Page 7 of 23
PE25.3 | Acute Laryngotracheobronchitis — SDL Guide
Learning Objectives
- Explain the etio-pathogenesis of acute laryngotracheobronchitis including the role of parainfluenza virus and subglottic anatomy
- Describe the clinical features of croup including barking cough, inspiratory stridor, and hoarse voice
- Apply the Westley Croup Score to categorise severity as mild, moderate, or severe
- Identify the radiological steeple sign on AP neck X-ray and distinguish it from the thumbprint sign of epiglottitis
- Select appropriate management for each severity category including weight-based dexamethasone dosing and nebulised adrenaline, with awareness of the rebound phenomenon
INSTRUCTIONS
Croup (acute laryngotracheobronchitis) is the most common cause of acute stridor and upper airway obstruction in children aged 6 months to 3 years. It is a highly characteristic clinical syndrome — the barking, seal-like cough is one of the most distinctive sounds in paediatric medicine and is pathognomonic once heard. Understanding the anatomical basis for its severity, how to score it, and when escalation is needed will equip you to manage this condition confidently from the outpatient clinic to the paediatric emergency unit.
References
- Ghai Essential Pediatrics, 9th ed., Ch 17 — Croup (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 412 — Croup (textbook)
- IAP Guidelines on Management of Croup in Children (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 AM. A mother rushes her 18-month-old son to the emergency department in a panic. He woke from sleep crying, and when she picked him up, she heard a strange, harsh barking sound with each cough — 'like a seal,' she says. He now has noisy breathing when he breathes in. He had a mild runny nose and low-grade fever yesterday but seemed otherwise well. On examination, his temperature is 38.2°C, there is inspiratory stridor audible at rest, and mild subcostal retractions. He is alert, maintaining oxygen saturation at 97%. How do you assess the severity and what do you do next?
WHY THIS MATTERS
Croup is the most common cause of acute stridor in children and the condition most frequently responsible for the terrifying experience of watching a child struggle to breathe. In India, parainfluenza-driven croup peaks in autumn and early winter, presenting primarily in children under three years. Most cases are mild and self-limiting, but moderate-to-severe croup causes genuine respiratory distress and can progress to respiratory failure if not recognised and treated. The availability of a single oral dose of dexamethasone — inexpensive, effective, and easy to administer — makes croup one of the most rewarding acute conditions to treat: a well-managed case goes home the same night. Knowing the Westley score, the correct steroid dose, and the rebound rules for nebulised adrenaline are the three practical skills this module delivers.
RECALL
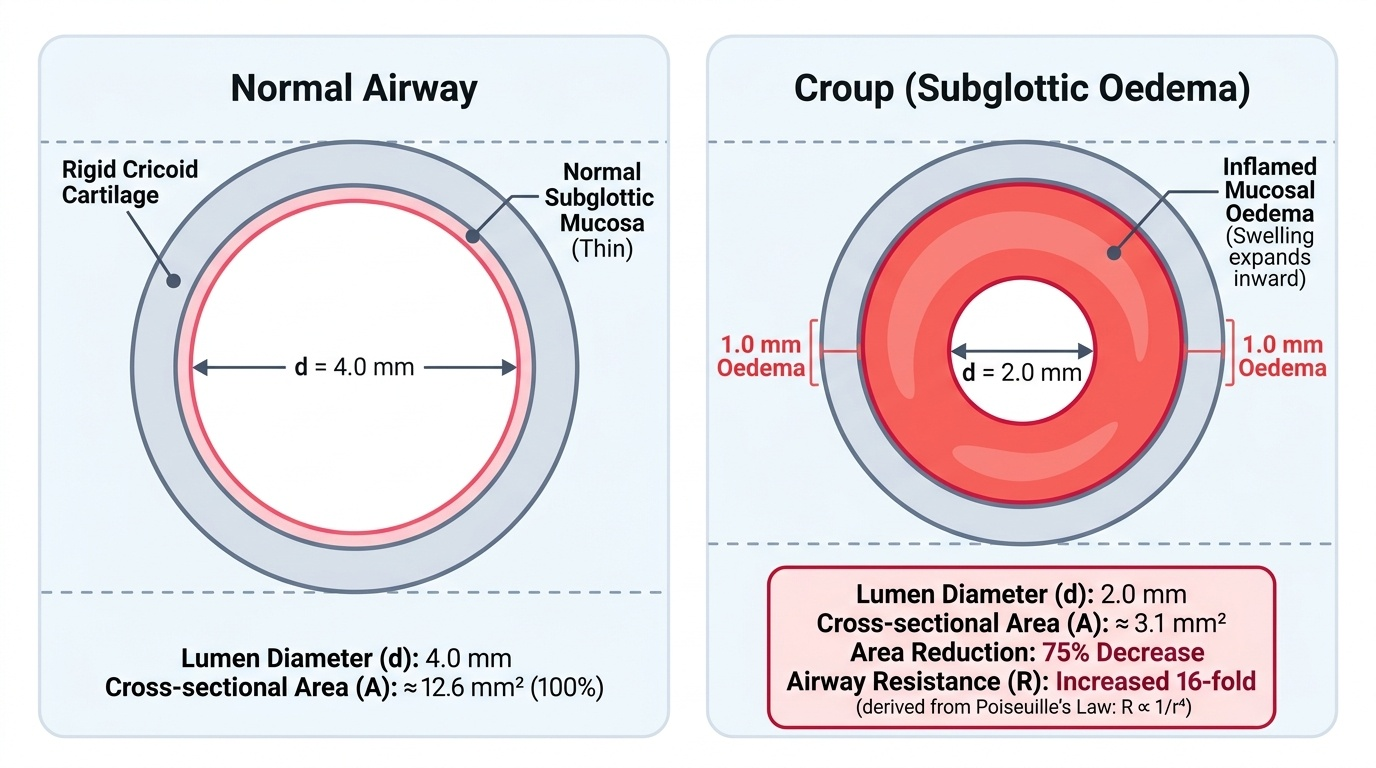
