Page 9 of 31
PE24.{3,12-14} | Shock Emergency — SDL Guide (Part 2)
Clinical Assessment: Checking for Signs of Shock
The clinical assessment for shock in a child is a structured, systematic, rapid examination targeting the key indicators of circulatory adequacy. This assessment can be completed in under 60 seconds and does not require any equipment beyond your hands, a watch, and a sphygmomanometer. The PALS 'evaluate-identify-intervene' loop mandates that assessment and intervention occur simultaneously — do not delay fluid resuscitation to complete a full examination. The six-component assessment below should be performed in the order listed, because the pulse assessment provides the most immediate information and takes the fewest seconds; subsequent components add detail and context. Committing this sequence to memory as a procedural routine — rather than a checklist you read — allows you to perform it automatically while simultaneously directing your team to prepare IV access and fluids, which is the standard parallel-tasking approach in paediatric emergency management.
1. Pulse assessment — the single most important first step:
• Rate: count for 15 seconds, multiply by 4; tachycardia is the earliest sign of shock (see age-specific thresholds above). Bradycardia in a shocked child = preterminal sign
• Volume/character: peripheral pulses (radial, dorsalis pedis) — weak/thready = vasoconstriction = poor peripheral perfusion; absent peripheral pulses + weak central pulses = decompensated shock. 'Bounding' central pulses with absent peripherals = early septic warm shock
• Location: in infants, assess brachial pulse (antecubital fossa) — the radial pulse is often impalpable in small infants even normally
2. Capillary refill time (CRT): press the sternum or forehead firmly for 5 seconds, then release and count the seconds until the blanched skin returns to its baseline colour. Normal: <2 seconds. Prolonged (>2 seconds) = reduced peripheral perfusion. Assess on a central site (sternum) rather than the finger — peripheral CRT is unreliable in cold environments.
3. Blood pressure: use the correct cuff size (bladder length 80% of arm circumference; cuff width 40% of arm circumference — too-small a cuff over-reads BP, too-large under-reads). Hypotension confirms decompensated shock but its absence does NOT exclude shock. Interpret BP against age-specific norms.
4. Skin assessment: temperature (warm/cold at what level of the limb?), colour (pink/pale/mottled/cyanosed), moisture (dry in dehydration; clammy in catecholamine response). In septic warm shock, the skin is warm and flushed; in hypovolaemic and cold septic shock, the skin is cool and mottled.
5. Mental status: AVPU scale — Alert, responds to Voice, responds to Pain, Unresponsive. A child who is only Pain-responsive or Unresponsive has significantly reduced cerebral perfusion — this is decompensated shock until proven otherwise.
6. Urine output (if catheterised or nappy weight available): normal ≥1 mL/kg/h in infants, ≥0.5 mL/kg/h in older children; oliguria (<0.5 mL/kg/h) indicates reduced renal perfusion and is an early marker of shock in children old enough to be toilet-trained.
Vascular Access in Paediatric Shock
Rapid vascular access is the enabling step for fluid resuscitation — without it, no drug or fluid can be delivered. In a shocked child, peripheral veins are collapsed and difficult to cannulate due to vasoconstriction. A clear hierarchy of access approaches, with defined time limits, guides the decision to escalate from peripheral IV to intraosseous (IO) access.
Peripheral intravenous (IV) access: the first attempt should always be a peripheral IV, using the largest-bore cannula that fits the vein (typically 22G or 24G in infants, 20G or 22G in older children). Best sites: antecubital fossa (large, straight vein, easy to landmark), dorsum of hand, greater saphenous vein at the medial malleolus, dorsum of foot. In shocked children, the external jugular vein (visible on crying/Valsalva) may be used as a peripheral site. Cannulate with warm skin (wrapping the limb for 60 seconds improves venous distension). Limit: if no access in 90 seconds or after 2 attempts, escalate to IO.
Intraosseous (IO) access is the PALS-recommended alternative when peripheral IV cannot be established within 90 seconds. IO access delivers drugs and fluids directly into the highly vascular bone marrow cavity, which drains into the systemic venous circulation — pharmacokinetics are equivalent to IV access. IO is not a 'last resort'; it is the standard second-line access in a resuscitating child.
