → reduces DO₂ → anaerobic metabolism → lactic acidosis.
• Normal HR ranges (approximate): infant <12 months 100–180/min; 1–5 yr 80–160/min; 5–12 yr 70–140/min; adolescent 60–120/min.
Clinical Indication: Recognising Shock in a Child
Shock is defined as a state of acute circulatory failure leading to inadequate delivery of oxygen and substrates to meet tissue metabolic demands. The definition is physiological, not solely haemodynamic — a child can be in shock with a normal blood pressure. This is the central challenge of paediatric shock recognition: hypotension is a late and preterminal sign in children. The vigorous sympathetic compensatory response in children — tachycardia, peripheral vasoconstriction, increased myocardial contractility — maintains blood pressure until approximately 25–30% of blood volume is lost or until the compensatory mechanisms are overwhelmed by ongoing injury or physiological decompensation. The clinician who waits for hypotension to diagnose shock has already missed the optimal intervention window.
Paediatric shock is classified into three phases based on the adequacy of compensation:
Compensated shock: cardiac output is maintained by compensatory mechanisms. Blood pressure is normal for age. Clinical signs: tachycardia (most sensitive early sign), prolonged capillary refill time (>2 seconds), cold extremities, pale or mottled skin, weak peripheral pulses with bounding central pulses, mild agitation or restlessness, slightly reduced urine output.
Decompensated (uncompensated) shock: compensatory mechanisms fail; cardiac output falls; blood pressure drops below the 5th percentile for age. Clinical signs: all of the above PLUS hypotension, depressed mental status (confusion, lethargy, unresponsiveness), absent peripheral pulses, central pulses weak, bradycardia (an ominous pre-arrest sign — indicates the heart itself is failing from hypoxia).
Irreversible shock: prolonged circulatory failure has caused irreversible cellular injury across multiple organ systems. Even with aggressive resuscitation, death is likely. Characterised by profound hypotension, coma, oligoanuria, multiorgan failure.
The most important first step in recognising shock is to ask: 'Is the heart rate elevated for this child's age, and is the perfusion adequate?' Perfusion is assessed by CRT, skin temperature, and mental status — not blood pressure alone.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
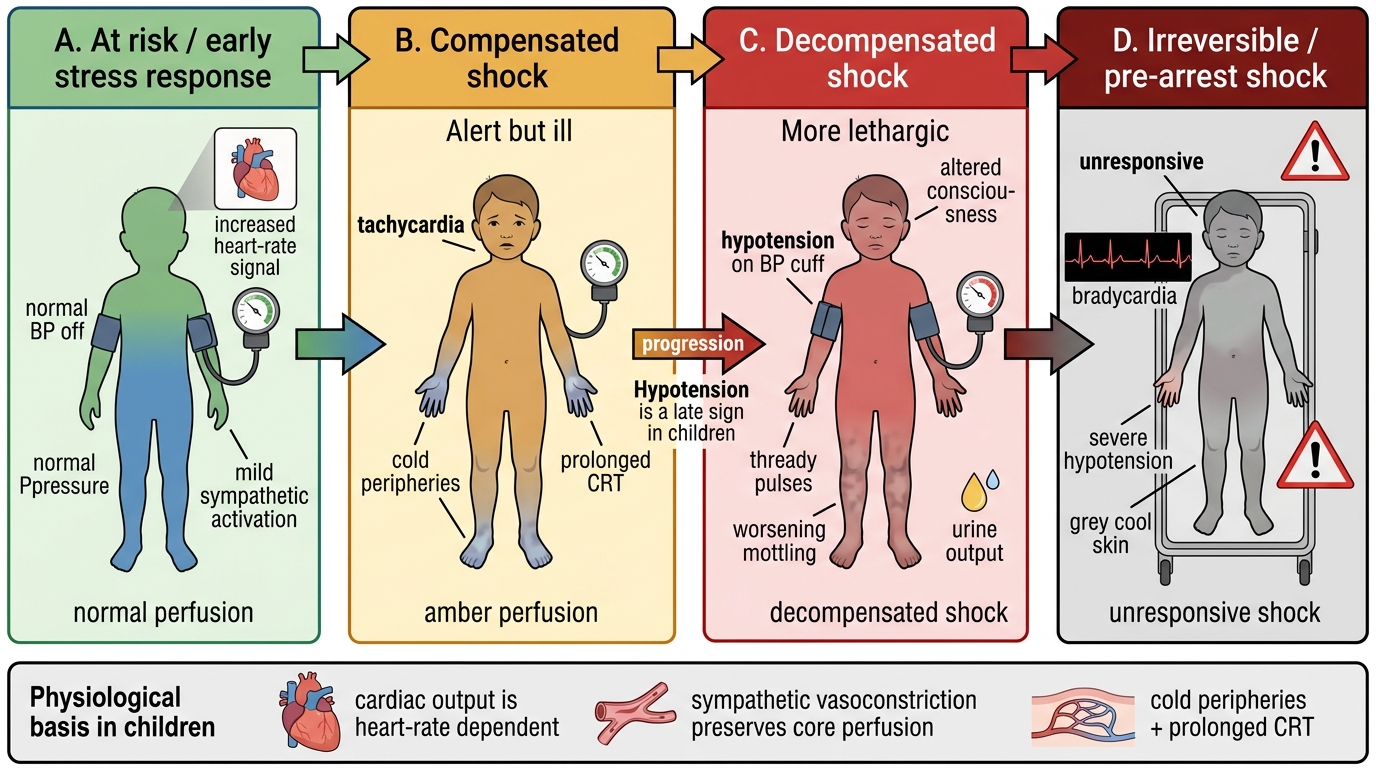
Recognition of Paediatric Shock Progression
Anatomy and Physiological Basis of Paediatric Shock
Children's circulatory physiology confers specific vulnerabilities and compensatory capacities that differ fundamentally from adults. Understanding these differences is essential for interpreting vital signs correctly and for calibrating the urgency of intervention.