Recall from your anatomy of the larynx that the cricoid cartilage forms a complete cartilaginous ring (unlike the C-shaped tracheal rings below it), making the subglottic space beneath the vocal cords the narrowest fixed segment of the paediatric airway. This anatomical fact is critical to understanding why subglottic oedema in an infant causes such disproportionately severe obstruction. Poiseuille's law states that airway resistance is inversely proportional to the fourth power of the radius (R ∝ 1/r⁴): in an infant whose normal subglottic diameter is 4 mm, a 1 mm circumferential oedema reduces the radius by 50%, increasing resistance 16-fold. The same 1 mm oedema in an adult (subglottic diameter ~10 mm) causes only modest resistance increase. This is why croup produces profound airway compromise in infants at oedema magnitudes that would be trivial in adults.
Clinical Presentation of Croup
Croup typically affects children aged 6 months to 3 years, with a peak incidence around 18 months. The condition follows a characteristic temporal pattern that begins with 1-3 days of an upper respiratory tract infection prodrome — coryza, low-grade fever, and mild rhinorrhoea — followed by the abrupt (often nocturnal) onset of the distinctive croup syndrome. The nocturnal worsening is a consistent and diagnostic feature, explained by the combination of recumbency (increasing secretions pooling at the subglottis) and the circadian trough in endogenous cortisol levels (less anti-inflammatory suppression). The combination of a recognisable prodrome, a distinctive cough, and a predictable time-of-day pattern makes croup one of the most diagnostically reliable syndromes in paediatric emergency medicine — provided the clinician knows what they are listening for.
Provided image
The cardinal clinical triad of croup is:
- Barking ("seal-like") cough — the single most characteristic sign; a harsh, brassy, low-pitched cough resembling a seal bark or a dog's bark; caused by vibration of the inflamed subglottic mucosa; unmistakable once heard
- Hoarse voice — the inflamed vocal cords produce a rough, husky voice (distinct from the hot-potato muffled voice of epiglottitis); in severe cases the child may be aphonic
- Inspiratory stridor — a harsh, high-pitched noise on inspiration, produced by turbulent airflow through the narrowed subglottis; stridor at rest indicates moderate-severe disease (at rest = worse than stridor only on exertion)
Additional features: low-grade fever (rarely >39°C), mild tachycardia, subcostal and intercostal retractions (in moderate-severe disease), and nasal flaring. The child is usually alert and interactive (unlike the toxic, anxious child of epiglottitis). There is no drooling, no dysphagia, and no tripod position — three features that distinguish croup from epiglottitis immediately.
Spasmodic croup is a recurrent variant without an infectious prodrome, occurring in atopic children, often triggered by allergens or viral exposure; clinically identical to infectious croup but resolves faster and recurs.
Pathophysiology and Aetiology
The pathophysiology of croup begins with viral infection of the upper respiratory epithelium and proceeds through an inflammatory cascade that culminates in the characteristic subglottic narrowing. Unlike epiglottitis, where bacteraemia seeds the supraglottis haematogenously, croup is driven by direct viral invasion of the mucosal lining of the larynx, trachea, and bronchi (hence laryngo-tracheo-bronchitis). The virus triggers mucosal oedema, inflammatory cell infiltration, and increased mucus secretion, which together produce the narrowed, inflamed subglottis responsible for all clinical manifestations.