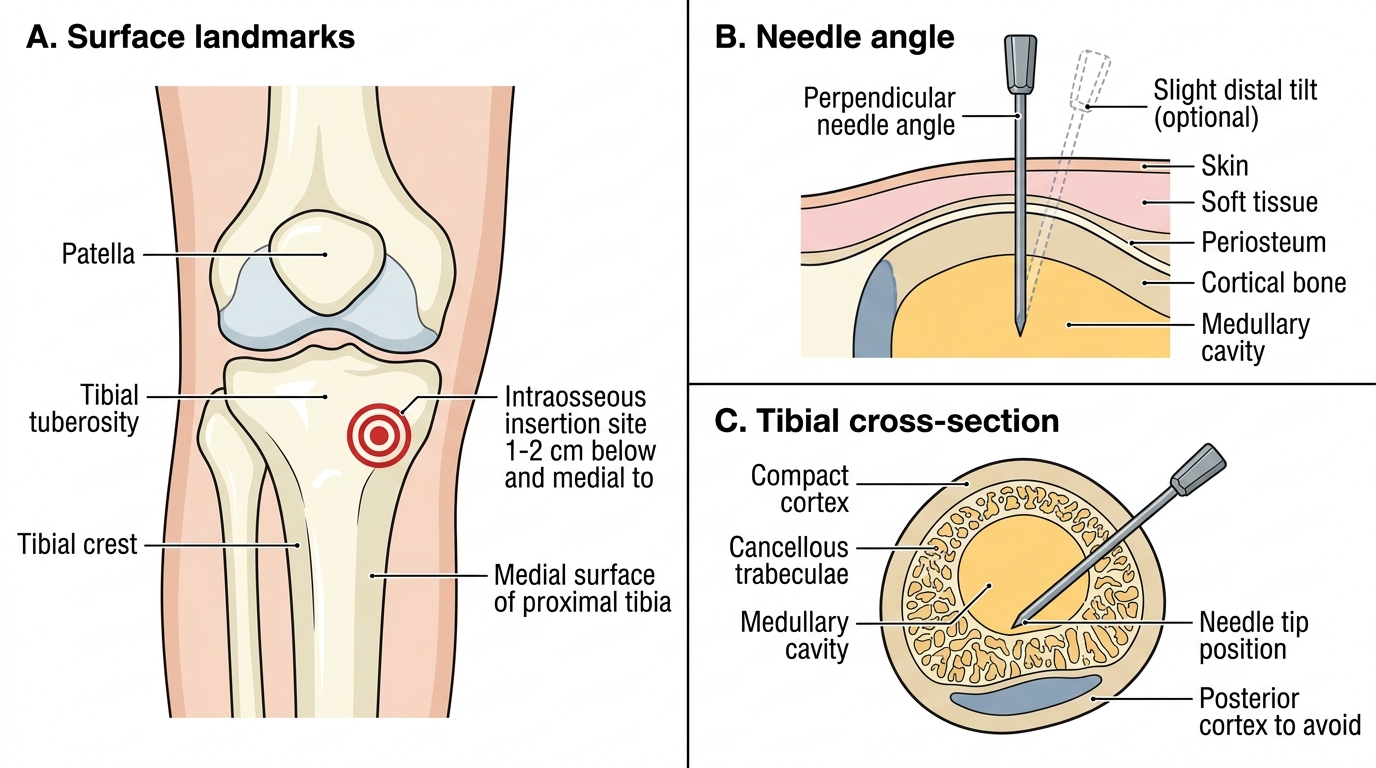
IO technique at the proximal tibia (most common site in children):
1. Position the leg with mild external rotation, slight knee flexion
2. Landmark: tibial tuberosity (the bony prominence below the patella), then move 1–2 cm distal and medial (anteromedial flat surface of the proximal tibia)
3. Clean the site; use lidocaine 1 mg/kg IO in a conscious child (for discomfort of marrow infusion)
4. Insert the IO needle (EZ-IO drill, manual IO needle, or 16–18G bone marrow needle) perpendicular to the bone surface (or with a 5–10° distal tilt in infants to avoid the growth plate)
5. Advance with a twisting/drilling motion until a 'give' is felt as the cortex is penetrated
6. Confirm position: needle stands upright without support, marrow aspirate obtained, flush 5–10 mL saline easily (no subcutaneous swelling)
7. Secure with tape; fluids and drugs given under pressure if needed (manual push or pressure bag)
Other sites: distal femur (infants — useful when tibial site is unavailable), distal tibia (just proximal to medial malleolus), humeral head (older children/adults). Sternal IO (used in adults) is NOT used in children — the sternum is too thin.
Central venous access (femoral vein, internal jugular, subclavian) provides reliable high-flow access but is time-consuming and carries higher complication risk; used when peripheral IV and IO both fail, or for ongoing vasopressor infusion in the PICU setting.