Cardiac output is rate-dependent in infants: unlike adults where stroke volume can increase substantially through the Frank-Starling mechanism, infant myocardium is relatively non-compliant and operates near the peak of the Starling curve at baseline. This means that during hypovolaemia or sepsis, infants primarily compensate by increasing heart rate rather than stroke volume. Tachycardia is therefore the earliest, most sensitive, and most reliable indicator of shock in infants and young children — it must always be taken seriously in a sick child, even if BP is normal.
Compensatory vasoconstriction: the sympathetic response to falling cardiac output triggers intense peripheral vasoconstriction, shunting blood from skin, gut, and muscle to preserve perfusion of heart, brain, and adrenal glands. This is why children in compensated shock have cold, mottled extremities despite a warm core, and why CRT is prolonged (capillaries are vasoconstricted). The skin serves as a 'window' on perfusion — a child with warm, well-perfused skin is unlikely to be in significant shock.
Blood volume reference values: total blood volume in children is approximately 70–80 mL/kg (neonates 85–90 mL/kg). A 10 kg child has ~750 mL of blood. A 20% blood volume loss (CLASS II haemorrhagic shock equivalent) = 150 mL — approximately the volume of a standard soft-drink can. This illustrates the narrow margin between compensated and decompensated haemorrhagic shock in small children. Even seemingly small amounts of blood loss (from trauma, surgical complications, or gastrointestinal haemorrhage) can push a child across the compensation threshold.
Age-specific normal vital signs are essential reference points because tachycardia and hypotension are defined relative to age norms:
• Systolic BP lower limit of normal: neonate ≥60 mmHg; infant ≥70 mmHg; 1–10 yr ≈ 70 + (2 × age in years) mmHg; >10 yr ≥90 mmHg
• Upper HR limit of normal: infants <180/min; 1–5 yr <160/min; 5–12 yr <140/min; >12 yr <130/min
• Normal CRT: <2 seconds (measured on the sternum or forehead — more reliable than finger in cold environments)
Classification and Pathophysiology of Shock Types
Understanding the type of shock is essential because each has a distinct pathophysiology and the fluid strategy differs — particularly for cardiogenic shock, where excessive fluid worsens pulmonary oedema. The four major categories of shock are defined by the primary haemodynamic defect. In practice, shock can be mixed (e.g., septic shock has components of distributive, hypovolaemic, and cardiogenic shock), but categorising the dominant mechanism guides initial treatment.