Aetiological agents (most to least common):
Parainfluenza viruses collectively account for the large majority of croup cases. The seasonal pattern — autumn and early winter peaks — mirrors the transmission dynamics of these respiratory pathogens in the community. In infants under 12 months, RSV plays a proportionally larger role than in older children, and these younger infants also tend to have more severe disease due to their smaller airway calibre. The vast majority of croup is therefore viral and self-limiting, which is why antibiotics play no role in its standard management. Bacterial causes, when they occur, produce a far more toxic picture (bacterial tracheitis) that fails to respond to the standard croup regimen and requires IV antibiotics and often intubation.
- Parainfluenza virus types 1 and 2 — responsible for approximately 75% of cases; type 1 is the single most common agent; type 2 is associated with slightly more severe disease; peak incidence autumn-early winter
- Respiratory syncytial virus (RSV) — important cause, especially in infants under 12 months; tends to also cause bronchiolitis
- Influenza A and B — can cause croup; influenza-associated croup tends to be more severe
- Adenovirus, human metapneumovirus — less common
- Mycoplasma pneumoniae — occasional atypical bacterial cause
Differential diagnoses to distinguish from croup:
- Epiglottitis — supraglottic, bacterial (Hib or post-vaccine organisms), rapid onset, drooling, thumbprint sign; managed as described in the preceding SDL
- Bacterial tracheitis (pseudomembranous croup) — rare, caused by S. aureus; mimics croup but is toxically ill, fails to respond to nebulised adrenaline, requires airway management + IV antibiotics
- Foreign body aspiration — sudden onset without prodrome, unilateral wheeze, asymmetric air entry; no fever; requires bronchoscopy
- Subglottic haemangioma — infants <6 months with recurrent stridor; cutaneous haemangiomas may be a clue
- Angioedema — rapid onset, urticarial rash, exposure history; managed as anaphylaxis
Assessment and Severity Scoring
Severity assessment is the pivot point of croup management — every treatment decision (outpatient vs admission, oral vs nebulised therapy, steroid dose) flows from the severity category. The Westley Croup Score is the validated, universally recommended scoring tool for croup severity. It scores five clinical parameters, each of which captures a different dimension of the child's respiratory compromise. A total score of 0-17 is possible; clinically, scores above 11 are rare. The score should be reassessed after each intervention to guide further management decisions. Importantly, the score captures the child's status at a single point in time — serial scoring is more informative than a single measurement, and a rapidly worsening score is more alarming than a static moderate score. Every student should be able to calculate the Westley score at the bedside without a chart, since the five parameters are straightforward clinical observations. The score also provides a common language between clinicians handing over care: saying 'Westley 5, improving after adrenaline' conveys far more than 'moderate croup, treated.'