Proximal Tibial Intraosseous Needle Insertion
CLINICAL PEARL
Tachycardia is a symptom, not a diagnosis. In a sick child, a heart rate of 180/min is shock until proven otherwise. Do not dismiss tachycardia as 'fever' or 'anxiety' without checking CRT and perfusion. The child who is febrile AND tachycardic beyond what the temperature alone explains needs a fluid bolus and sepsis workup.
The FEAST trial changed our approach to routine fluid boluses. In sub-Saharan African children with febrile illness (predominantly malaria and anaemia), 20 mL/kg fluid boluses increased 48-hour mortality compared to no bolus. This was because rapid fluid loading in profoundly anaemic children (Hb <5 g/dL) worsened outcome. The Indian IAP/WHO guidance therefore recommends caution before giving fluid boluses in children with known or suspected severe anaemia or malaria — reassess the haemoglobin and consider blood transfusion rather than crystalloid bolus in these situations. This does NOT apply to standard hypovolaemic or septic shock in well-nourished children without severe anaemia.
Fluid Resuscitation: Choosing and Calculating
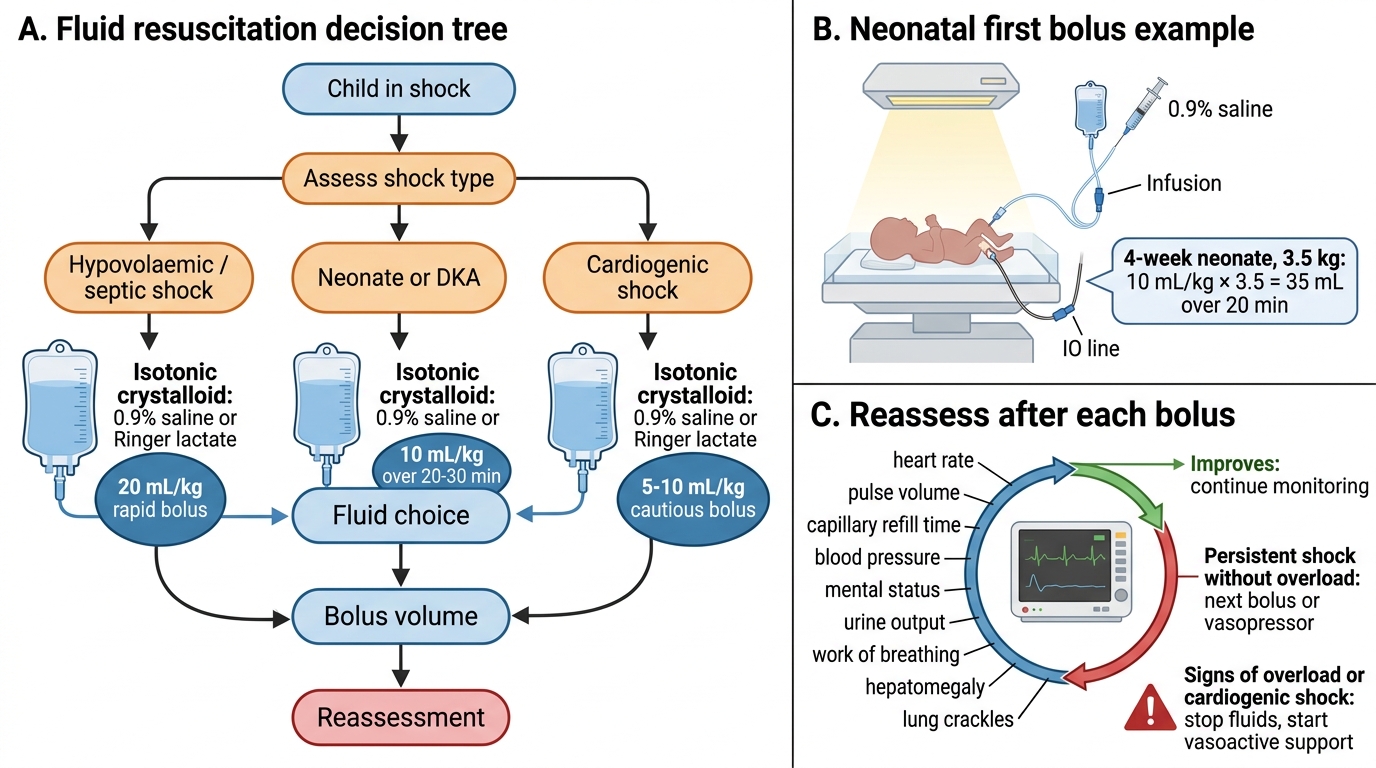
Fluid resuscitation is the cornerstone of shock management for all types except cardiogenic and obstructive shock. The choice of fluid type, volume, and rate of administration must be individualised based on the aetiology of shock, the child's age, and the clinical context. Getting the volume calculation wrong is a high-stakes error — both under-resuscitation (perpetuating shock) and over-resuscitation (pulmonary oedema, cerebral oedema in DKA) cause harm. The principles that govern fluid selection are straightforward once the underlying physiology is understood: the goal is to expand the intravascular compartment rapidly, which requires a fluid whose tonicity keeps it in the vascular space rather than redistributing into cells or interstitium. Isotonic crystalloid meets this criterion; hypotonic fluids do not. The volume exceptions (10 mL/kg for neonates and DKA; 5-10 mL/kg for cardiogenic shock) exist because the pathophysiology of those situations makes the cardiac or cerebral systems susceptible to harm from rapid volume loading, not because the principle of fluid replacement is different.