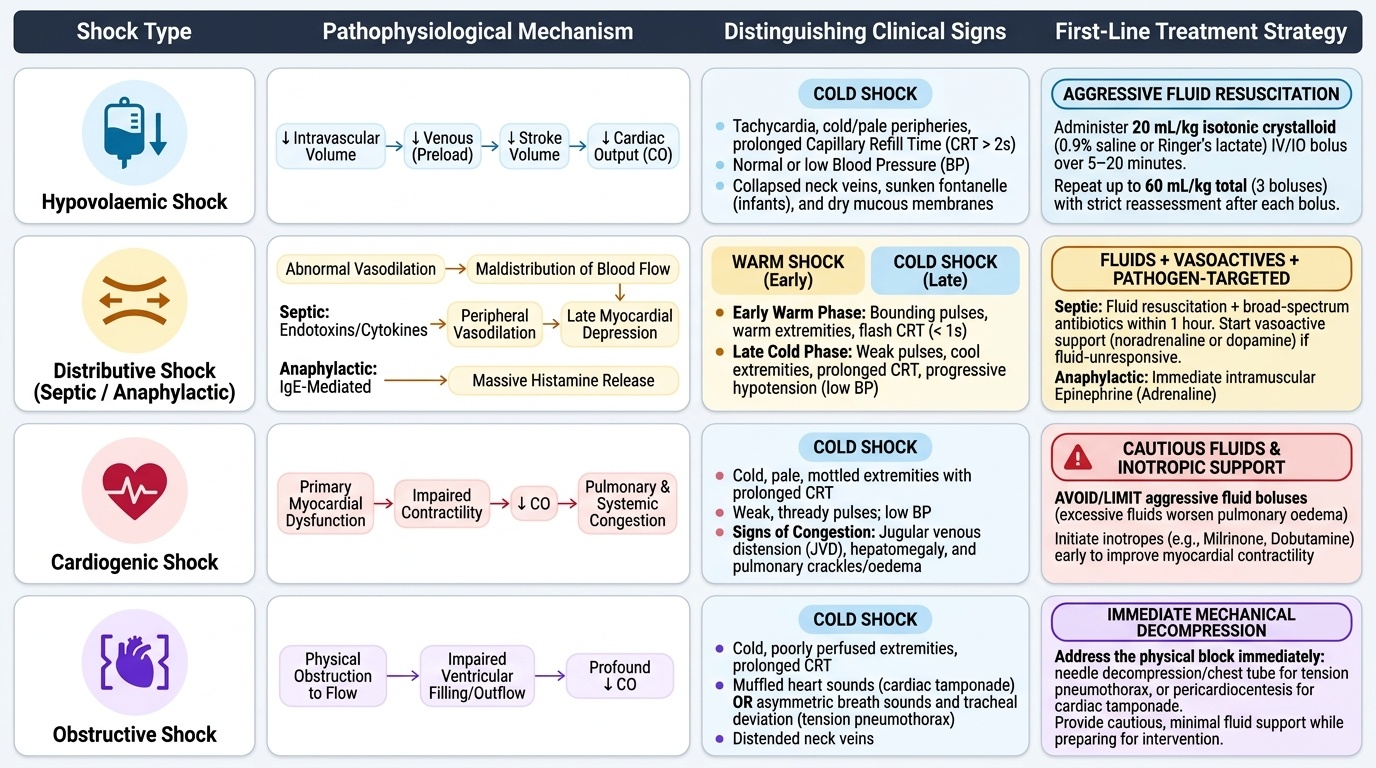
Provided image
Hypovolaemic shock is the most common type in children in India, usually from diarrhoeal dehydration, haemorrhage (trauma, surgical), or internal losses (burns, peritonitis). The mechanism is reduced intravascular volume → decreased venous return → reduced preload → reduced stroke volume → reduced CO. Clinically: tachycardia, cold peripheries, normal or low BP, prolonged CRT, collapsed veins, sunken fontanelle (infants), dry mucous membranes. Treatment: 20 mL/kg isotonic crystalloid (0.9% saline or Ringer's lactate) IV/IO bolus over 5–20 minutes, repeated as needed up to 60 mL/kg total (3 boluses) with reassessment after each bolus.