Provided image
Westley Croup Score:
| Parameter | Score 0 | Score 1 | Score 2 | Score 3 | Score 4 | Score 5 |
|---|---|---|---|---|---|---|
| Stridor | None | At rest with stethoscope | At rest without stethoscope | — | — | — |
| Retractions | None | Mild | Moderate | Severe | — | — |
| Air entry | Normal | Decreased | Markedly decreased | — | — | — |
| Cyanosis | None | — | — | — | With agitation | At rest |
| Level of consciousness | Normal | — | — | — | Depressed | — |
Score interpretation:
- Mild (total <3): Barking cough only, no stridor at rest, no retractions — manage at home with a single oral dose of dexamethasone
- Moderate (total 3-7): Stridor at rest, mild-moderate retractions, normal O₂ saturation — hospital care with nebulised adrenaline + dexamethasone; observe ≥2-4 hours post-nebulisation
- Severe (total ≥8): Marked retractions, decreased air entry, cyanosis or altered consciousness — ICU/HDU admission; may require intubation
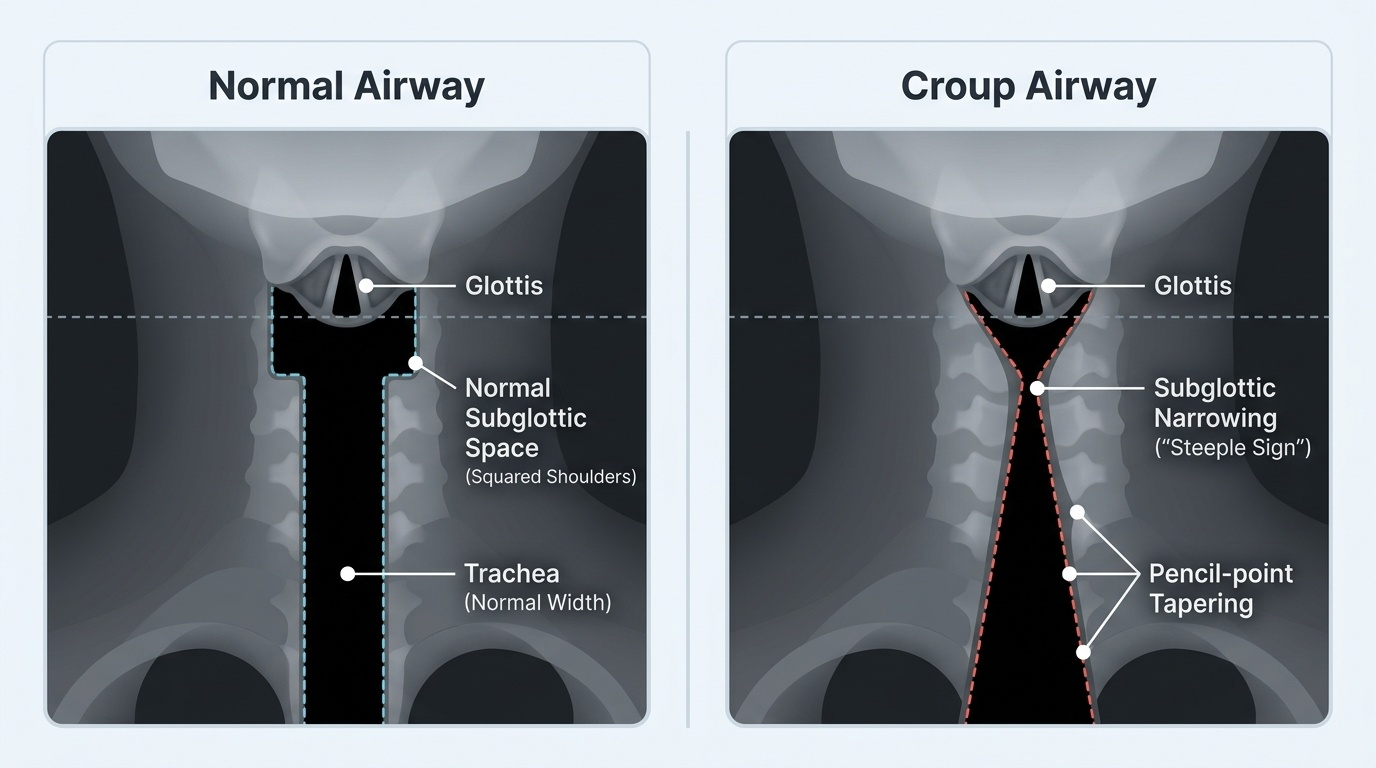
Radiological finding — Steeple sign:
The AP (anteroposterior) neck or chest X-ray may show the steeple sign (also called the pencil-point sign): the normal shoulder-shaped subglottic profile is replaced by a symmetric narrowing of the subglottic column, creating a pointed or steeple-like shape below the vocal cords. This reflects the subglottic mucosal oedema seen in croup. However, the steeple sign is present in only 50-60% of cases and its absence does NOT exclude croup — the diagnosis remains clinical. Note: the X-ray for croup is AP (anteroposterior); the X-ray for epiglottitis is lateral.
SELF-CHECK
An 18-month-old has inspiratory stridor audible at rest, mild subcostal retractions, normal air entry bilaterally, and is alert and conscious. Temperature is 38.2°C, SpO₂ 97%. What is his Westley Croup Score and what is the appropriate management?
A. Score 1 (mild) — discharge home with humidified air, no medication needed
B. Score 4 (moderate) — oral dexamethasone 0.15 mg/kg and observe at home if improving
C. Score 4 (moderate) — nebulised adrenaline + dexamethasone 0.6 mg/kg, observe ≥2-4 hours
D. Score 8 (severe) — immediate ICU admission and prepare for intubation
Reveal Answer
Answer: C. Score 4 (moderate) — nebulised adrenaline + dexamethasone 0.6 mg/kg, observe ≥2-4 hours
Stridor at rest without stethoscope = 2, mild retractions = 1, normal air entry = 0, no cyanosis = 0, alert = 0 → Westley score = 3 (moderate, threshold ≥3). Moderate croup requires nebulised adrenaline (for immediate relief) PLUS dexamethasone 0.6 mg/kg (for sustained effect). Observation for at least 2-4 hours after nebulised adrenaline is mandatory because of the rebound phenomenon — symptoms can return once the adrenaline effect wanes. Discharge home is appropriate only once stridor at rest has resolved and the child is stable for ≥2-4 hours post-nebulisation. The higher dexamethasone dose (0.6 mg/kg) is used for moderate-severe; 0.15 mg/kg is sufficient for mild croup.