Fluid type selection:
• Isotonic crystalloid (0.9% normal saline or Ringer's/Hartmann's lactate) is the first-line fluid for hypovolaemic, distributive (septic/anaphylactic), and neurogenic shock. Ringer's lactate is preferable for large-volume resuscitation as it avoids hyperchloraemic acidosis (excess chloride from large-volume NS can cause a metabolic acidosis). Both are acceptable for initial boluses.
• Blood / packed red blood cells (pRBC): indicated for haemorrhagic shock when the estimated blood loss exceeds 30–40% blood volume, or when the child fails to respond to 2–3 crystalloid boluses. Target Hb >7 g/dL in most children; higher (>8–9 g/dL) in cardiogenic or respiratory compromise.
• 5% albumin or other colloids: not recommended as first-line for shock resuscitation in children (no evidence of benefit over crystalloid; SAFE trial and FEAST trial data).
• Avoid hypotonic fluids (0.45% saline, dextrose-saline) for resuscitation boluses — they distribute into the intracellular space rather than remaining in the intravascular compartment, worsening hyponatraemia and cerebral oedema risk.
Volume and rate — the standard approach and exceptions:
| Clinical context | Volume per bolus | Rate | Notes |
|---|---|---|---|
| Hypovolaemic/septic/anaphylactic shock (most children) | 20 mL/kg | Over 5–20 min IV/IO push | Reassess after each; repeat up to 60 mL/kg total |
| Neonates (any shock type) | 10 mL/kg | Over 20–30 min | Smaller reserve; risk of NEC and IVH with rapid expansion |
| DKA (any age) | 10 mL/kg | Over 20–30 min | Cerebral oedema risk with rapid expansion |
| Cardiogenic shock | 5–10 mL/kg | Over 20–30 min; cardiac monitoring | Risk of pulmonary oedema; add inotrope if no response |
| Severe anaemia (Hb <5 g/dL) | Transfuse, not crystalloid bolus | Slowly | FEAST trial evidence — avoid large crystalloid bolus |
Calculating the bolus volume: Dose (mL/kg) × weight (kg) = volume in mL.
Example: standard 20 mL/kg for a 14 kg child with septic shock = 280 mL of Ringer's lactate given over 10–15 minutes IV/IO.
Reassessment after each bolus is mandatory before repeating: check HR (should decrease toward normal), CRT (should shorten toward <2 s), BP (should rise if previously low), mental status (should improve), and breath sounds (rule out pulmonary oedema from over-resuscitation). If the child does not respond after 60 mL/kg (3 boluses), the shock is likely fluid-unresponsive — add vasopressors and call for PICU support.
Pediatric Shock Fluid Resuscitation Decision Tree
SELF-CHECK
A 4-week-old neonate (weight 3.5 kg) is brought in with poor feeding, mottled skin, and HR 196/min. You assess the baby as being in shock. You have secured IO access. What is the correct first fluid bolus?
A. 70 mL of 0.9% saline over 5 minutes
B. 35 mL of 0.9% saline over 20 minutes
C. 35 mL of 5% dextrose over 20 minutes
D. 70 mL of Ringer's lactate over 10 minutes
Reveal Answer
Answer: B. 35 mL of 0.9% saline over 20 minutes
In neonates, the standard fluid bolus is 10 mL/kg (not 20 mL/kg) given more slowly over 20-30 minutes. For a 3.5 kg neonate: 10 mL/kg × 3.5 = 35 mL. The fluid should be isotonic (0.9% normal saline or Ringer's lactate) — NOT 5% dextrose, which is hypotonic and distributes intracellularly rather than expanding the intravascular space. 70 mL (20 mL/kg) over 5 minutes is the standard paediatric approach, not appropriate for neonates who have a smaller cardiac reserve and risk of intraventricular haemorrhage with rapid fluid expansion.