Distributive shock results from maldistribution of blood flow, usually from abnormal vasodilation. The most important causes in children are:
• Septic shock (most common distributive type): bacterial, viral, or fungal sepsis → endotoxins + cytokines → peripheral vasodilation (warm shock initially — bounding pulses, warm extremities, flash CRT) → myocardial depression → eventual cold shock (poor perfusion). Treatment: fluid resuscitation + broad-spectrum antibiotics within 1 hour + vasopressors (noradrenaline or dopamine) if fluid-unresponsive.
• Anaphylactic shock: IgE-mediated massive histamine release → profound vasodilation + airway oedema. Treatment: adrenaline IM 0.01 mg/kg (max 0.5 mg) as FIRST-LINE treatment; antihistamines and steroids are secondary.
• Neurogenic shock: spinal cord injury above T6 → loss of sympathetic tone → vasodilation + bradycardia (distinguishing from other shock types where bradycardia is a late sign).
Cardiogenic shock results from primary myocardial pump failure. Causes in children: congenital heart disease (obstructed TAPVD, hypoplastic left heart), myocarditis, arrhythmias, post-cardiac surgery. Clinically distinguishable from other shock types by: raised JVP / hepatomegaly (fluid overload signs), gallop rhythm, crepitations at lung bases, cardiomegaly on CXR, low ejection fraction on echo. Fluid resuscitation is cautious: 5–10 mL/kg over 20–30 minutes with cardiac monitoring — excessive fluid worsens pulmonary oedema. Vasopressors (dopamine, dobutamine, adrenaline infusion) are primary treatment.
Obstructive shock results from physical obstruction to cardiac filling or outflow: tension pneumothorax (mediastinal shift, absent breath sounds on one side, tracheal deviation away from affected side), cardiac tamponade (Beck's triad: low BP, elevated JVP, muffled heart sounds; in children, often from haemopericardium after trauma or pericarditis), massive pulmonary embolism (rare in children). Treatment is cause-directed (needle decompression for tension pneumothorax, pericardiocentesis for tamponade) — fluid alone does not reverse obstructive shock.
SELF-CHECK
A 6-year-old child is brought in after a road traffic accident. She is tachycardic (HR 152/min), pale, and has a CRT of 4 seconds. BP is 94/60 mmHg (normal for age). She weighs 20 kg. Which of the following best describes her condition, and what is the appropriate fluid bolus?
A. Decompensated shock; give 400 mL isotonic crystalloid bolus
B. Compensated shock; give 400 mL isotonic crystalloid bolus
C. Compensated shock; give 200 mL isotonic crystalloid bolus
D. No shock; observe and reassess in 30 minutes
Reveal Answer
Answer: B. Compensated shock; give 400 mL isotonic crystalloid bolus
This child has compensated shock: tachycardia, pale skin, and prolonged CRT (4 seconds) indicating poor perfusion — but blood pressure is still normal for a 6-year-old (lower limit ~82 mmHg by 70+2×6). Compensated shock requires urgent fluid resuscitation to prevent progression to decompensated shock. The fluid bolus is 20 mL/kg = 20 × 20 = 400 mL isotonic crystalloid (0.9% saline or Ringer's lactate) IV/IO over 5-20 minutes. Option C (200 mL = 10 mL/kg) is the cautious dose used in neonates, DKA, and cardiogenic shock — not standard hypovolaemic shock in a 6-year-old.